
Abstract
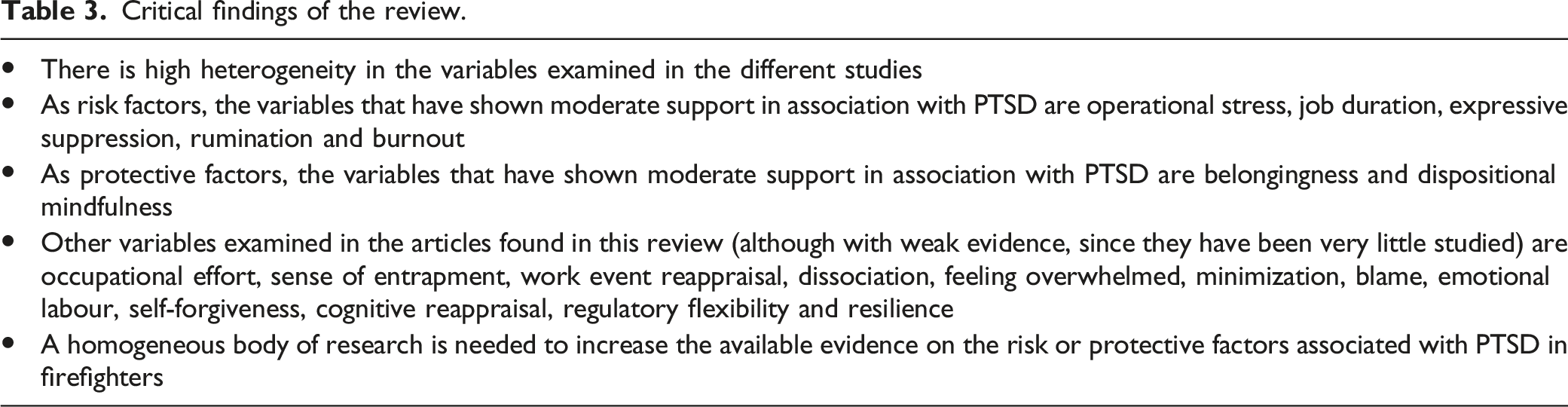
Firefighters are repeatedly exposed to work-related potential traumatic events and have an increased risk of developing post-traumatic stress disorder (PTSD). However, the mechanisms implicated in this relationship are not clear. The aim of this study was to analyse the risk and protective factors related to the development of PTSD in firefighters. According to PRISMA, a systematic review of scientific literature was conducted in Web of Science, PsycINFO, Scopus, PubMed and the Cochrane Central Register of Controlled Trials. Quality in Prognosis Studies (QUIPS) was used as the methodological quality indicator of the selected articles (PROSPERO reference CRD42020213009). Prognostic studies involving active firefighters with presence of post-traumatic symptomatology, presenting original findings, and written in Spanish or English were included. A total of 1768 potentially eligible articles were identified. According to the inclusion criteria, 87 articles were selected to evaluate the full text. Finally, 19 articles were included, comprising 12,298 active firefighters. There is high heterogeneity in the variables evaluated in the different studies. Taking the data for which this review has found more evidence (moderate support), operational stress, job duration, burnout, expressive suppression and rumination could be risk factors of PTSD, and belongingness and dispositional mindfulness could be protective factors. Other variables with weak support (e.g. resilience) were analysed. This review analyses the available literature, highlighting its scarcity for future research on the subject. Due to repeated trauma exposure, it is important to continue investigations and bear these variables in mind for the prevention of PTSD in firefighters.
Worldwide epidemiology studies have found that 70% of people have experienced one or more traumatic event in their lifetime (Benjet et al., 2016) and 4% of the population have suffered post-traumatic stress disorder (PTSD) after a trauma (Kessler et al., 2017). However, this prevalence changes depending on various factors such as the type of job held. It has been found that first responders or emergency workers face a variety of potentially traumatic situations more recurrently than the general population (Carleton et al., 2019).
In view of the nature of emergency services, first responders are regularly exposed to real/threatened death or serious injury as part of their work-related activities. They can directly experience it, witness it in victims or colleagues, or learn that the event has occurred to a person close to them. All these factors comprise the DSM-5 conceptualization of trauma (American Psychiatry Association, 2013).
Compared with other emergency groups, firefighters are more exposed to traumatic events, including transportation accidents, fire or explosions, serious accidents at work, home or during recreational activity, life threatening natural disasters, violent death, severe human suffering, corpse rescue and toxic substances (Sahebi et al., 2020). Moreover, 80% of firefighters have frequent and repeated traumatic experiences; each of these situations is usually suffered 11 or more times throughout their career, significantly more than other first responders (Carleton et al., 2019). For example, 89% of firefighters exposed to a serious transportation accident reported 11 or more exposures, whereas only 73% of police officers have been exposed this number of times. In addition, 57% of firefighters are exposed 11 or more times to toxic substances compared to 18% of police officers or 20% of paramedics (Carleton et al., 2019). These frequent and repeated traumatic events are a crucial aspect of what could distinguish firefighters from other first responders, since the importance of accumulated trauma has been demonstrated in this and other populations (Karam et al., 2014).
Furthermore, their main occupation of firefighters is to attend an emergency. This is different from, for example, police officers, who also have other functions such as traffic organization, or ambulance personnel who attend other types of situations such as childbirth (Skorgstad et al., 2013). Moreover, firefighters are directly involved in the stressor and the resolution of the emergency (for example, rescuing people caught in a fire or removing them from a car in a traffic accident), because they are the ones who must work within the stressful situation to resolve it. In doing so, they could put their life in danger. Furthermore, they suffer from secondary trauma, which results from helping others who are suffering (Greinacher et al., 2019).
Due to all this, firefighters are at a high risk of developing PTSD (Wagner et al., 2020a, 2020b). Berger and colleagues (2012), in a meta-regression analysis, showed a worldwide PTSD prevalence of about 7.3% in firefighters, with significant differences compared to police officers (4.7%). Skorgstad and colleagues (2013), in a systematic review about work-related PTSD, found that 20% of firefighters, compared to 10% of police officers, were sufferers, noting a major problem in this population.
Symptoms of PTSD include difficulty concentrating, sleeping problems, flashbacks, intrusive thoughts or images, irritability, etc. (APA, 2013). All these aspects could be putting at risk not only the health or life of these professionals, but also the quality of their work and care for the victims (for example, reducing their capacity when risking their own life by entering a burning building to save victims). Additionally, PTSD is associated with poor quality of life (Noor et al., 2019) and has been shown to increase the risk of suicidal ideation and suicide (Noor et al., 2019) in firefighters, as well as destructive behaviour such as drug or alcohol misuse (Lebeaut et al., 2020; Smith et al., 2019). For all these reasons, it is important to analyse this phenomenon in firefighters, to know its development in this specific population and prevent it.
In line with this, the general literature shown that the association between suffering traumatic experiences and developing PTSD is indirect and is mediated or moderated by different factors. The importance of risk and protective factors is exposed in the Diathesis-Stress Model of Post-Traumatic Stress Disorder (McKeever & Huff, 2003), which postulates that the development of PTSD is mediated by three basic factors: (a) ecological diathesis, referring to psychological and social risk factors – for example, the level of social support; (b) biological diathesis, referring to neurobiological risk factors – for example, genetic aspects or neurochemical abnormalities; and (c) residual stress, being the negative psychological condition resulting from exposure to a traumatic situation. The diatheses could interact with one another and, in turn, with the severity of the traumatic experience and its residual stress, causing PTSD (McKeever & Huff, 2003). Thus, a person with a high premorbid risk (who would present many risk factors) would not need the severity of the traumatic experience to be very high to develop the disorder, and vice versa.
Thus, understanding the risk factors implicated in the development and maintenance of PTSD could be relevant to preventing or treating this problem in order to avoid developing long-term trauma-related psychopathology. Several reviews among general populations have found that the risk factors for developing PTSD and post-traumatic symptoms include family psychiatric history, prior trauma psychopathology, trauma severity, poor emotional regulation and low social support or dissociation (Brewin et al., 2000; Ozer et al., 2008). On the other hand, studies have found that variables such as resilience (Agaibi & Wilson, 2005), trauma-coping self-efficacy (DeCou et al., 2019) and social support (Dworkin et al., 2018) could be protective factors against PTSD. Other researchers have revealed that strong group cohesion, trust in leadership, high motivation and training are related to lower PTSD scores (e.g. Weisæth, 2002). Nevertheless, the samples of these studies are diverse (general populations, combat veterans, etc.), and these risk and protective factors could be different in firefighters owing to the characteristics of the traumatic situations they face. To the best of our knowledge, there are no published systematic reviews on the risk and protective factors in this population.
Several studies (for example, Kearns et al., 2012) indicate that prevention and early intervention on risk and protective factors in cases of PTSD in firefighters could prevent the development of the disorder and/or its aggravation. Thus, to help these professionals, it is clinically and theoretically important to identify the psychological variables implicated in the development and maintenance of PTSD in firefighters. The aim of this study was therefore to examine and condense the current body of scientific knowledge on risk and protective factors related to PTSD in firefighters.
Method
A systematic review of the literature was conducted. The international prospective register for systematic reviews (PROSPERO) accepted the protocol of this systematic review, registration number CRD42020213009, on 6 November 2020 (PROSPERO, 2020). This systematic review follows the guideline of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021).
Search Strategy
The search was conducted using the electronic databases Web of Science (WoS), PsycINFO, Scopus, PubMed and Cochrane Central Register of Controlled Trials (CENTRAL). The search was closed on December 2020. The only limitations imposed on the search were the inclusion of documents in English and Spanish that were peer-reviewed and human studies. There were no limits regarding the publication year. Boolean logic operators were used to combine search terms. Considering the format of each database, the combination and form of terms were firefighter AND post-traumatic stress, to ensure that all available articles were selected.
Inclusion and Exclusion Criteria
The established criteria for this systematic review followed the traditional method of PICOS (population, intervention, comparator, outcomes, study), adapted for a systematic review of association (Higgins & Green, 2008; Moola et al., 2015). The inclusion criteria were as follows: (i) population: active female and male firefighters; (ii) exposure of interest: different and wide range of risk and protective factors of post-traumatic stress disorder; (iii) outcome: presence of PTSD or post-traumatic symptomatology assessed by self-report or validated tools; regarding the DSM, only articles pertaining to DSM-IV-TR and DSM-5 were included; and (iv) type of study: prognostic studies (quantitative, observational studies, including retrospective, prospective, cross-sectional, longitudinal and cohort studies). Thus, retired, training or veteran war firefighters were excluded, as well as intervention or case-control studies, editorials and conference abstracts.
Quality and Risk of Bias Assessment
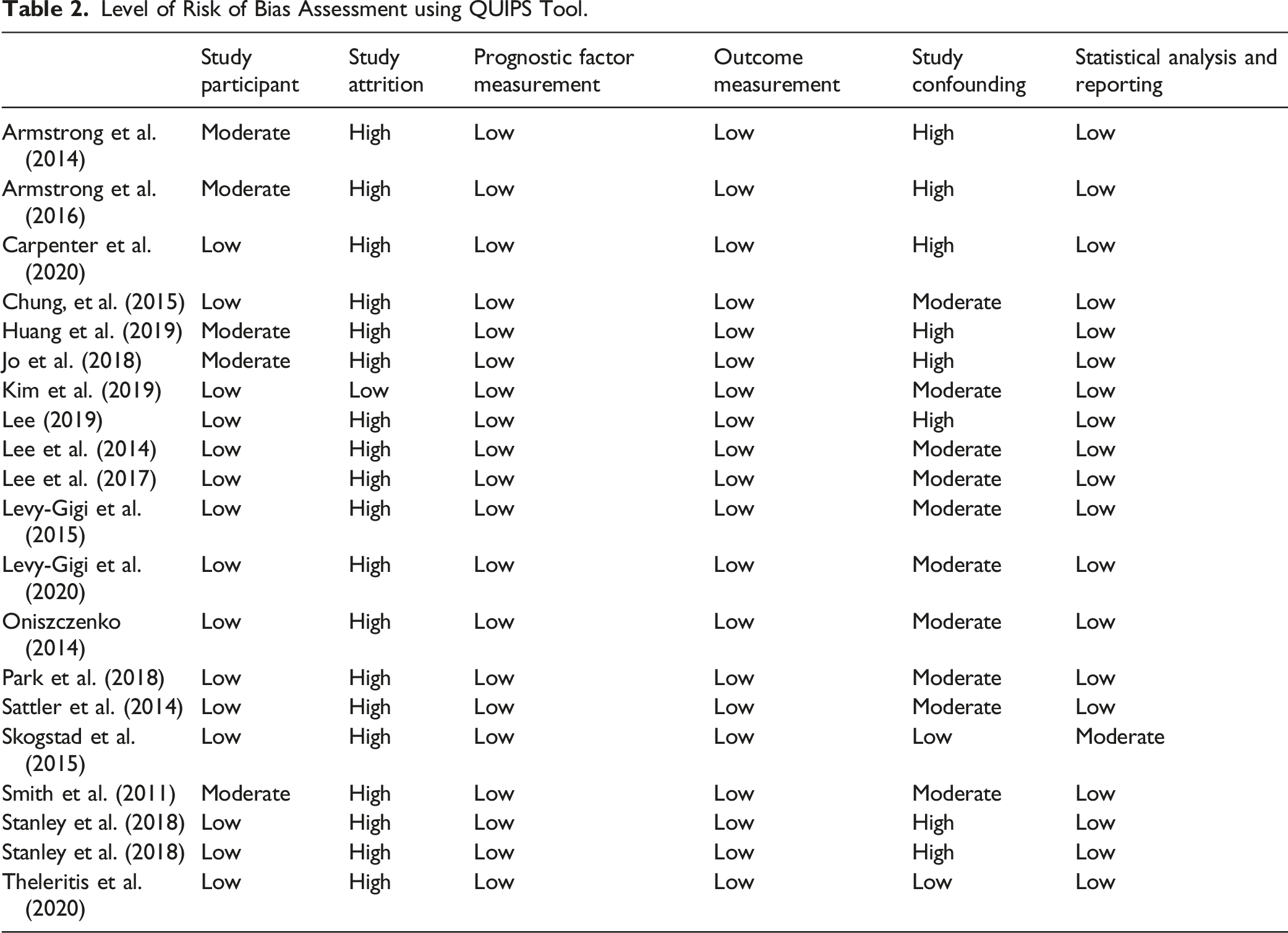
Two independent reviewers assessed the methodological quality of the selected articles using Quality in Prognosis Studies (QUIPS), the tool recommended by Cochrane. This tool contains six main domains of evaluation: (i) study participation: the study sample represents the population of interest; (ii) study attrition: loss from study sample is not associated with specific characteristics; (iii) prognostic factor measurement: this variable is adequately measured in the study sample; (iv) outcome measurement: this variable is adequately measured in the study sample; (v) study confounding: potentially confounding variables are adequately accounted for; and (vi) statistical analysis and reporting: analysis is adequate for the design of the study (Hayden et al., 2006). Each of the domains presents a series of descriptors to be evaluated on a three-point scale (high, medium or low level of risk), according to the tool specification, to analyse the risk of potential bias in the results (Grooten et al., 2019).
Data Synthesis
Three independent reviewers conducted the data extraction. The extracted information included the following: (i) characteristics of the study: authorship, year, country and sample size; (ii) characteristics of the population: gender, age, marital status, firefighters’ job roles and years of service; (iii) characteristics of the exposure variables: type, frequency and instrument to measure trauma, types and instruments to assess risk and protective factors for PTSD; (iv) characteristics of the outcome variable: instrument or DSM chosen to assess the presence of PTSD or symptoms or PTSD; and (v) characteristics of statistical analysis: type of statistical analysis and results.
Results
Identification of Studies
A total of 1768 articles were identified using the research strategy described and were imported into Rayyan, a web application to work with systematic reviews. Of these, 870 were removed because they were replicated across the five databases. Finally, 898 were analysed for the information provided in their title and abstract. Of these, 809 were excluded because they did not meet the inclusion criteria: the sample population was not the object of study of this review (for example, some studies’ sample comprised retired firefighters or veterans), the study did not examine risk or protective factors for PTSD, or the study’s design was not appropriate for the review (for example, intervention studies).
Finally, the authors read the full text of the 87 studies, 19 of which were included for analysis in this review. Sixty-eight articles were excluded because they did not meet the inclusion criteria: (i) population: the sample of 15 studies did not comprise active firefighters (nine retired, two veteran war and four training firefighters); (ii) exposure of interest: 25 articles did not analyse risk or protective factors for PTSD; (iii) outcome: 19 studies were excluded because they did not report PTSD, or not according to DSM-IV-TR or DSM-5 criteria; and (iv) type of study: nine articles were not prognostic studies (eight intervention studies and one editorial).
Two independent reviewers completed the process and disparities were resolved by a third reviewer. Figure 1 shows the flow chart of the study selection process according to PRISMA. Flow diagram of study selection.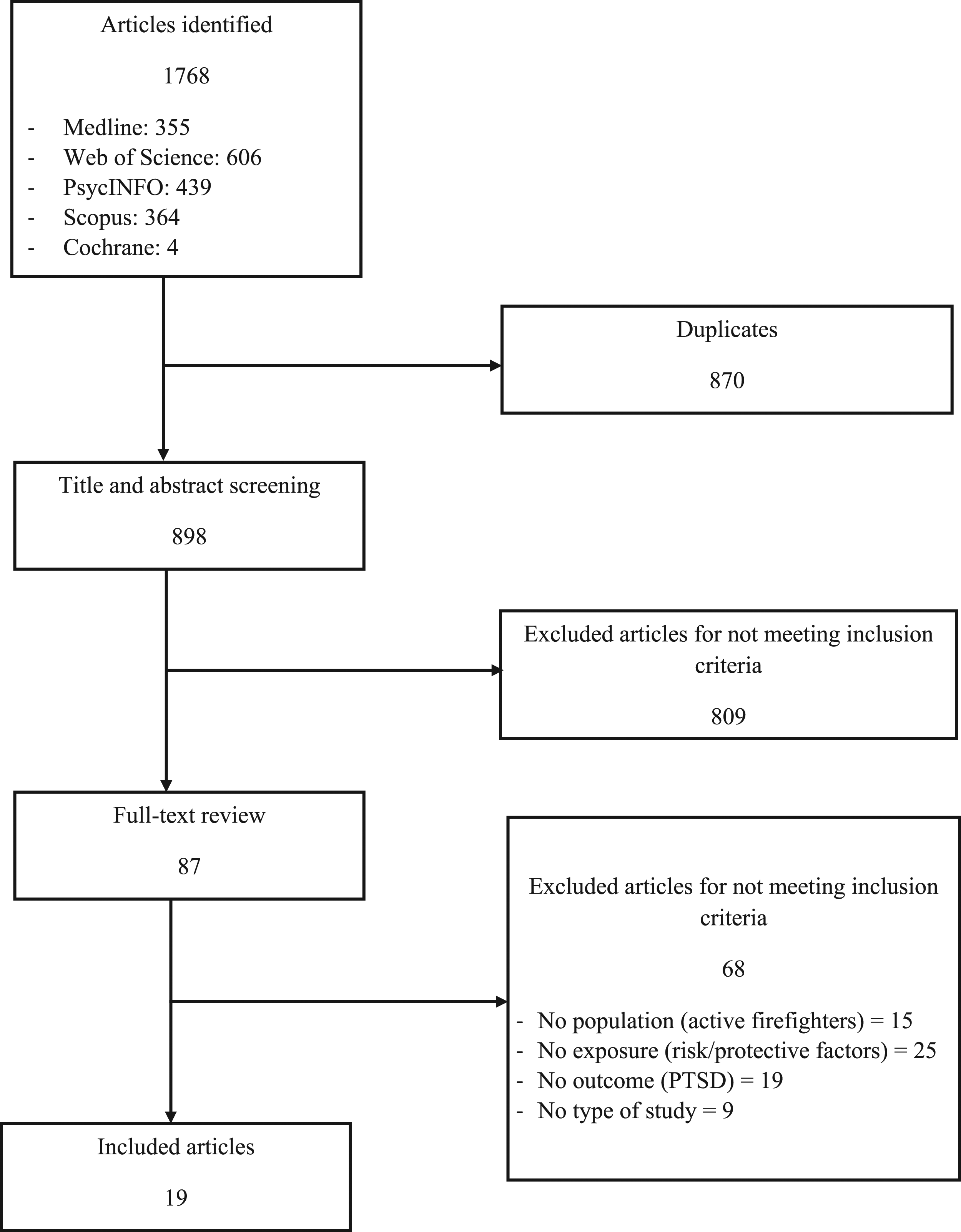
Descriptive Characteristics
Findings of the Studies Included in the Systematic Review.
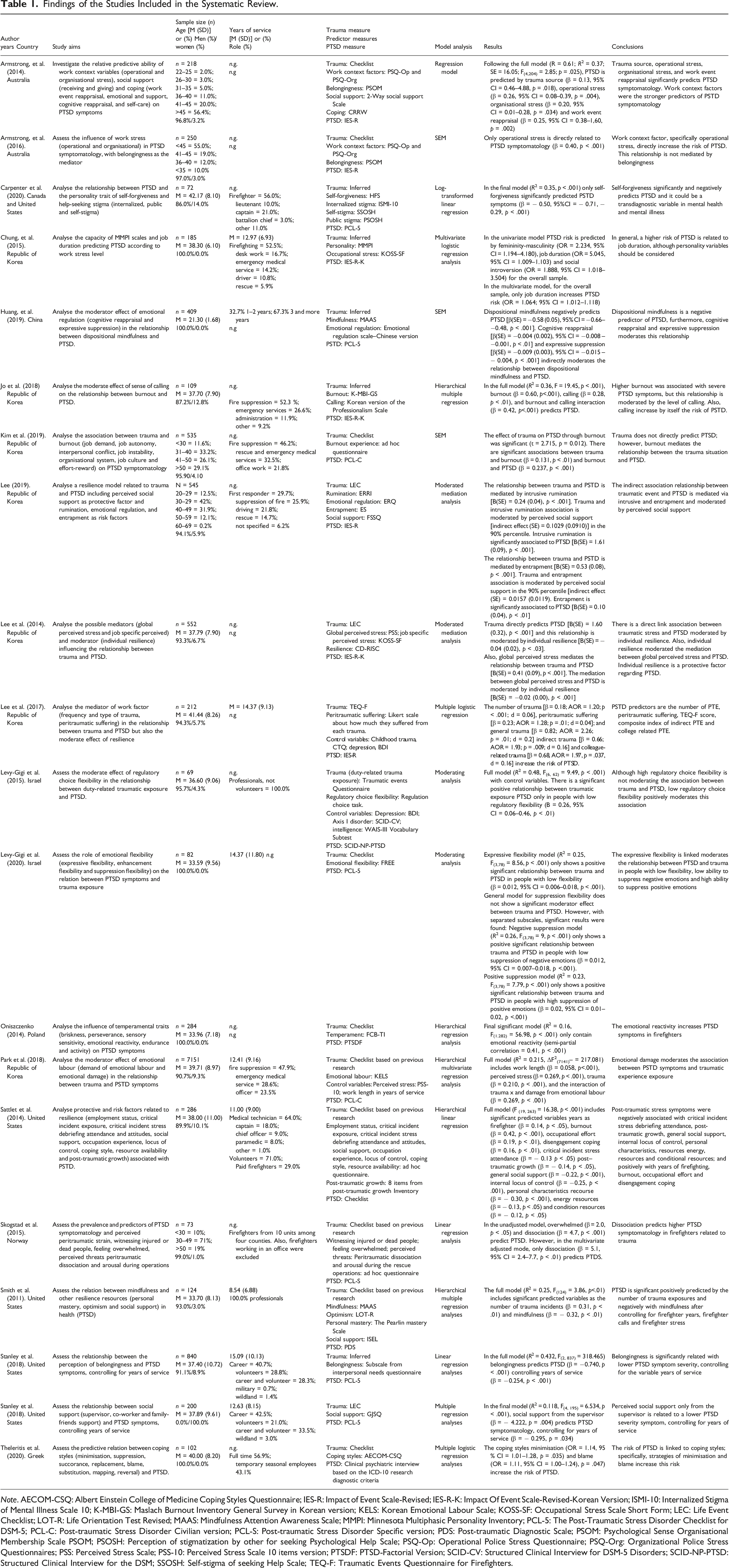
Note. AECOM-CSQ: Albert Einstein College of Medicine Coping Styles Questionnaire; IES-R: Impact of Event Scale-Revised; IES-R-K: Impact Of Event Scale-Revised-Korean Version; ISMI-10: Internalized Stigma of Mental Illness Scale 10; K-MBI-GS: Maslach Burnout Inventory General Survey in Korean version; KELS: Korean Emotional Labour Scale; KOSS-SF: Occupational Stress Scale Short Form; LEC: Life Event Checklist; LOT-R: Life Orientation Test Revised; MAAS: Mindfulness Attention Awareness Scale; MMPI: Minnesota Multiphasic Personality Inventory; PCL-5: The Post-Traumatic Stress Disorder Checklist for DSM-5; PCL-C: Post-traumatic Stress Disorder Civilian version; PCL-S: Post-traumatic Stress Disorder Specific version; PDS: Post-traumatic Diagnostic Scale; PSOM: Psychological Sense Organisational Membership Scale PSOM; PSOSH: Perception of stigmatization by other for seeking Psychological Help Scale; PSQ-Op: Operational Police Stress Questionnaire; PSQ-Org: Organizational Police Stress Questionnaires; PSS: Perceived Stress Scale; PSS-10: Perceived Stress Scale 10 items version; PTSDF: PTSD-Factorial Version; SCID-CV: Structured Clinical Interview for DSM-5 Disorders; SCID-NP-PTSD: Structured Clinical Interview for the DSM; SSOSH: Self-stigma of seeking Help Scale; TEQ-F: Traumatic Events Questionnaire for Firefighters.
The total sample comprised 12,298 active firefighters (volunteers and employees). Specifically, regarding the characteristics of the work carried out, six studies (Chung et al., 2015; Huang et al., 2019; Lee et al., 2017; Levy-Gigi et al., 2020; Smith et al., 2011; Stanley et al., 2018) reported the mean number of years participants had been employed, finding an average of 13 years (SD = 8.84), and Huang and colleagues (2019) stated that 67% of the participants had more than 3 years’ work experience. Furthermore, five papers (Chung et al., 2015; Jo et al., 2018; Kim et al., 2019; Lee, 2019; Park et al., 2018) reported the working area, showing that most of the participants worked in fire suppression (46.79%) or emergency services (21.23%). The other studies did not provide information on experience or type of job.
The majority of participants were men (90% across studies, with a range of 86–100%). One of the studies (Stanley et al., 2019; second study) comprised a sample composed only of women. Five studies (Armstrong et al., 2014, 2016; Kim et al., 2019; Lee, 2019; Skogstad et al., 2015) described age ranges, the majority being between 30–49 years of age. The other studies reported an overall mean sample age of 36.64 years. Concerning marital status, most of the participants were married (70.6%); however, several articles did not provide information in this regard.
All firefighters that formed the study sample had been exposed to at least one duty-related traumatic event, evaluated through validated self-report instruments, checklists about critical work incident exposure based on previous research, ad hoc questions about trauma or inference of trauma, since the sample comprised active personnel who work in these situations. All studies based the definition of trauma and post-traumatic symptoms of DSM-IV (Armstrong et al., 2014, 2016; Chung et al., 2015; Jo et al., 2018; Kim et al., 2019; Lee, 2019; Lee et al., 2014, 2017; Levy-Gigi et al., 2015; Oniszczenko, 2014; Park et al., 2018; Sattler et al., 2014; Skogstad et al., 2015; Smith et al., 2011) or DSM-5 (Carpenter et al., 2020; Huang et al., 2019; Levy-Gigi et al., 2020; Stanley et al., 2018), except for Theleritis et al. (2020), who used ICD-10. Specifically, seven studies (Armstrong et al., 2014, 2016; Chung et al., 2015; Jo et al., 2018; Lee, 2019; Lee et al., 2014, 2017) assessed PTSD symptoms using the Impact of Event Scale-Revised (IES-R; Weiss & Marmar, 1997) or the Korean version (IES-R-K; Eun et al., 2005); four articles (Carpenter et al., 2020; Huang et al., 2019; Levy-Gigi et al., 2020; Stanley et al., 2018) used the Post-Traumatic Stress Disorder Checklist for DSM-5 (PCL-5; Weathers et al., 2013), and two studies used the PTSD Checklist-Civilian Version (PCL-C; Weathers et al., 1994). The other studies used different validated instruments (see Table 1 for more information).
Risk of Bias Assessment
Level of Risk of Bias Assessment using QUIPS Tool.
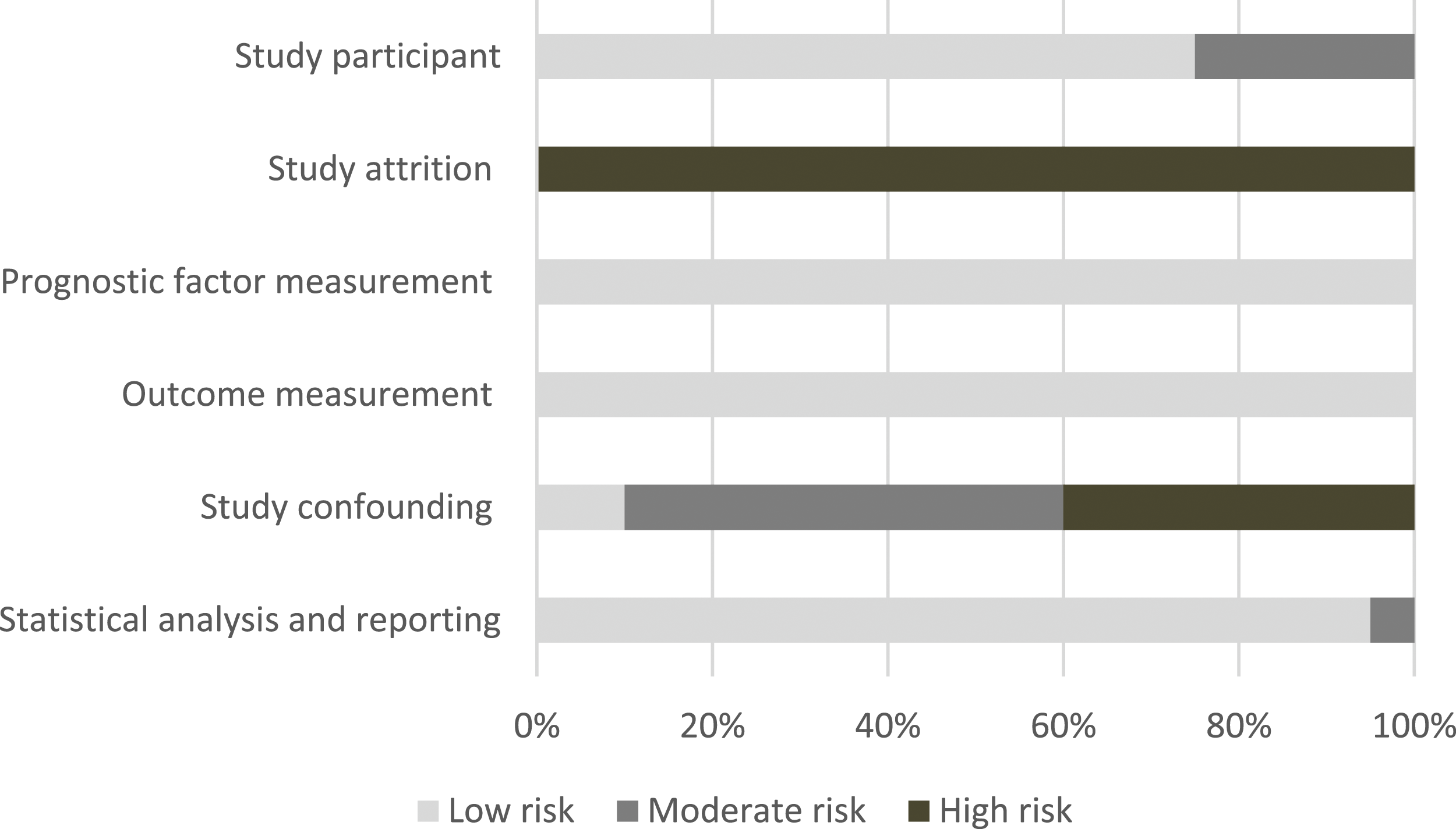
Risk of bias summary.
Synthesis of the Results for Variables Associated with the Development of PTSD in Firefighters
In this section, the evidence for each variable associated with PTSD symptoms in firefighters is presented. The studies included in this review reported very different and heterogeneous variables. Because of this, the individual results have been organized by their latent constructs in four subsections.
Variables Related to Trauma Characteristics or Work as a Firefighter
All studies reported that, to develop PTSD, firefighters have experienced at least one traumatic event. However, only two studies specifically analysed the influence of trauma characteristics on the development of PTSD (Armstrong et al., 2014; Lee et al., 2017). It was found that general traumatic life events (B= 0.54, p < .01) (Armstrong et al., 2014) and the number of traumatic events (AOR = 1.20, d = .06), peritraumatic suffering (AOR = 1.28, p = .010, d = .04), indirect experience (AOR = 1.93, d = .16) and colleague-related trauma (β = 1.97, AOR = 1.97, d = .16) were related to the development of PTSD (Lee et al., 2017).
On the other hand, seven studies reported data pertaining to work-related variables and their association with the presence of PTSD (Armstrong et al., 2014, 2016; Chung et al., 2015; Jo et al., 2018; Kim et al., 2019; Lee et al., 2014; Sattler et al., 2014). Five studies showed a relationship between work-related stress – namely, organizational and daily hassles involved in the work – and the development of PTSD (Armstrong et al., 2014, 2016; Chung et al., 2015; Lee et al., 2014; Sattler et al., 2014). Armstrong et al. (2014) identified a significant relationship between operational stress (e.g. working hours) (β = 0.26, p = .004) and organizational stress (e.g. management or excessive administration duties) (β = 0.20, p = .034). The influence of operational stress (β = 0.40, p < .001) was confirmed in a later study (Armstrong et al., 2016), and Sattler et al. (2014) also found that years of firefighting (β = 0.14, p< .05) and occupational effort (β = 0.19, p < .01) played a role. In this line, Chung et al. (2015) observed that job duration was related to an increased risk of PTSD in the whole sample (OR = 1.064, 95% CI = 1.012, 1.118). Moreover, the influence of perceived stress on PTSD [B(SE) = 0.41 (0.09), p < .001] obtained significant results (Lee et al., 2014).
Three studies examined the association of burnout with PTSD. Jo et al. (2018) and Sattler et al. (2014) showed the direct influence (β = 0.60, p < .001; β = 0.42, p < .001), and Kim et al. (2019) observed that trauma was not directly related to PTSD but a higher degree of trauma was indirectly related to PTSD through burnout as a mediator. Moreover, the interaction between burnout and sense of calling also predicted the presence of PTSD (β = 0.42, p < .001), and sense of calling with direct association (β = 0.28, p < .01) (Jo et al., 2018). Thus, the sense of calling is related to the level of satisfaction derived from an occupation that helps people who are suffering.
Maladaptive Coping Strategies
Five studies analysed the relationship between maladaptive coping strategies – that is, risk factors – and PTSD (Armstrong et al., 2014; Lee, 2019; Park et al., 2018; Sattler et al., 2014; Theleritis et al., 2020). Specifically, it has been found that intrusive rumination (B = 1.61, p < .001), entrapment (B = 0.10, p < .01) and suppression (B = 0.15, p < .05) predict PTSD (Lee, 2019). Huang et al. (2019) also observed the negative effect of expressive suppression on the development of PTSD (β = −0.25, p < .001), and Armstrong et al. (2014) showed that work event reappraisal increased the risk of PTSD (β = 0.25, p = .002). Also, the results of Skogstad et al. (2015) in the unadjusted model associated overwhelmed (β = 2.0, p < .05) and dissociation (β = 4.7, p < .001) with PTSD (this variable is also in the adjusted model). Theleritis et al. (2020) analysed coping styles: (a) minimization: a personal predisposition to de-emphasize the burden and importance of a stressful event; (b) suppression: avoiding the problem or situation; (c) succorance: asking others for help; (d) replacement: dealing with stressful situations by finding alternative solutions; (e) blame: blaming others or the ‘system’ for one’s own problem; (f) substitution: engaging in tension-reducing activities; (g) mapping: collecting information about the situation or problem; and (h) reversal: acting the opposite of the way you feel. They only found significant associations for minimization (OR = 1.14, p = .035) and blame (OR = 1.11, p = .047). Sattler et al. (2014) analysed the effect of problem-focused, emotion-focused and disengagement strategies, but only disengagement showed a significant association with PTSD (β = 0.16, p < .01).
Related to these findings is emotional labour – that is, the process by which the firefighters have to control their feelings in accordance with organizational demands and their occupational role. Park et al. (2018) studied the effect of the demands of emotional labour (β = 0.042, p = ns) and the damage of emotional labour (or severity of emotional hurt due to emotional labour) (β = −0.024, p = ns) on PTSD, but the results were not significant. However, the interaction between trauma and damage of emotional labour showed a significant association with PTSD (β = 0.269, p < 0.01).
Variables Related to Trait Characteristics
Six studies analysed the influence of various personal characteristics on the development of PTSD in firefighters (Carpenter et al., 2020; Chung et al., 2015; Huang et al., 2019; Oniszczenko, 2014; Sattler et al., 2014; Smith et al., 2011). Chung and colleagues (2015) assessed the utility of the Minnesota Multiphasic Personality Inventory (MMPI) as a related factor with PTSD according to the job stress level. In a univariate model, they observed that masculinity-femininity (OR = 2.234, 95% CI: 1.194, 4.180) and social introversion (OR = 1.888, 95%CI = 1.018, 3.504) were associated with PTSD symptoms for the overall sample. For the group with a lower job stress level, masculinity-femininity showed a significant association with PTSD (OR = 5.304, 95% CI = 1.191, 23.624). For the group with a higher job stress level, social introversion showed a significant association with PTSD (OR = 3.727, 95% CI = 1.096, 12.673).
Huang et al. (2019) analysed the influence of dispositional mindfulness, or a general tendency to attend to the present moment non-judgementally and purposefully, on the development of PTSD (β = −0.58, p < .001). Also, they found that this relationship to be mediated by the coping strategies of cognitive reappraisal (β = −0.004, p < .01) and expressive suppression (β = −0.009, p < .001). Smith et al. (2011) similarly observed the influence of dispositional mindfulness on PTSD (β = −0.32, p< .01). Moreover, optimism (β= 0.05, p= ns) and personal mastery (β = −0.08, p = ns) were analysed, but their associations with PTSD were not significant.
Finally, Carpenter et al. (2020) observed that self-forgiveness significantly predicted PTSD symptoms (β= −0.50, p < .001). Sattler et al. (2014) analysed the influence of an internal locus of control (e.g. people can take measures to reduce their risk) (β = −0.25, p < .001); personal characteristics (e.g. self-efficacy and optimism) (β = −0.30, p < .001); energy resources (e.g. physical health) (β = −0.13, p < .05); and condition resources (e.g. tenure, status and employment) (β = −0.12, p < .05). Oniszczenko (2014) observed that emotional reactivity was a significant predictor of PTSD symptoms in firefighters [F = 56.98, df = 1.282, p < .000].
Adaptative Strategies or Protective Factors
Ten studies analysed the association between PTSD and adaptative strategies, that is, protective factors against PTSD (Armstrong et al., 2014, 2016; Huang et al., 2019; Lee, 2019; Lee et al., 2014; Levy-Gigi et al., 2015, 2020; Sattler et al., 2014; Smith et al., 2011; Stanley et al., 2018). Belongingness and perceived social support were the most examined adaptative coping strategies, analysed in seven studies.
Three studies analysed the influence of belongingness on the development of PTSD. Armstrong et al. (2014) found that belongingness, giving social support and receiving social support explained 37% of PTSD variance. However, these variables did not obtain significant results separately or mediate the relationship (Armstrong et al., 2016). Stanley et al. (2018) showed that greater levels of belongingness were significantly associated with lower overall symptoms of PTSD (β = −0.740, p < .001), controlling for years of service.
Regarding social support, four studies showed results analysing the relationship between this variable and PTSD, throwing up controversial data. It was shown that general support (β = −0.22, p < .001) predicted PTSD (Sattler et al., 2014). Concretely, greater levels of perceived social support by co-workers (β = −4.465, p < .001), supervisors (β = −4.615, p < .001) and family/friends (β = −3.206, p = .021) were significantly associated with lower overall PTSD symptoms (Stanley et al., 2018). However, entering the three types of social support into a single model, only support from supervisors remained significant (β = −4.222, p = .004). Conversely, Smith et al. (2011) found that social support did not present significant results in the association with PTSD (β = −0.09, p = ns). Also, Lee (2019) observed that social support did not have a direct effect on PTSD, but high levels of social support protected firefighters from developing PTSD via resistance rumination (B = 0.1029, p < .01) and entrapment (B = 0.0157, p < .01).
Three studies analysed the effect of adaptative strategies related to emotional regulation in PTSD. Huang et al. (2019) showed that cognitive reappraisal protected firefighters from the development of PTSD (β = −0.15, p < .01). Levy-Gigi et al. (2015) studied the joint influence of duty-related traumatic exposure with regulatory choice flexibility on PTSD, in that high exposure individuals with high regulatory flexibility had significantly fewer PTSD symptoms compared with those with low regulatory flexibility (β = 0.26, p < .01). Levy-Gigi et al. (2020) also observed that expressive flexibility (β = −2.26, p < .01) and the interaction between this variable and duty-related traumatic exposure (β = −0.004, p < .05) had a protective effect on the development of PTSD. To evaluate the magnitude of the last association, analyses were conducted separately for individuals with low (β = 0.012, p < .01) and high (β = 0.001, p = ns) expressive flexibility.
Finally, one study analysed the protective effect of resilience on the development of PTSD. Lee et al. (2014) observed that a greater number of traumatic events and a greater level of perceived stress increase the probability of developing PTSD. However, firefighters with a high level of resilience (upper 50th percentile) were less vulnerable to PTSD (B(SE) = 1.61 (0.1191), p < .001). There was a direct effect of traumatic events on PTSD, but firefighters with resilience scores above the 75th percentile were less vulnerable (B(SE) = 1.13 (0.3929), p < .001).
Discussion
Although the association between trauma experience and PTSD is well known, the mechanisms by which this problem develops in emergency workers following such an event have yet to be fully established. This systematic review aimed to identify the risks and protective factors associated with PTSD in active firefighters. The synthesis of the results shows that several factors can be significantly associated with this disorder, acting as diathesis or vulnerability variables. However, the evidence is moderate due to the small number of studies carried out with each of the variables.
Variables Related to Trauma Characteristics or Work as a Firefighter
There was moderate evidence (seven articles analysed) that work-related factors were relevant. On the one hand, five studies show that more perceived stress, both general and occupational, is a predictor of PTSD – operational and organizational, but, to a greater extent, operational. This is consistent with studies among police officers that found that work stressors were associated with PTSD symptoms, and these effects were independent of the effects of cumulative trauma exposure (Liberman et al., 2002). On the other hand, there is moderate evidence that burnout is related both directly and indirectly to PTSD, as in other emergency workers (e.g. Chatzea et al., 2018). It was found, albeit with weak support, that this variable could interact with the sense of calling to increase the predicted percentage of PTSD. If these results are corroborated in future research, perhaps it can be ascertained whether firefighters with a higher vocation are more involved in their work, which can generate greater personal dedication and so lead to higher levels of stress or feeling overwhelmed; it is highlighted, in line with this hypothesis, that feeling overwhelmed has been associated with PTSD in this review, although with weak support.
In addition, with moderate support, it has been found that job duration (years of firefighting) predicts PTSD, perhaps because there is greater exposure to traumatic events over more years of service. In line with this, it has been found that police officers’ cumulative exposure to traumatic situations increases the risk of developing PTSD and/or symptom severity of PTSD (Marmar et al., 2006), contributing to the development of this problem over time as a ‘building block effect’ (Kolassa et al., 2018). This effect could also occur not only with direct trauma: the literature has shown that indirect experience and colleague-related trauma also predict PTSD, as established by the DSM-V (APA, 2013). These results could confirm the negative effect of vicarious trauma or secondary traumatic stress, as shown in the literature (see Greinacher et al., 2019). Furthermore, also with limited evidence, the reviewed studies found that the number of personal/work traumas suffered predicts PTSD, showing a possible cumulative effect of trauma. It is noteworthy that firefighters, in addition to being exposed to occupational traumas, may suffer these situations in their personal lives, which may increase the accumulated trauma (Del Ben et al., 2006). To corroborate these hypotheses, these results must be confirmed in firefighters in future investigations.
Variables Related to Coping to Trauma Exposure
It has been found that the way in which firefighters cope with traumatic events could predict PTSD. However, the evidence is moderated since great heterogeneity has been found in the variables examined in the different studies. Regarding emotional regulation strategies, two studies showed that rumination on a work event predicted post-traumatic symptoms. This is not surprising, because rumination processes have been established as a transdiagnostic variable included in the context of PTSD, which makes emotional regulation difficult (Moulds et al., 2020). On the other hand, a further two studies found that expressive suppression could predict PTSD as well as, dissociation, disengagement and minimization. It has been suggested that avoidance strategies limit the capacity to encode and process the trauma memory, which is a crucial variable in the development and maintenance of PTSD and recovery from the problem (e.g. Tull et al., 2020).
In this line, the review found that an experience of peritraumatic suffering and/or feeling overwhelmed was associated with the development of PTSD. It is possible that these emotions make it difficult for the person to implement skills of emotional regulation and management of the situation (Terry et al., 1995), thereby establishing maladaptive coping strategies. Other emotional aspects, including a sense of entrapment; a perception of situations, feelings and cognitions being uncontrollable and inescapable; damage from emotional labour (difficulties controlling feelings in agreement with structural demands and work-related roles); or feeling blame are predicted variables of PTSD. Although firefighters might wish to escape exposure to traumatic events, it is challenging to do so when rushing to the scene of traumatic accidents is a requirement of the job. Due to the inherent conditions of their work, firefighters cannot escape traumatic situations. They must make an effort to control their emotions in relation to their job requirements, and to a greater extent if they present post-traumatic symptoms (Paltell et al., 2019). All this could generate negative emotions, derived from both the circumstances and from having these feelings. However, more research is necessary to examine these aspects because the evidence is scarce. This review has only been able to find specific articles that talk about it – that is, isolated investigations.
In respect of protective factors, this systematic review found, with moderate support, that a highlevel of belongingness significantly predicted lower post-traumatic symptoms, similar to, for example, veterans (Kintzle et al., 2018). Also, according to the results, social support from supervisors is associated with low PTSD symptoms. Furthermore, it was shown that the indirect link associating traumatic events and PTSD symptoms via event-related intrusive rumination and entrapment is moderated by perceived social support. Although the literature points in this direction in other populations and disorders (see Guilaran et al., 2018), Smith et al. (2011) found no direct significant association between social support and PTSD. This may be due to the variables that make up the prediction model, since the most relevant for this author was trait mindfulness. Huang and colleagues (2019) also found that high dispositional mindfulness predicted lower PTSD, both directly and by showing that greater mindfulness predicts greater cognitive reappraisal and less expressive suppression, which leads to lower levels of PTSD. Thus, two studies were found that analysed this question. Although the evidence found in relation to mindfulness is limited, the data could suggest that this variable may improve self-regulation and emotional regulation (Coffey & Hartman, 2008), and diminish avoidance or inhibition coping strategies that precipitate PTSD in firefighters.
In terms of other protective factors against the development of PTSD in this situation, with weak support, it was found that cognitive reappraisal could be an emotional regulation strategy that reduces PTSD because it decreases experience and emotional expression (Gross, 2002). Although this evidence is limited in firefighters, in populations such as war veterans (Boden et al., 2013) or workers exposed to traumatic situations (Shepherd & Wild, 2014), among others, within the strategies focused on the antecedents of emotion, there seems to be unanimity in showing that the use of cognitive reappraisal is related to fewer post-traumatic symptoms. However, in this review, Levy-Gigi and colleagues (2015) showed that a high degree of regulatory choice flexibility could be an important protective variable for PTSD. As in previous studies, flexibly choosing regulatory options could be the best adaptive coping strategy because the individual can adapt to the different demands of each context (Sheppes & Levin, 2013). On the other hand, a single study was found that analysed other variables. As Agaibi and Wilson (2005) also showed in other populations, post-traumatic resilience is a type of adaptive behaviour to a stressful situation in firefighters, which includes recovery from PTSD to optimal conditions of functioning (Stanley et al., 2018). Also, self-forgiveness and an internal locus of control negatively predicted PTSD. High levels of both variables are related to better mental health in populations such as the military (Carpenter et al., 2020; Karstoft et al., 2015).
As has been explained, some of the risk and protective factors are shared by firefighters and other first responders or war veterans. In war veterans, cognitive reappraisal (Boden et al., 2013) or belongingness (Kintzle et al., 2018) have been shown to be protective of PTSD. In police officers, a systematic review (Wagner et al., 2020a, 2020b) showed that individual variables (e.g. years of service) have weak or non-existent relationships with PTSD, while organizational variables (e.g. low support form supervisor) are possible contributors, and trauma characteristics (e.g. number of traumas or severity of exposure) are more strongly associated with PTSD. However, no studies with other emergency workers were found to identify other variables observed in firefighters (e.g. belongingness, cognitive reappraisal, dispositional mindfulness, etc.). Given that they share assistance in emergency situations, it is not surprising that they share some risk and protection variables, but others may not coincide because each group has different competencies, functions, organizations, etc. A more systematic and rigorous body of research is necessary to analyse which variables are associated with PTSD in firefighters and if these variables are pertinent in other emergency groups.
Limitations, Implications, and Conclusions
Several limitations should be considered in the conclusions of this review. Firstly, the variance in the assessment of PTSD and DSM criteria used to diagnose post-traumatic stress symptoms (DSM-IV-TR or DSM-5) should be mentioned; this means that the sample may differ in the symptomatology. Secondly, there is high heterogeneity in the variables evaluated (and the assessment instruments) in the different studies. So, the review considers a very high number of variables, but it is not possible to draw conclusions about them. Thus, the variability of results is a critical source of inconsistency across the literature, with implications for accurate detection of risk/protective factors for PTSD in firefighters. Thirdly, the studies reviewed did not inform about participants who refused to participate (study attrition); because of this bias, it may not be guaranteed that the sample is generalizable. Finally, the sample was comprised predominantly of men; for this reason, these data cannot be fully extrapolated to female firefighters, since the sample may not be representative. The firefighter population is mainly formed by men (Danbold & Bendersky, 2020), so it is hard to achieve representative rates of the firefighter population balanced by sex. However, sex-based differences may mediate the effects of post-traumatic symptomatology (Olff, 2017) and the variables could operate differently. More research is needed with female firefighters to explore this question.
Ethnic and cultural differences were not specified in the studies. Scientific literature has highlighted the higher risk for certain racial/ethnic minority firefighters’ populations of showing mental health diseases (Poston et al., 2014). Bearing this in mind, studies must include interpersonal differences, allowing the study of their moderator effect but also facilitating the improvement of equality policies and strategies.
Critical findings of the review.
Implications for Research, Practice and Policy.
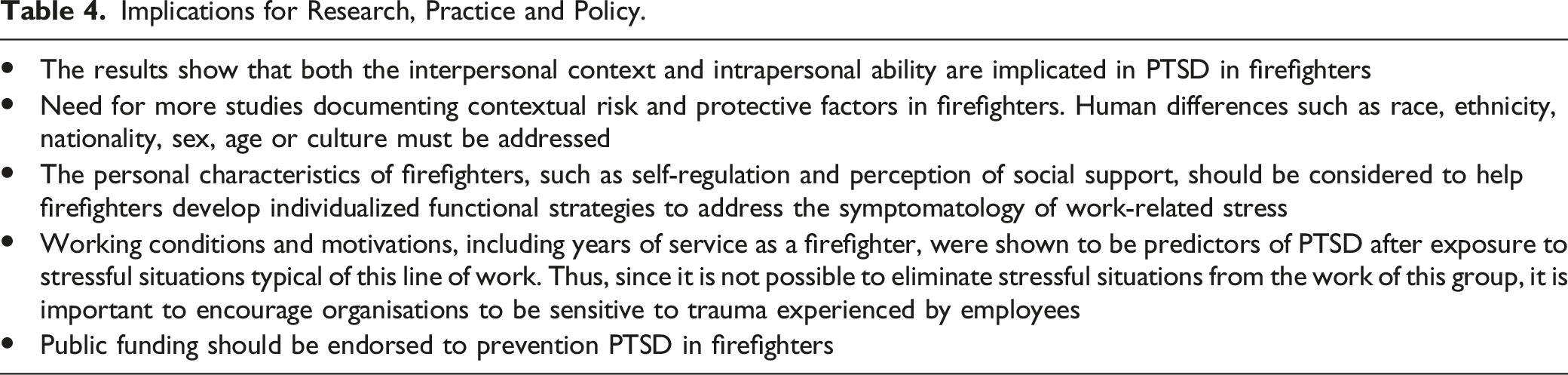
Although there is little research in this direction, this review analyses the available literature, highlighting this fact for future research on the subject. Continuing to investigate this matter will allow us to design primary and secondary prevention actions to help those who help.
Footnotes
Acknowledgements
The project leading to these results has received funding from ‘la Caixa’ Foundation (ID 100010434), under agreement <FUI1 - PI010>
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the from ‘la Caixa’ Foundation (ID 100010434) under Grant FUI1 - PI010.