
Abstract
Sexual and gender-based violence (SGBV) is a leading cause of physical, emotional, and psychosocial problems around the world, with many countries in East Africa having rates above the global average. Despite the high prevalence in the region, service provision for post-SGBV care is often poorly funded, difficult to access, or simply nonexistent. This review reports the findings of a scoping review of literature from East Africa. The goals of this research were to evaluate existing service provision practices throughout the region, understand how provider bias may affect service provision, and compare existing practices to national policies and internationally agreed human rights treaties. This review identified 54 academic papers and reports through a search of electronic databases and grey literature sources, and four main themes emerged: (1) current models of service provision are inadequate to address the medical and psychosocial needs of survivors; (2) countries are not providing sufficient funding for services; (3) further research is needed into how to incorporate SGBV care into existing health systems and align with international human rights treaties; and (4) there is limited research in many countries in East Africa. The findings are likely to be of use to policy makers, nongovernmental organizations, and service providers working in the medical, legal, and justice systems.
Keywords
Introduction
Sexual and gender-based violence (SGBV) encompasses several types of violent behavior perpetrated against the will of victims (including women, girls, men, boys, and LGBTQI+ people) that can lead to serious bodily harm or even death (ICRC, 2022; Médecins Sans Frontieres [MSF], 2021). Gender-based violence (GBV) refers to harmful acts directed against a person based on their gender (UNHCR, 2021b). Harmful acts include emotional, psychological, and physical abuse, as well as sexual violence (SV). While SGBV can be perpetrated by and against anyone, perpetrators are primarily men, and victims are largely women and girls (UNHCR, 2021a, 2021b; WHO, 2021b). For example, worldwide, 35% of women have experienced at least one form of SGBV, such as intimate partner violence (IPV) or non-partner SV, and 15 million girls have experienced forced sex (The World Bank, 2019; UN, 2021).
This paper focuses on SGBV in East Africa, one of the UN regions with the highest rates of lifetime SGBV in the world (WHO, 2021b). SGBV is a significant contributor to morbidity and mortality in East Africa (Amenu & Hiko, 2014) and is a major obstacle to achieving Sustainable Development Goal 5, which concerns achieving gender equality in all its forms. Around the world, including in East Africa, SGBV can cause lasting physical health consequences, such as injuries and sexually transmitted infections, mental health impacts, such as depression and anxiety, and social consequences, such as stigma and social rejection (WHO, 2021a). Injuries from SGBV can include stab wounds, fractures, vaginal fistulas, and bleeding, and victims may become pregnant (MSF, 2021). Furthermore, female SV victims are twice as likely to have an abortion across their lifespan than their counterparts (MSF, 2021). In many countries that have the highest rates of SGBV worldwide, abortion is illegal, and women frequently seek out unsafe procedures that can cause infections or even death (MSF, 2021). Against this backdrop of human suffering in East Africa, there is an urgent need to synthesize research on SGBV in this region.
Toward this end, we conducted a scoping review of the literature on SGBV medical and legal service provision practices in East Africa. Our goals in conducting the review were to: (1) describe SGBV service provision throughout the region; (2) understand how provider bias may affect service provision; and (3) compare existing practices to national policies and internationally agreed human rights treaties that outline the medical and/or legal services that SGBV survivors are entitled to receive. The review analyzed papers that focused on peacetime SGBV. 1 This allows for determining the level of services that survivors receive in the absence of conflict, wherein service disruption may not be entirely, if at all, under state control. In the sections that follow, we provide an overview of policy and treaties concerning SGBV, the types of services SGBV survivors may be entitled to receive, and research on service delivery in East Africa, as well as outline considerations that arise in the care of the large populations of refugees in the region.
SGBV Survivors’ Rights to Medicolegal Service Provision
The WHO (2015) report on strengthening the medical and legal response to SGBV highlights the importance of involving multiple sectors, including the police, forensic medicine, health and social service agencies, and the judiciary. Moreover, typical steps along the medical and legal service provision pathway include gathering evidence and documenting the crime, addressing a victim’s medical needs, referring victims to the police, carrying out a forensic medical exam, and connecting victims to sustained psychosocial support services. The report lays out the key principles of best practice service provision: prioritizing victims’ physical and emotional safety, keeping information confidential, ensuring that victims are not discriminated against by agencies and organizations, and respecting the victims’ rights and wishes (WHO, 2015). However, SGBV survivors are frequently stigmatized and face gender bias from providers on the pathway, which may discourage help seeking (WHO, 2015).
Policies in East African countries on SGBV service provision are scarce, as explained later in this review, while existing policies outlining services that survivors should receive may not be actioned or enforced (Ajema et al., 2011). To counter this, the Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa, otherwise known as the Maputo Protocol, was written. The Maputo Protocol covers SGBV at length, including female genital mutilation (FGM) and underage marriage as well as stigma and bias against SGBV victims (African Union, 2003). Signatories vow to enforce change through policy action or administrative decision making. However, while multiple countries in the East African region are signatories to international human rights and global health treaties regarding SGBV-related service provision, like the Maputo Protocol, there are reports that survivors in these countries still find it difficult or impossible to access services (Rockowitz et al., 2021b).
Refugee Service Provision
Countries in East Africa host large refugee populations, which further complicates SGBV medical and legal service provision. People living in emergency and humanitarian contexts are at a high risk of SGBV, including FGM, socioeconomic abuse, and denial of reproductive health choices (Muuo et al., 2020). Humanitarian emergencies also make the delivery of adequate care for SGBV survivors difficult and increase the vulnerability of survivors to future victimization (Muuo et al., 2020). This is partially because refugees may be offered services within camps from external organizations with foreign staff, such as the UN, rather than medical or legal professionals from the country they are seeking refuge in. This camp context may not be an indicator of the status of wider service provision throughout the country, but this population nevertheless makes up a percentage of East African residents and we felt it was important to explore their experience in care-seeking. Additionally, even when refugees are living outside of camps, they face unique barriers to healthcare that their local neighbors do not experience, such as discrepancies in cost of healthcare between refugees and locals, and documentation requirements for treatment (Jemutai et al., 2021). Papers that include the experiences of refugees were included in the review given these considerations.
Present Study
In sum, this paper reviews the range of SGBV research activity on East Africa that has taken place, and identifies knowledge gaps, which is one of the key pillars of a scoping review (Levac et al., 2010; Munn et al., 2018). Our aim is to stimulate research that addresses critical knowledge gaps by highlighting topics and countries where research has been most lacking. Furthermore, this review evaluates whether practice models are compliant with national policies and international treaties. The review also considers what is known about the impact of services on victim health and well-being and highlights barriers in accessing and delivering medical and legal services. To examine provider bias, the review captures research whether beliefs about gender equality (e.g., believing that a husband has the right to abuse his wife, or that SV is to be expected in society) on the part of practitioners affects quality of care.
Method
We followed the steps outlined by Arksey and O’Malley (2005) and advanced by Levac et al. (2010), including identifying the research question, finding relevant studies, selecting studies, charting the data, and synthesizing and reporting the results (Levac et al., 2010).
Research Questions and Study Purpose
We originally sought to review research on service provision as well as existing regulations and policies surrounding SGBV medical and legal services in East Africa (Rockowitz et al., 2021a); however, subsequent literature searches returned few academic papers on SGBV regulations and policies in East Africa countries. Per recommendations of Levac et al.(2010), to envision the intended outcome of the study while also considering the feasibility of the research, we modified our original research questions and focused solely on service provision in the region rather than service provision and policy. As a result, the following questions guided our scoping review:
Search Strategy
Our search strategy included conducting title, abstract, and keyword searchers of the PubMed, SCOPUS, CINAHL Plus, and Web of Science databases. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram was used to record the number of articles included along each step of the search process (Page et al., 2021).
Our review included literature on East African countries published between 2000 and 2020. This timeframe was chosen so that more recent policy and international health treaty agreements could be analyzed. Due to a lack of resources and translation skills, only papers in English were included in this review. Our search terms were chains created to allow for variations in terminology and phrases related to SGBV. These included “rape” + “East Africa,” “rape” + “East Africa” + “law,” “rape” + “East Africa” + “policy,” and “rape” + “East Africa” + “health.” We also used the terms “sexual assault” and “sexual violence” in place of “rape,” and we expanded “East Africa” when possible in the database to include “Burundi,” “Comoros,” “Djibouti,” “Eritrea,” “Ethiopia,” “Kenya,” “Madagascar,” “Malawi,” “Mauritius,” “Mayotte,” “Mozambique,” “Reunion,” “Rwanda,” “Seychelles,” “Somalia,” “South Sudan,” “Tanzania,” “Uganda,” “Zambia,” and “Zimbabwe.” We largely followed the UN’ geoscheme, which lists all the above countries, except South Sudan, as being in the East African region (Mendelson et al., 2014). As South Sudan is included in the East African Community, we included in our analysis (EAC Partner States, 2021). We conducted a grey literature search to find reports from nongovernmental organizations (NGOs) and other local organizations that worked with SGBV survivors.
Study Selection
Initial database searches yielded 14,230 academic articles, with an additional 124 results coming from other sources, such as grey literature and “cited by” searches. After these lists were combined and we removed duplicates using Endnote X9. This left us with 3,685 results to be screened by title and abstract. There are a few reasons why there were so many articles. Firstly, we were searching for research related to 20 countries, which yielded many results, and the use of the term “rape” yielded many irrelevant papers about “rapeseed” or “oilseed rape.”
A key element of a scoping review is that the researchers should engage with each step in the process in an iterative and reflexive way to comprehensively search the literature (Arksey & O’Malley, 2005). Levac et al. (2010) further noted that the research team should use an iterative approach to choosing studies and extracting data. To this end, the first author did the initial title and abstract screening, yielding 257 results. Articles and research documents were excluded if they were about countries other than those in East Africa, if they were about East African diaspora populations living elsewhere, if they were about preventing SV rather than working with survivors post-incident, if they were about agriculture as mentioned above, and others. After the initial review was conducted by the first author, titles and abstracts were uploaded onto the online systematic review program Rayyan (https://www.rayyan.ai), which facilitates collaboration when identifying articles for a review paper. The first author tagged articles with a green label for inclusion and a red label for exclusion, while also adding additional customizable tags such as “medical,” and “legal.” Afterwards, the link was shared with the co-authors, and they repeated the process. Any articles that were tagged differently by the co-authors were then discussed by the team to determine the final set of papers.
Additionally, many papers that appeared in the searches were specifically about abortion services or HIV medication provision; while SGBV was mentioned in these papers as a possible reason why these services may be needed, the authors determined that they should be excluded because they were not principally about SGBV. Following this process, as well as a full-text review by the first author, 54 papers were included in the final sample (see Figure 1 for the PRISMA diagram).
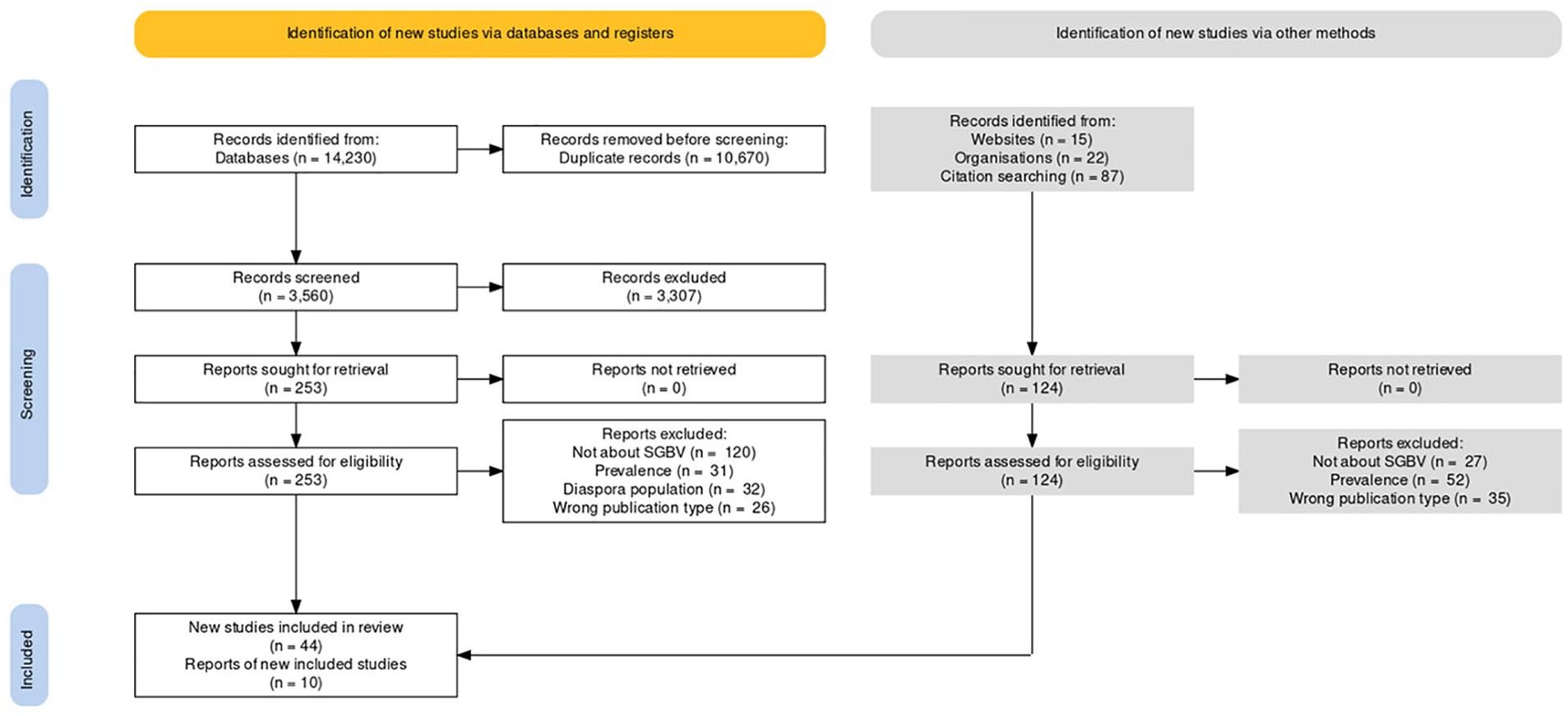
Preferred Reporting and Identification for Systematic reviews and Meta-Analyses flow diagram.
Data Charting
The researchers developed a data charting form using Microsoft Excel 2021. To facilitate data analysis and follow charting recommendations (Arksey & O’Malley, 2005), the charting form gathered information regarding the author, publication year and type (academic or grey literature), country, study design, study setting (refugee camp, health center, district, etc.), key findings, and the paper’s conclusion.
Results
Sample Characteristics, Study Design, and Study Setting
All academic articles (n = 44) and grey literature (n = 10) in the final sample were published between 2001 and 2020. Details of the breakdown of countries included can be found in Supplemental Table 1. Although 20 countries were included in the search, most countries did not appear in the findings, while others had a relatively high number of publications (Supplemental Table 1). Kenya was the country with the most publications, with 22 (35.5%) academic papers or reports focused on the Kenyan context alone and one paper focused on Kenya and Ethiopia together. The country with the next highest number of dedicated studies was Uganda, with 10 papers (16.1%), followed by Tanzania, and Zimbabwe with four each (6.5%). Two pieces of literature, one a journal article and one report from USAID, focused on the continent rather than specific countries.
In most cases, the studies were based on qualitative research methods, primarily through in-depth interviews or focus group discussions. As many papers also included document and record analysis from health centers, cross-sectional prospective methods were also commonly used. More information about study setting and methodology can be found in Supplemental Table 1.
Medical and Legal Service Provision Across East Africa
The results are organized by type of SGBV. The terminology used to describe types of SGBV had differing operational definitions across papers. For instance, sometimes the term “sexual assault” was defined to include acts of penile-vaginal penetration (rape), while in other papers, it was not defined specifically but instead used interchangeably with the terms “rape” and “sexual violence” (e.g., Lakew, 2001). Given the lack of clarity and inconsistencies across the literature, we were unable to operationally define and code violence type and had to rely on the terminology used in the papers.
Rape
Rape was the form of SGBV studied the most (see Supplemental Table 1). Unlike IPV, which can have differing definitions depending on the source, rape is more consistently defined, perhaps because all the countries included in this review legally define rape. For instance, the National Guidelines on Management of Sexual Violence in Kenya define rape as “An act done which causes penetration of one person’s genital organs with the genital organs of another without their consent or where the consent is obtained by force, threats or intimidation of any kind” (Ministry of Public Health & Sanitation and Ministry of Medical Services, 2009). Tanzania’s government defines rape as when “a male person. . .has sexual intercourse with a girl or woman under circumstances falling under any of the following descriptions:” including forcibly having sex with a non-wife or ex-wife due to use of force, obtaining consent when the woman is of unsound mind, and others (Tanzania, 1998). Throughout other countries in East Africa, rape is similarly defined. Penetration of often a requirement, and some countries still state that women can be raped by men, but men cannot be raped by women.
Most of the studies focused on rape were conducted in Kenya. Most papers used qualitative methods, primarily interviews, although some of the papers either solely or additionally performed document analysis, including retrospective record reviews from an adult rape clinic (Kufa et al., 2019). Of the 11 rape papers, all except one discussed service provision, and only two discussed interventions. The first intervention paper designed and implemented a training program for healthcare workers in Tanzania to improve the quality of care they offered rape survivors, and the second designed a post-rape care algorithm in Kenya to be implemented at selected government health facilities (Abeid et al., 2015; Kilonzo et al., 2009).
Papers focusing on rape collected information on medical and legal service provision from multiple sources. Some researchers interviewed providers, such as health practitioners or police officers (Ajema et al., 2009; Munala et al., 2018). Others interviewed survivors and those who care for them, or simply just community members who are aware of rape in their immediate surroundings (Kilonzo et al., 2003, 2009). Across all studies, there was minimal (if any) discussion of existing policies concerning service provision, except at times to say that there were none. As a result, a common theme across all papers was that their findings should be used for policy recommendations. These included formal training of healthcare workers, expanded abortion services, and the creation of a formal strategy for the provision of post-rape services (Abeid et al., 2015; Ajema et al., 2009; Casey et al., 2015; Kilonzo et al., 2003).
Despite these findings, it is important to note that research on rape was found for only five of the 20 countries that are in East Africa, and these were largely on Kenya. Additionally, little attention was paid to sociocultural factors that may have affected service provision or a victim’s decision to seek out services in the first place. For example, victim care may be affected by the religious alignment between victim and provider, or the victim preferring traditional health and justice practices (Odero et al., 2014).
Intimate Partner Violence
IPV was the second most frequently occurring type of violence found in the included papers. It was variously defined, such as “a form of interpersonal violence by a spouse or life partner” (e.g., Shumba et al., 2017) “violence committed against a woman by her current or former spouse or boyfriend” (e.g., Horn, 2010), “violence committed in a present or past relationship.” (e.g., Manuel et al., 2019). The primary data collection method for understanding medical and legal service provision for IPV survivors was qualitative interviewing, although two studies distributed surveys to medical students, nurses, and midwives (Ambikile et al., 2021; Manuel et al., 2019).
Two of the papers focused on mental healthcare needs of IPV victims, and these were specifically on screening processes and service provision (Ambikile et al., 2021; Chepuka et al., 2014). The remaining papers focused on screening for, responding to, or training for working with IPV cases more generally (Horn, 2010; Maina, 2009; Maina & Majeke, 2008; Manuel et al., 2019; Nguyen et al., 2016; Odero et al., 2014; Shumba et al., 2017; Undie et al., 2016). Unlike rape, there were no interventions studied in the IPV papers. Of the nine IPV papers, six focused on the providers’ perspectives, with all providers in these papers described as working in the medical field, not in the legal or justice fields. The other three papers sampled survivor and non-survivor refugees, survivors, or men and women in general.
Several studies cited a lack of knowledge and relevant skills as potential reasons for inadequate service provision. This was often attributed to a lack of targeted trainings, staff shortages, and lacking protocols for case management (Ambikile et al., 2021; Odero et al., 2014; Undie et al., 2016). Additionally, several papers noted the additional challenges associated with treating the mental health impacts of IPV, whether due to societal pressures to resolve issues, poor training of service providers, or a lack of linkages to mental health services (Ambikile et al., 2021; Chepuka et al., 2014; Odero et al., 2014).
Sexual Assault
Sexual assault (SA) was the third most common type of SGBV studied. Unlike other topics, which mention the type of SGBV in the titles of the papers without any qualification, two papers in this group, one in Uganda and one in Ethiopia, refer to “alleged” SA in the titles of their papers (Lakew, 2001; Ononge et al., 2005). Interestingly, all papers that studied populations in Ethiopia focused on SA.
As with other topics, SA is defined rather fluidly. One paper defined SA as “any genital, oral, or anal penetration by a part of the accused’s body or by an object using force or without the victim’s consent,” (Ononge et al., 2005). Another defined SA as “rape, attempted rape, sexual abuse and sexual exploitation,” and yet another as “all non-consenting sexual activity from fondling to penetration” (Amenu & Hiko, 2014; Krolikowski & Koyfman, 2012).
Six of the nine SA papers analyzed medical and legal service provision for SA victims. More than half of the SA papers used quantitative approaches, reviewing records or other data as the primary data source. This enabled the researchers to analyze more data: for instance, a study on a SA center in Western Kenya analyzed 321 charts of SA survivors and another analyzed 474 medical affidavits from a hospital in Zimbabwe (Ranney et al., 2011; Tapesana et al., 2017).
None of the SA papers about medical and legal service provision mentioned policy, either by the government or hospitals, that may pertain to the treatment of SA victims. Whether this means they were nonexistent is unclear, although it seems consistent with findings for other types of SGBV. Additionally, research concerning medical and legal service provision for SA victims was found for only four countries in East Africa, indicating a dearth of research both on SA in general and on service provision for said victims. This may be indicative of the “umbrella” of SGBV that many types of violence fall under or perhaps a reflection of the direction SGBV research has taken in recent years.
Sexual Violence
Seven papers in this review focused on SV. Definitions of SV were unique in that there was less of a focus on defining the act itself and more of a focus on noting what the societal and public health implications of SV are. For example, it was referred to as “a serious societal problem that creates significant challenges to local communities” and “a serious global health problem with significant physical, psychological, and social consequences” (Ajema et al., 2011; Gatuguta et al., 2018). While all included SV papers focused on service provision in some regard, only three focused on barriers. Two others focused on the perspectives of the providers, which is unique compared to other types of violence, and one was a report from USAID on strengthening service provision. The three service provision papers were all descriptive studies that used primarily qualitative methodologies.
The three SV papers that strictly covered medical and legal service provision were based in Kenya (2) and Uganda (1). Both Kenya papers used qualitative interviews with service providers to collect data, although one also compared health records from a hospital with data from the Demographic and Health Survey (DHS) (Gatuguta et al., 2018). Both Kenya papers mentioned the importance of proper forensic evidence collection to help victims pursue justice, which makes them unique from many of the other papers included in this study that have less of a focus on the legal aspect of service provision. As with previous types of violence, there was little mention of existing policy concerning service provision.
The paper based in Uganda is somewhat unique in this review in that it pulls data from an existing longitudinal study that the researchers had worked on previously. The WAYS Study, which focused on war-affected youth in Northern Uganda, was started in 2002 and targeted toward youth who had been targeted by the Lord’s Resistance Army (Amone-P’Olak et al., 2018). While the study primarily focused on the prevalence of post-traumatic stress disorder in the research population, there was also an assessment of the availability of mental health services. This paper was also distinctive in that a significant portion is dedicated to understanding the meaning of mental illness among the target population, a focus on cultural competency that has seldom been seen in previously included papers.
Sexual and Gender-Based Violence
Six papers on SGBV were included in this review. Four of the papers studied SGBV in humanitarian settings, primarily with South Sudanese refugees, and all were based in Uganda (Liebling et al., 2020a, 2020b). This may be because SGBV is an all-encompassing term that can cover many other types of violence, and because it is more commonly associated with humanitarian efforts than other terms, such as SV or IPV (Liebling et al., 2020a). Due to this context, SGBV was often not explicitly defined but rather was explained as a “weapon of conflict” and “a growing problem in humanitarian settings” (Liebling et al., 2020a, 2020b; Odwe et al., 2018). Four of the papers focused on service provision, either health alone or health and justice, one on perceptions of violence as well as service provision, and the final paper focused on help-seeking.
Most of the service provision papers for SGBV explicitly mentioned both health and justice service provision, perhaps because of the focus on refugees and the involvement of international aid organizations in their care. As a result of the involvement of the justice aspect of service provision, bribery and corruption appeared multiple times throughout the included papers (Liebling et al., 2020a, 2020b; McCleary-Sills et al., 2013). An interesting component when evaluating these papers that is not included in many of the others is the involvement of international actors, such as the UNHCR (UNHCR) and Médecins Sans Frontieres (MSF). This means that the systems being evaluated are not necessarily on the country-level alone, but instead reflect collaborations between local governments and international actors and human rights officials. It is therefore difficult to ascertain how much responsibility individual countries take for service provision and how much they outsource to international aid organizations.
Gender-Based Violence
Five papers covered GBV, four of which researched GBV in humanitarian settings. As a result, GBV was often defined in relation to conflict. For example, one paper noted that “GBV has been committed against civilians and soldiers as a means of warfare,” while another noted that “emergency and humanitarian situations expose individuals, particularly women and girls, to a heightened risk for GBV” (Kawaguchi, 2018; Muuo et al., 2020).
All but one of the included papers were academic articles, with the final being a report from a Japanese aid organization (Kawaguchi, 2018). All papers focused on service provision, although one was on reproductive health services more generally rather than specifically GBV (Whelan & Blogg, 2007). All papers but one focused on existing structures for service provision, and the final analyzed a dataset from a purpose created GBV and recovery center in Mombasa (Temmerman et al., 2019). The primary data sources across all studies were female refugee GBV victims, although a few studies also interviewed providers.
A few common themes appeared throughout the included papers. Financial constraints, either at the health facility level or the aid organization level, were seen as a common barrier to adequate service provision (Henttonen et al., 2008; Kawaguchi, 2018; Whelan & Blogg, 2007). Stigma was noted in most papers as a reason for underreporting of GBV and one of the barriers to accessing care (Henttonen et al., 2008; Kawaguchi, 2018; Muuo et al., 2020; Temmerman et al., 2019), though little was said about what could be done to address this problem.
Violence Against Women
Three papers examined violence against women (VAW). Two were academic articles, one was a report, and all covered medical and legal service provision (Amnesty International, 2010; Dennis et al., 2019; Vyas, 2019). Uganda, Tanzania, and Zambia were all represented once, making this one of the few topics where Kenya was not the primary area of work. Another unique aspect of this pool of research is that primarily quantitative methods were used. One paper analyzed data from Tanzania’s DHS, and other used signal functions to identify the availability of clinics that were able to provide VAW services (Dennis et al., 2019; Vyas, 2019). The final paper conducted qualitative interviews with victims, NGOs, government officials, and international aid organizations to ascertain their experiences in providing and accessing care (Amnesty International, 2010).
Both quantitative studies found that distance was a limiting factor for accessing post-VAW services. Researchers in Zambia discovered that the median distance to a comprehensive care facility was 5.9 km and that quality of care was often poor, owing to limited resources or poorly trained staff (Dennis et al., 2019). Researchers in Tanzania similarly found that abused women had to travel on average 3.8 km to their nearest health facility, although the quality and comprehension of care offered was not assessed (Vyas, 2019).
Interpersonal Violence, Domestic Violence, and Collective Sexual Violence
These three forms of violence occurred only once each in the literature search. All three papers included were academic articles and used qualitative methods. One such paper covered interpersonal violence (IPEV), which is used as an umbrella term to include community violence, IPV, SV, and more (Decker et al., 2018). This paper (Schober et al., 2016) was based in Zambia, while the studies on domestic violence (DV) (Githui et al., 2018) and collective SV, which refers to nonconsensual sexual activity by a group of individuals or single individual that is driven by social movement goals (Ten Bensel & Sample, 2017; Zraly et al., 2011) were based in Kenya and Rwanda, respectively. Because only one paper was found for each violence type, the quality of research throughout the region more generally could not be assessed. Githui et al. focused on barriers to screening pregnant women for DV, Zraly et al. focused on providing mental healthcare for genocide survivors, and Schober et al. applied an intervention to an emergency room to improve care outcomes for IPEV victims. Participants of the three studies include medical and social service professionals, members of refugee support groups, and nurses, indicating once again that there is very little focus on the legal aspect of service provision throughout the region.
Service Provision Models and International Health Treaties
Types of service provision were varied, and included emergency center care, access to emergency contraception (EC) post-SA, and mental health care services (Amone-P’Olak et al., 2018; Kassa et al., 2009; Krolikowski & Koyfman, 2012; Maina, 2009). While most articles focused on provision of medical services, including mental healthcare, a few also focused on access to legal and judicial services (Liebling et al., 2020a, 2020b; Muganyizi et al., 2011; Odero et al., 2014).
The most consistent form of service provision offered was EC, typically in the form of oral contraceptive pills and often in tandem with post-exposure prophylaxis for HIV (Amenu & Hiko, 2014; Amnesty International, 2010; Dennis et al., 2019; Gatuguta et al., 2018; Kilonzo et al., 2003; Kilonzo & Taegtmeyer, 2005; Krolikowski & Koyfman, 2012; Muganyizi et al., 2011; Ononge et al., 2005; Tapesana et al., 2017; Temmerman et al., 2019). Although EC was included in the most basic of service packages, and was offered the most frequently, as with most other services in this region, resource constraints limited availability. Furthermore, a survivor was not eligible for EC if they presented outside of the 72-hour window in which it would still be effective (Ononge et al., 2005). Additionally, a lack of knowledge on behalf of some survivors led them to refuse EC even when they were offered it. Research in Zimbabwe found that 20% of clients who were eligible for EC did not take it, perhaps due to a lack of education and sensitization, and research in Ethiopia similarly found that a lack of knowledge about EC in society was a barrier to providing adequate health services to victims of SA (Harrison et al., 2017; Kassa et al., 2009).
Another factor that was a significant predictor of the type of service provision a survivor would receive was the tier of health facility to which they had access. Tiers and levels of health facilities vary significantly within countries, with some countries (such as Kenya) having as many as six tiers of health facilities (Gatuguta et al., 2018). Laboratory services were no exception; district health facilities in Kenya were found to be unable to analyze all components of forensic medical exam samples, while other health facilities lacked speculums and rape kits (Ajema et al., 2011; Gatuguta et al., 2018). This point was emphasized by Dennis and colleagues, who found that signal function domains, defined as three domains of SV response services (core services, immediate care, and delayed and follow-up care) varied greatly by level of health facility (2019). When surveying hospitals, the most advanced facility level, only 50% were able to offer all three signal functions, and less than 1% of health centers and 0% of health posts were able to offer all three signal functions (Dennis et al., 2019). Tanzania had similar breakdowns in service availability by facility level, with health dispensaries being able to provide the most basic of services and district designated hospitals or referral hospitals able to provide more comprehensive GBV services (McCleary-Sills et al., 2013). Similar disparities between services offered at health facility level were found in Uganda and South Sudan (Casey et al., 2015; Liebling et al., 2020a, 2020b).
This study initially sought to compare existing service provision models with international treaties that the countries had signed and/or ratified, but there was no mention of this in any of the papers included in the study. Additionally, since there is little policy literature, it is difficult to tell if the countries have changed their laws in response to the treaties they signed. Regardless, it is possible to compare what we learned about existing practices with public health treaties, such as the Maputo Protocol and the SDGs. For instance, the Maputo Protocol instructs state parties to establish mechanisms for the rehabilitation of victims of SGBV, yet previous findings have shown that services are often scarce, inaccessible due to financial or infrastructural constraints, and lacking the involvement of legal professionals (African Union, 2003; Ajema et al., 2011; Gatuguta et al., 2018). The Maputo Protocol also states that there should be a focus on eliminating cultural beliefs and stereotypes that “exacerbate the persistent and tolerance of violence against women,” yet our research shows that these beliefs are still pervasive and having strong impacts on victims’ care (African Union, 2003; Ferdowsian et al., 2018; Munala et al., 2018). SDG 5, which also focuses on eliminating violence against women and girls, states there should be universal access to sexual and reproductive health services (UN, 2021). As with the Maputo Protocol, our research indicates that this is simply not the case for people living in countries in East Africa.
Providers’ Personal Beliefs
Nine papers in this review studied the personal beliefs of service providers. All the papers were academic articles and, as seems to be the overall trend with research in East Africa, most of the research took place in Kenya. Of the 20 countries included in East Africa, only Kenya, Malawi, Ethiopia, Tanzania, and Mozambique were represented in this area of research. Qualitative methodology was used in all studies, primarily qualitative interviews, or self-administered surveys. Some studies evaluated the providers’ perceptions of the victims themselves, while others examined how the providers viewed or understood their responsibilities in providing care for SGBV victims. IPV was the most common type of violence included in these studies, followed by SV, rape, and SA. This is an interesting finding, as rape was the most common type of violence studied overall yet occurred only once in this topic area.
Two of the studies on the topic of duty bearers included NGO-organized trainings aimed at service providers to improve their “capacity to provide services to SV survivors” and to “improve the clinical care of SA survivors in diverse low resource settings” (Ferdowsian et al., 2018; Smith et al., 2013). One study evaluated beliefs pre- and post-intervention, and the other evaluated the effect of multiple variables on participant responses during the early stages of the intervention. All other studies in this group were descriptive. Attitudes, beliefs, knowledge, and confidence were some of the factors being evaluated in both studies, and pre- and post-intervention responses were measured with self-administered questionnaires.
Of the nine papers, the majority focused on the healthcare providers’ views on how they cared for the victims, although three focused more on how the providers viewed the victims and how their opinions of the victims affected their care provision. All nine papers interviewed providers of varying types, be it medical students, nurses, midwives, or doctors, and one paper based in Kenya also interviewed legal and law enforcement professionals. The focus on healthcare professionals in this theme is reflective of the pattern seen throughout the review, wherein very little attention was paid to service providers other than those in the medical field.
Victim blaming was a pervasive theme throughout this group of articles, whether perpetrated by the service providers themselves or simply observed by them. Perhaps the most glaring example of provider bias came from a study in Nairobi, which found that providers felt they could tell when a survivor was not being genuine but was instead trying to access free reproductive health services, particularly because of being a commercial sex worker and being too ashamed to say so (Munala et al., 2018). One provider interviewed in the study noted “Not every client is genuine. Someone will find something happens and because now they are scared of the pregnancy they will tend to create a story” while another said, “Ok people are not being truthful; others know that you provide services for free” (Munala et al., 2018). Other research in Kenya evaluating attitudes toward SV survivors across different professional sectors found that law enforcement professionals were the most likely to feel that survivors should feel ashamed (19%), followed by legal professionals (13%) and healthcare professionals (5%) (Ferdowsian et al., 2018). In a humanitarian context, lying about SA was seen as a way of qualifying for resettlement. One nurse in Ethiopia believed that women “don’t come with medical problems they come for referral. They like to be referred. It is spoken or rumored that they will get a chance of getting resettlement” (Smith et al., 2013). Despite the training initiated during the intervention, there were not significant improvements post-intervention in the 68% of HCPs in Ethiopia who agreed that “people often make accusations about SA that are not true” or the 35% of healthcare providers who agreed with the opinion “if a woman’s husband forces her to have sex, it does not count as sexual assault” because of cultural beliefs about a man’s rights concerning his wife (Zraly et al., 2011).
Providers also felt that societal views of SGBV impacted their ability to provide services, both in how feelings of shame often prevented survivors from coming forward, which they understood from discussions with community members, and in how survivor-family interactions played out while in health centers. Providers additionally found that the potential financial consequences of reporting rape often dissuaded survivors from coming forward, especially when the perpetrator was the primary wage earner (Munala et al., 2020; Nguyen et al., 2016). Healthcare workers felt that their capabilities were limited by the societal views of violence, observing that often they would try to help but the community’s ideals surrounding keeping families together and simply paying off the perpetrator made it difficult for them to do their jobs. One counseling psychologist described how she could do little more than try to make sure her clients were medically safe, as her abilities to help her clients who settled out of court were limited and the survivors had to continue living in the presence of their attacker(s) in their daily life after reparations had been arranged between families, potentially causing re-traumatization (Munala et al., 2020).
Gaps in the Literature
While Arksey and O’Malley’s framework was key in executing most steps of this scoping review, the PAGER (pattern, advances, gaps, evidence for practice, and research recommendations) framework was referenced when identifying and addressing the gaps in the literature. This framework supplements Arksey and O’Malley’s previous work and emphasizes that the identified gaps be contextualized and written for the target audience. With this in mind, a few notable gaps in the literature were found (Bradbury-Jones et al., 2021). A group notably absent from this review were men and boys, although this is largely to be expected because of the stigma attached to male victims of SV and the fact that significantly fewer men are victimized than women. Additionally, survivors who identified as genders beyond strictly male and female were not mentioned in the papers included in this review. It was not always clear whether the researchers excluded these other victims intentionally or whether they simply did not come forward to participate. Future research should examine service provision plans to determine whether and how providers adapt treatment depending on the gender of the survivor. Additionally, studies did not examine the type of psychosocial services offered to survivors. Research on this topic would further our understanding of how survivors’ wellbeing is managed once they leave a health facility. Many papers mentioned women were often afraid to leave their spouses because of financial insecurity or societal pressures, and research regarding possible solutions for this, such as economic assistance or relocation, was largely absent from this literature.
Although this scoping review initially sought to examine medical and legal service provision, it became immediately clear that there is significantly less research on the legal/justice side of SGBV care than on the medical side. Of the 54 papers included in this review, 11 interviewed legal professionals, including police and justice organizations. These 11 papers covered only five of the 20 countries in East Africa, indicating there is a significant gap in knowledge about most countries in the region. It is important to conduct research on the legal aspect of post-SGBV service provision, especially because, while medical services may offer physical wellness to the survivors, pursuing justice and prosecuting the perpetrators may provide a sense of closure and security, as well as prevent the perpetrators from committing future similar crimes.
This review initially sought to evaluate existing medical and legal service provision practices throughout East Africa as they relate to country and region-wide policies; however, policy was scarcely mentioned throughout the literature. Without this insight, it made it difficult to know if the medical and legal practices were occurring as such because of a lack of guidance, because that is how the country’s government or hospital’s board instructed, or because of resource constraints. Additionally, the lack of policy inclusion made it difficult to compare country-wide medical and legal service guidelines with internationally agreed treaties, which was another original plan of this review which ended up not being feasible.
Discussion
This scoping literature review of 54 papers about SGBV in East Africa identified key themes surrounding both types of violence commonly seen in the region and common approaches to service provision. Many types of violence were identified as being pervasive throughout the region, and while rape was the most common type of violence in the selected literature, the interchangeable nature with which researchers and aid organizations use different definitions of violence mean that this finding is not necessarily reflective of which type of violence is the most prevalent in East Africa. Papers discussing rape made up 20% of the sample, followed by IPV (18%) and SA (17%).
Ten types of violence emerged from the literature. Although a type of violence was often specified in the title, authors frequently switched between terms when explaining their research, further exacerbating the issue with finding clear, violence-specific data and contributing to poor data quality. This makes it difficult to compare similar statistics across countries and can complicate case building as the laws in countries may only pertain to some types of violence and not others. It is, however, an interesting finding that similar behaviors are being defined differently, perhaps pointing to political reasons why one phrase is preferred over another. Rape, for instance, is clearly defined in many countries’ constitutions, whereas other terms, such as IPEV, are not mentioned once. In acknowledging the potential reasons why certain terms may be used more than others, we felt it was appropriate to organize this paper by the frequency of the term used in the papers included in this review. Rape, SV, and SGBV were often woven throughout a paper when describing the same study, although technically speaking, each of those terms has a different definition according to lawmakers, NGOs, and human rights organizations (Harrison et al., 2017; Liebling et al., 2020a, 2020b; Munala et al., 2018). SGBV and SV could perhaps be thought of as umbrella terms, however this should be better clarified in the papers for ease of understanding if certain types of violence make a victim more likely to seek and receive care and how resources are allocated.
Societal views of women were seen as a common cause of the violence itself and of the reluctance among survivors to seek help (Gatuguta et al., 2018; Kilonzo et al., 2003; Munala et al., 2020; Shumba et al., 2017). Patriarchal communities were explained as a common cause of violence throughout the region, although perhaps because the papers were not about preventing violence but rather addressing the side effects of it little was said about what could be done to address the patriarchal ideologies that made SGBV acceptable (Amnesty International, 2010; Kilonzo et al., 2003; Liebling et al., 2020a, 2020b; Manuel et al., 2019; McCleary-Sills et al., 2013; Munala et al., 2020; Odero et al., 2014; Tapesana et al., 2017). Patriarchal systems were also seen as the reason why many women did not seek help, but instead stayed in abusive relationships owing to ideas about what sort of behavior is to be expected in a marriage, as well as fears about financial insecurity and potential homelessness if one were to report her husband to the authorities (Fiske & Shackel, 2015; Kilonzo et al., 2003; McCleary-Sills et al., 2013).
A lack of human, material, and financial resources contributed to the difficulties in service provision felt by survivors and providers alike. Limited funding for supplies meant that, although providers often knew what should be included in a rape kit and what sort of treatment survivors should have access to, they simply did not have the resources to give to each survivor (Ajema et al., 2009; Dennis et al., 2019; Henttonen et al., 2008). A common approach to evaluate the quality of post-SGBV service provision was whether certain supplies were available in a post-rape/SGBV kit, or the elements of SGBV survivor medical management plans. The most common supplies deemed necessary to provide adequate care were EC, HIV tests and prophylaxis, speculums, and other materials needed for forensic exams (Dennis et al., 2019; Krolikowski & Koyfman, 2012; McCleary-Sills et al., 2013; Temmerman et al., 2019). While the possession of these materials is promising, their presence in a health facility does not mean that they are being utilized correctly, if at all. Resource constraints may mean that while some materials do exist, not all victims who present are deemed worthy of their use. Researchers also examined whether survivors were referred to psychological, psychosocial, and legal services to evaluate whether a given service provision package was comprehensive (Buard et al., 2013; Chepuka et al., 2014; Dennis et al., 2019; Gatuguta et al., 2018; Harrison et al., 2017; Kilonzo et al., 2009; Liebling et al., 2020a, 2020b; Liebling et al., 2019; Ononge et al., 2005; Ranney et al., 2011; Sithole et al., 2018; Tapesana et al., 2017).
Determining approaches to SGBV service provision throughout the region of East Africa was difficult, as some countries were studied far more than others. Kenya, for example, featured in 23 papers, whereas smaller countries, such as Burundi, Comoros, Djibouti, and Madagascar, were not mentioned once. Additionally, some countries in East Africa were mentioned mainly in the context of refugees that had come from that country to other countries in search of humanitarian aid, like refugees from Somalia and South Sudan in refugee camps in Kenya and Uganda (Amnesty International, 2010; Horn, 2010; Kawaguchi, 2018; Liebling et al., 2020a, 2020b; Muuo et al., 2020; Whelan & Blogg, 2007). Our review found that resource constraints and the failure of countries to follow WHO guidance were the most common themes that cut across the research studies on post-SGBV service provision in East Africa, although other issues, such as inconsistent provider training and provider bias, were also significant barriers to adequate service provision (Ajema et al., 2011; Ambikile et al., 2021; Amnesty International, 2010; Dennis et al., 2019; Gatuguta et al., 2018; Henttonen et al., 2008; Muganyizi et al., 2011; Nguyen et al., 2016; Odwe et al., 2018; Tapesana et al., 2017; Whelan & Blogg, 2007; Zraly et al., 2011).
Limitations
One limitation of the literature is the dearth of information about policies in each country. Although policy evaluation was to be included in this review according to the original protocol, it was so scarce in the literature that it had to be removed from the review altogether. Because there is such limited information on this topic, it is difficult to tell how each country’s service provision compares to what “should” be happening, and what the possible policy implications might be. By not mentioning national policies as a criterion to evaluate service delivery, and similarly by neglecting to mention human rights treaties as a means of measuring the ethics of service provision, there is little official guidance to compare the practices to, WHO guidelines for post-SGBV service provision were mentioned many times; however, these are not legally binding, whereas national policies would be. Additionally, there was little information provided about the health systems in each country, such as how the levels of care were divided or whether the country had nationalized health services, as well as the socioeconomic status of participants. Information on both facts could have helped provide a more comprehensive picture of why services are being accessed in the manner they are, especially regarding a victim’s socioeconomic status compared to their country’s health system. The researchers expanding on the types of services offered at private versus public institutions could have clarified equality of care, although most survivors surveyed accessed public institutions.
Conclusion
SGBV is a widespread human rights violation that is especially prevalent in the East African region. Research has found that current models and methods of service provision are leaving survivors with significant medical and psychosocial needs, and that countries are not providing adequate funding for services. Given the tremendous impact SGBV has on society, there is a need for further research into how to better incorporate SGBV into existing health systems and how to align the national policies of countries with international human rights treaties and WHO recommendations. Researchers should also account for the limited research that exists in some of the smaller countries to ensure that no SGBV survivors get left behind.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221134292 – Supplemental material for A Scoping Review on Sexual and Gender-Based Violence Medicolegal Service Provision in East Africa
Supplemental material, sj-docx-1-tva-10.1177_15248380221134292 for A Scoping Review on Sexual and Gender-Based Violence Medicolegal Service Provision in East Africa by Sarah Rockowitz, Heather Flowe and Caroline Bradbury-Jones in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.