
Abstract
Serving military personnel and veterans are known to be at elevated risk of post-traumatic stress disorder (PTSD), and some veterans have been shown to respond poorly to current standard treatments. Evidence so far suggests that according to the 11th edition of the International Classification of Diseases and Related Health Problems guidelines, complex PTSD (CPTSD) may be of higher prevalence in the general population than PTSD. The aim of the study was to investigate the prevalence of CPTSD compared to PTSD in serving and ex-serving military populations. A systematic review was conducted with the search criteria set to peer-reviewed English language journal articles, focusing on serving military or veteran populations, reporting on the prevalence of CPTSD, not restricted by year. Four comprehensive databases (Psycinfo, Pubmed, CINAHL, and Embase) were searched. Of the 297 identified articles, 16 primary studies were eligible for inclusion. The review was registered in the PROSPERO database (CRD42023416458), and results were reported based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Of the 16 studies, 13 demonstrated higher prevalence of CPTSD than PTSD. Studies were predominantly veteran focused. Prevalence of CPTSD ranged from 5% to 80.63%, while prevalence of PTSD ranged from 3.8% to 42.37%. There was high heterogeneity in study populations, preventing meta-analysis. This is the first systematic review to assess the prevalence of CPTSD in serving military and veteran populations, with the findings demonstrating a higher rate of CPTSD compared to PTSD. It is hoped that the review will assist clinicians and military and veteran health services with appropriate assessment, diagnosis, and intervention for those affected by CPTSD, as well as PTSD.
Introduction
According to the 2021 census, almost 600,000 Australians have served, or are currently serving in the Australian Defence Force (ADF) with 84,865 currently serving and 496,276 veterans recorded at that time (Australian Bureau of Statistics, 2021). Mental health disorders are known to be a prominent issue in both serving and veteran communities. The 2018 Mental Health Prevalence Report estimated that almost three out of four transitioned ADF members have met criteria for a mental disorder in their lifetime (Van Hooff et al., 2018). Further to this almost one in four transitioned ADF members was estimated to have met criteria for a post-traumatic stress disorder (PTSD) diagnosis. Rates of PTSD have also been demonstrated to be higher in deployed than non-deployed veterans in studies from the United Kingdom, Canada, the United States of America, and Australia (Hoge et al., 2014; Stevelink et al., 2018; Thompson et al., 2016; Van Hooff et al., 2018).
There is evidence to demonstrate that some veterans do not respond as well to standard treatments for PTSD compared to members of the general public (Kitchiner et al., 2012). This presents obvious problems given the elevated rates of PTSD in this population. There is therefore a need to understand the complexities and contributing factors in order to better understand and treat PTSD in military and veteran groups. There has been some evidence to demonstrate poorer response to treatment associated with factors such as PTSD severity, mental health co-morbidities, and childhood adversity (Murphy & Smith, 2018; Phelps et al., 2018; Richardson et al., 2014). However, the current understanding of PTSD may be limiting treatment outcomes.
In the 11th edition of the International Classification of Diseases and Related Health Problems (ICD-11), significant changes have been made to those disorders termed “specifically associated with stress” (World Health Organization, 2022). The established diagnosis of PTSD is joined by a related one, namely complex PTSD (CPTSD). CPTSD has its origins in the seminal work of Herman (1992). Herman posited that PTSD was not sufficient in its classification to embody the true multifaceted symptomatology expressed by individuals who had experienced prolonged and sustained traumatic life events; particularly those which had occurred in early and formative years. As specified in ICD-11, CPTSD retains the core diagnostic components of PTSD (characterized in ICD-11 by three symptom groupings of re-experiencing of trauma, avoidance of traumatic reminders, and a heightened sense of threat), and indeed in order to receive a diagnosis of CPTSD, the PTSD criteria must be met. In addition to these criteria, symptoms must be present in three additional areas of disturbances in self-organization (DSO), comprising symptom groupings of (a) severe difficulties with affect regulation, (b) persistent negative self-image or concept, and (c) persistent difficulties in interpersonal relationships (Cloitre et al., 2013). Both the symptoms of PTSD and DSO must correspond to functional impairment (World Health Organization, 2022). Although the PTSD criteria must be met it should be noted that these are intended to be mutually exclusive diagnoses. A more restrictive approach to the PTSD diagnosis is taken by the ICD-11 (Brewin et al., 2017), which results in lower prevalence estimates (Wisco et al., 2016) compared to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), in which CPTSD is not included (American Psychiatric Association, 2013). The ICD-11 therefore provides a way of distinguishing those with more complex presentations.
Research into the prevalence of CPTSD as defined by ICD-11 criteria is now emerging. The International Trauma Questionnaire (ITQ) is a validated measure for assessment of CPTSD as defined by ICD-11 (Cloitre et al., 2018). Initial studies with this measure have demonstrated marginally higher rates of CPTSD than PTSD in the general population in the United States (Cloitre et al., 2019). Further studies have shown higher rates of CPTSD than PTSD in a trauma-exposed population sample in the United Kingdom (Karatzias, Hyland, et al., 2019) and in treatment-seeking adults (Karatzias et al., 2017). Exposure to childhood trauma and multiple trauma exposures have also been demonstrated to be significant risk factors for CPTSD (Karatzias et al., 2017). There is evidence to suggest serving personnel and veterans have a higher chance of having been exposed to childhood trauma with high rates of pre-service adversity (Murphy et al., 2019). Given this, as well as the fact that combat veterans are commonly exposed to multiple traumatic war zone experiences, it is conceivable that veterans may be at elevated risk of CPTSD.
There is existing evidence suggesting that there are differences in treatment modalities effective for PTSD and CPTSD (Karatzias, Murphy, et al., 2019). While others have argued there is insufficient evidence to support this (De Jongh et al., 2016), it is clear that understanding the prevalence of CPTSD may be beneficial in guiding identification of veterans and serving personnel less likely to respond to standard PTSD treatments. Differentiating between CPTSD and PTSD is also important in order to fully understand the extent and implications of each individual’s history of trauma and to subsequently tailor treatments to their individual needs.
Aims
This study aimed to investigate the prevalence of CPTSD within current-serving military and veteran populations. The review also aimed to compare the prevalence of PTSD within the study populations where this data was available. This is the first systematic review to investigate the prevalence of CPTSD in these populations.
Methodology
The findings of this review were reported in accordance with The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). See Supplemental File 1 for the PRISMA checklist. The review protocol was registered with and approved by PROSPERO (CRD42023416458), the international prospective register for systematic reviews. PROSPERO was also searched to ensure that a systematic review in this area was not already underway. No ethics approval was required.
Data Sources and Search Strategy
Four databases (Psycinfo, Pubmed, CINAHL, and Embase) were searched up to and including April 6, 2023 with no start date, to identify relevant articles. Searches were carried out using the following terms:
Veteran and military terms: “veteran*” OR “military” OR “ex-military” OR “soldier*” OR “defence” OR “defense” OR “serving personnel” OR “servicem*n” OR “armed forces”
CPTSD terms: “C*PTSD” OR “CPTSD” OR “complex PTSD” OR “complex post*traumatic stress disorder”
These were then combined in the format 1 AND 2.
Eligibility Criteria
Studies were included if they
Included serving military or veteran populations.
Reported the prevalence of CPTSD (consistent with ICD-11 diagnostic criteria; World Health Organization, 2022) or had sufficient data to calculate this.
Were published in English with full-text version readily available.
Exclusion criteria were as follows:
Papers classified as reviews, commentaries, presentations or book reviews, and studies conducted in other populations.
Studies where the CPTSD diagnosis did not reflect the ICD-11 diagnostic criteria.
Gray literature.
Data Extraction and Study Selection
Databases were searched independently by two authors (R.G. and M.K.). Literature references were exported to EndNote where duplicates were identified and removed. Studies were screened using a two-stage process: based on title and abstract initially within EndNote, with full texts sought for articles deemed eligible for further review. After final identification of those articles meeting the selection criteria, the lists were compared by the two authors with disagreements resolved by discussion. The wider research team was available for further discussion if needed but was not required. The following data were extracted from all included studies: author names, study setting and location, sample size and population, year of publication, CPTSD and PTSD measure utilized, prevalence of CPTSD, and where available PTSD prevalence. Other demographics and variables presented in the included studies were also extracted in order to identify any findings suggesting potential moderators or risk factors for the prevalence of CPTSD.
Data Analysis
Included articles were read with all relevant data then synthesized for the review including use of tables where appropriate. Discussion of the data then occurred, primarily focusing on the prevalence of CPTSD and PTSD within the studies but also addressing other variables of interest which were identified. A meta-analysis was not completed due to significant heterogeneity within the study populations therefore narrative synthesis was undertaken.
Quality of Studies
All studies were critically assessed for suitability for inclusion using the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data (JBI Checklist; Munn et al., 2020). This critical appraisal tool is widely used and is considered appropriate in studies of this type (Ma et al., 2020). All studies were assessed as being valid for inclusion based on the domains in the JBI Checklist. The table showing the outcomes from this assessment can be found at Supplemental File 2.
Results
As shown in Figure 1, from a yield of 297 records, 173 were screened on title and abstract and 41 records underwent full-text review. Eighteen of these articles met eligibility criteria and were deemed suitable for inclusion using the JBI Checklist. However, 2 of the 18 were secondary analysis papers of primary papers already included; therefore, this left 16 primary studies included in the review.
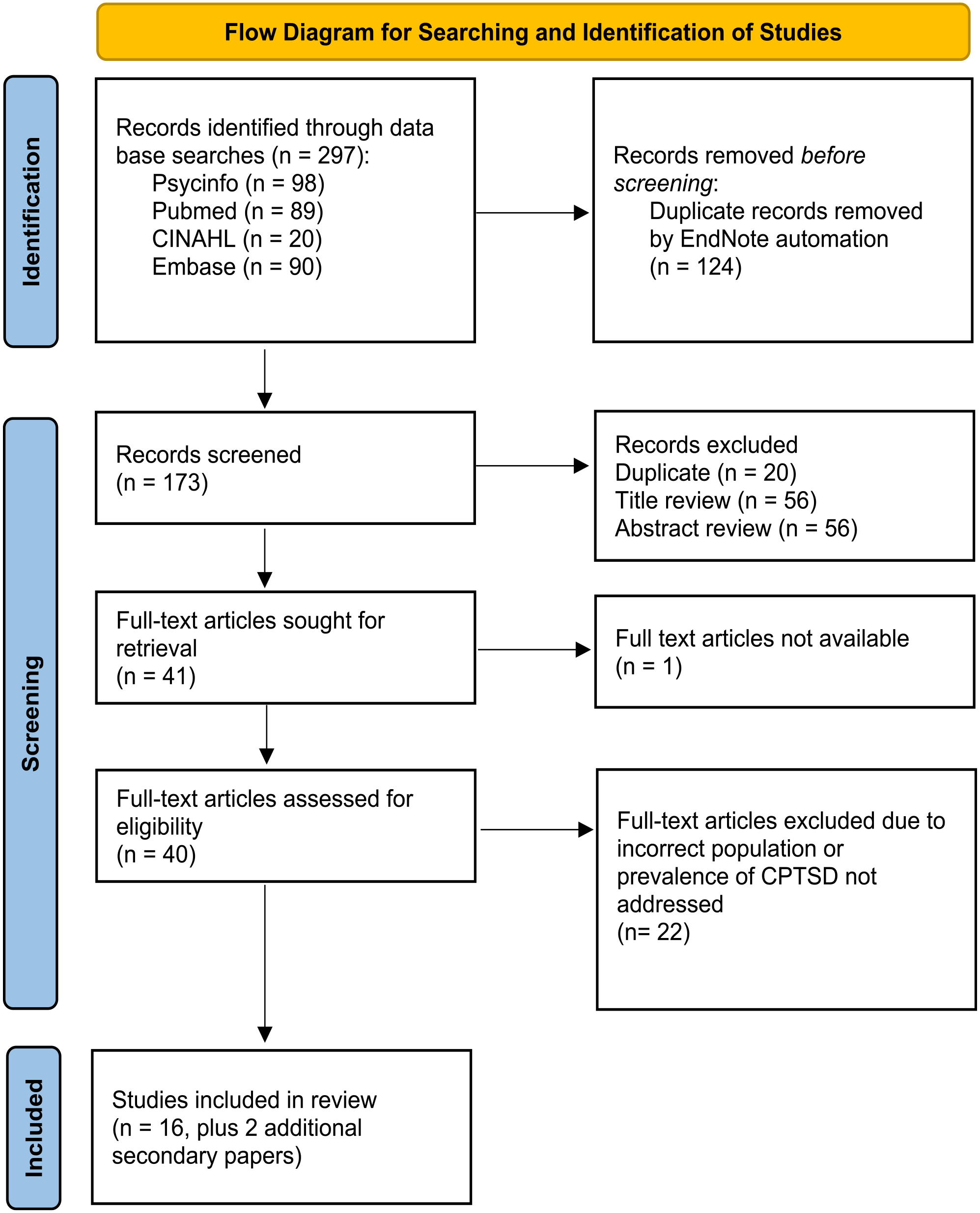
PRISMA flow diagram.
Study Characteristics
The characteristics for the 16 included studies are provided in Table 1 (together with the two secondary analyses). Country of origin was variable with studies included from seven countries, with the United Kingdom contributing the highest number of studies. Study samples ranged in size from 160 to 2,353 (not including civilians). Mean age across all studies ranged from 26 to 63.8 and was not reported in four studies. Studies were predominantly veteran focused with 15 of 16 containing veteran populations and only two (Howard et al., 2021; Mordeno et al., 2019) assessing current-service personnel. All studies providing population data were male dominated other than one Israeli study focusing on female veterans (Zerach & Levi-Belz, 2023; Zerach et al., 2019).
Study Characteristics and Data.
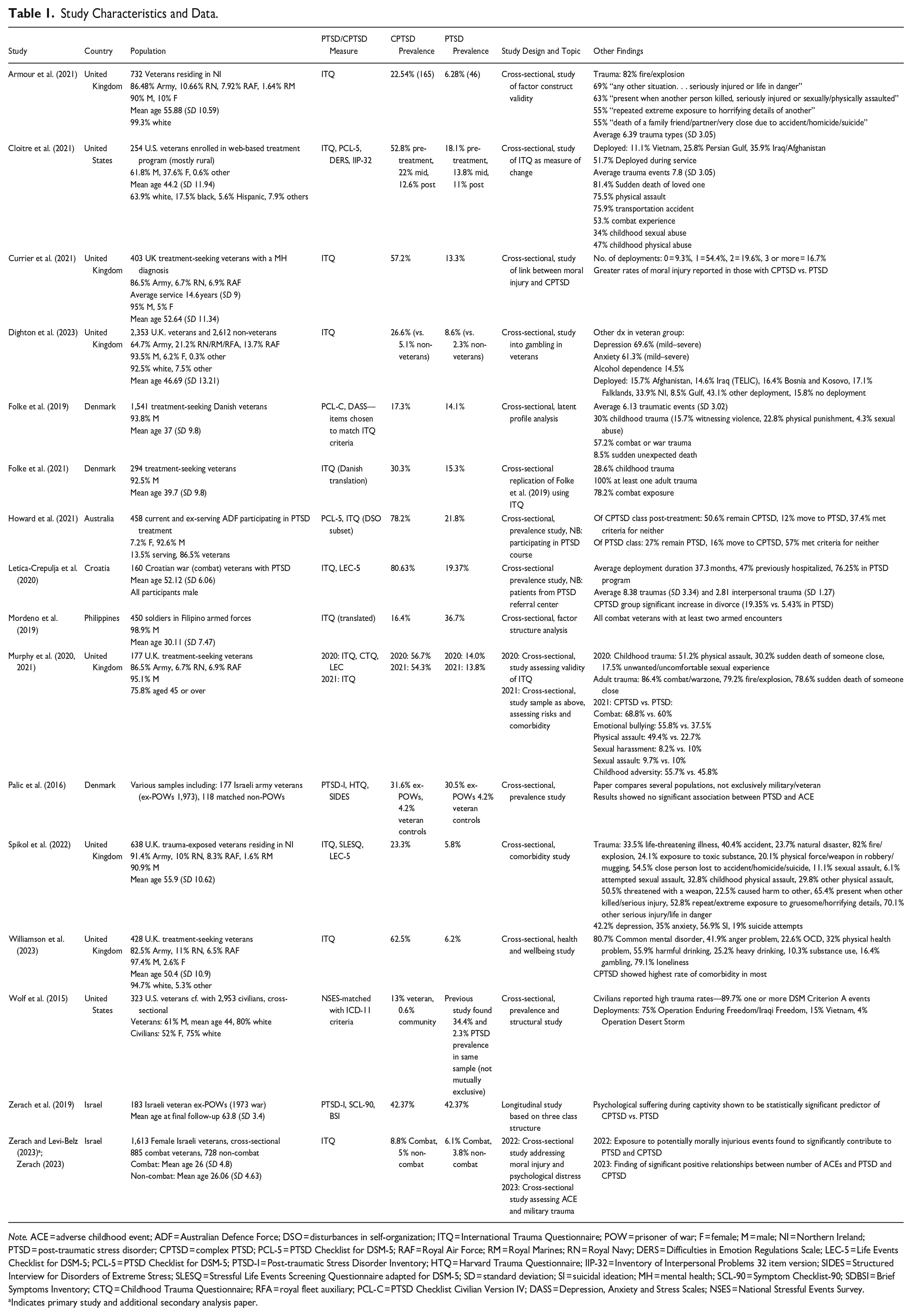
Note. ACE = adverse childhood event; ADF = Australian Defence Force; DSO = disturbances in self-organization; ITQ = International Trauma Questionnaire; POW = prisoner of war; F = female; M = male; NI = Northern Ireland; PTSD = post-traumatic stress disorder; CPTSD = complex PTSD; PCL-5 = PTSD Checklist for DSM-5; RAF = Royal Air Force; RM = Royal Marines; RN = Royal Navy; DERS = Difficulties in Emotion Regulations Scale; LEC-5 = Life Events Checklist for DSM-5; PCL-5 = PTSD Checklist for DSM-5; PTSD-I = Post-traumatic Stress Disorder Inventory; HTQ = Harvard Trauma Questionnaire; IIP-32 = Inventory of Interpersonal Problems 32 item version; SIDES = Structured Interview for Disorders of Extreme Stress; SLESQ = Stressful Life Events Screening Questionnaire adapted for DSM-5; SD = standard deviation; SI = suicidal ideation; MH = mental health; SCL-90 = Symptom Checklist-90; SDBSI = Brief Symptoms Inventory; CTQ = Childhood Trauma Questionnaire; RFA = royal fleet auxiliary; PCL-C = PTSD Checklist Civilian Version IV; DASS = Depression, Anxiety and Stress Scales; NSES = National Stressful Events Survey.
Indicates primary study and additional secondary analysis paper.
The study samples varied, with 8 of the 16 studies involving participants who were either treatment seeking or in a treatment program. Three of the studies appeared to be more representative of the wider veteran/serving population while three others only included participants with a background of combat, trauma, or experience of being a prisoner of war (POW). There was a further comparison of former POWs with non-POWs (Zerach et al., 2019), and one study (Zerach, 2023; Zerach & Levi-Belz, 2023) assessed combat exposed versus non-combat exposed veterans.
Outcome Measures
The ITQ was the primary measure used for assessing rates of PTSD and CPTSD in 12 of the 16 studies included. The ITQ is an 18-item, self-report diagnostic measure of the core features of PTSD (questions 1–9) and CPTSD (questions 10–18). It has shown consistency with the principles of ICD-11 and demonstrated diagnostic rates in line with prior findings for both diagnoses (Cloitre et al., 2018).
Prevalence Estimates
Study prevalence values were calculated based on probable diagnoses of PTSD and CPTSD using the measures as above. Full results are presented in Table 1. Prevalence of CPTSD ranged from 5% (in non-combat Israeli veterans; Zerach & Levi-Belz, 2023) to 80.63% (in Croatian war veterans with existing diagnosis of PTSD; Letica-Crepulja et al., 2020). Prevalence of PTSD ranged from 3.8% (in non-combat Israeli veterans; Zerach & Levi-Belz, 2023) to 42.37% (in Israeli veteran ex-POWs; Zerach et al., 2019). In 13 of the 16 studies the prevalence of CPTSD was higher than PTSD, with one study demonstrating equal prevalence (Zerach et al., 2019) and one study not reporting a valid prevalence of PTSD (Wolf et al., 2015). As can be seen in Figure 2, the differences between the two values are often substantial. Only one study demonstrated a PTSD prevalence greater than that of CPTSD, with that study focusing on active serving Filipino soldiers (Mordeno et al., 2019). In this case a pooled prevalence is not appropriate due to the heterogeneity associated with these studies. Table 2 outlines the critical finding from this study.
Summary of Critical Findings.
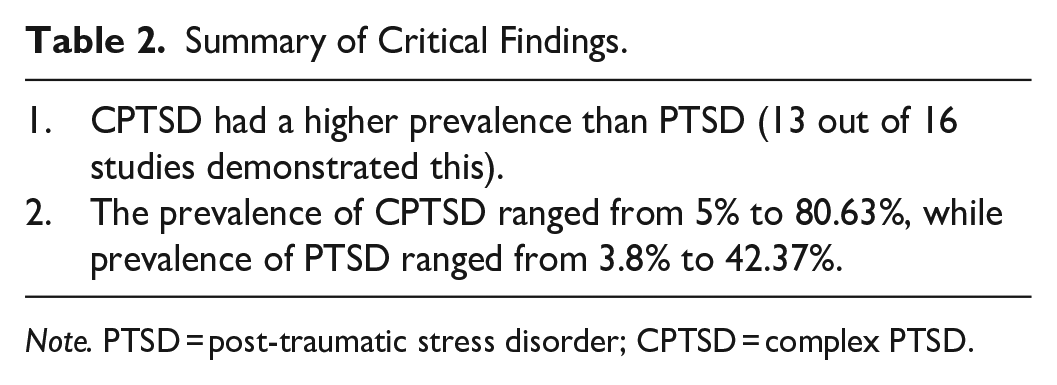
Note. PTSD = post-traumatic stress disorder; CPTSD = complex PTSD.
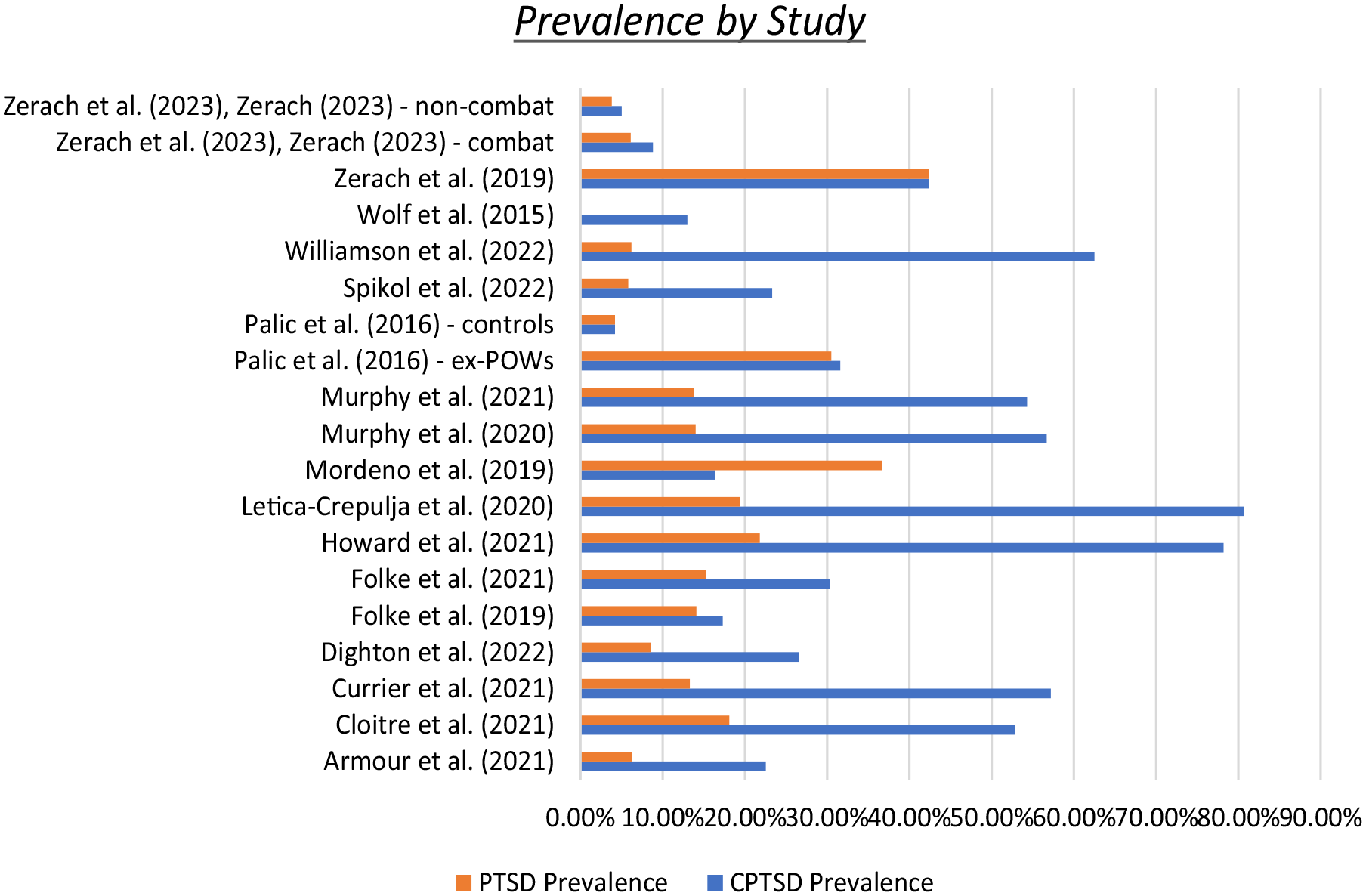
Prevalence of PTSD and CPTSD by study.
Other Findings
A number of other findings of interest were extracted. In regard to the role of childhood adversity, the results were mixed. Murphy et al. (2021) contrasted trauma types in those with each diagnosis, demonstrating higher rates of childhood adversity and more experiences of emotional or physical bullying in their military careers in the CPTSD group. Palic et al. (2016) were able to demonstrate no significant association between these diagnoses and adverse childhood events (ACEs), whereas Zerach (2023) conversely found significant positive relationships between ACEs and both PTSD and CPTSD.
The role of moral injury (MI) was also explored in some studies. Zerach et al. (2019, 2023) demonstrated that psychological suffering during captivity is a significant predictor of CPTSD versus PTSD, and that morally injurious events are a significant contributor to both. Currier et al. (2021) also studied MI but found evidence of greater MI in those with CPTSD versus PTSD.
Williamson et al. (2023) found that those with CPTSD showed higher rates of most mental health co-morbidities compared with those with PTSD. Letica et al. (2020) found a significant increase in divorce in those with CPTSD versus PTSD.
Discussion
The purpose of this systematic review was to investigate the prevalence of CPTSD in serving military and veteran populations. This is the first systematic review to assess the prevalence of CPTSD in these populations. In 13 of the 16 primary studies, the prevalence of CPTSD was higher than that of PTSD. While in some cases the difference between the two values is small, in others it was profound. Although this area of research is still emerging, due to the relatively recent change to the diagnosis of CPTSD, it appears likely that in veteran groups the prevalence of CPTSD may indeed be higher than that of PTSD. While there is awareness of the high prevalence of PTSD in veteran communities, this presents obvious implications in care and treatment as CPTSD may not be routinely considered or assessed for.
In terms of measures used to estimate prevalence, 12 of the 16 studies utilized the ITQ, an established and reliable self-report measure (Cloitre et al., 2018). As noted by Currier et al. (2021) the ITQ was not designed to make a diagnosis without a clinical interview, and it is important therefore to be aware that the diagnoses in these studies were not clinician confirmed. It is somewhat reassuring in terms of consistency that the majority of studies have used the same, evidence-based measure to make the estimates. It is also interesting to note, however, that the studies which did not utilize ITQ demonstrated prevalence rates of CPTSD and PTSD which were much closer than those in other studies (Folke et al., 2019; Palic et al., 2016; Zerach et al., 2019). In order to ascertain the true measure of the difference in prevalence between these two disorders, a study utilizing clinician confirmed rather than probable diagnoses would be necessary.
The studies in this review were inclusive, covering populations varying from ex-POWs in a 1973 war to current-service personnel, including various conflicts, various service branches, and several different countries. Also included are those with combat and non-combat backgrounds, and in two studies, comparison is even made with civilians. That such a variety of veteran populations is included, with agreement across the majority of studies, provides some confidence in the likelihood of CPTSD being more prevalent in veterans than PTSD. It should be noted though that a number of the included studies are restricted to patients seeking treatment, with existing mental health diagnoses or who have experienced particular traumas. It is therefore difficult to extrapolate the prevalence values to the wider military and veteran populations. In regard to diversity, the majority of the studies were based on predominantly male, or all male, samples. While this reflects the gender differences in military and veteran populations, it also means caution must be exercised in generalizing results to female populations. Table 3 outlines key findings and implications as a result of this systematic review.
Implications for Practice, Policy, and Research.
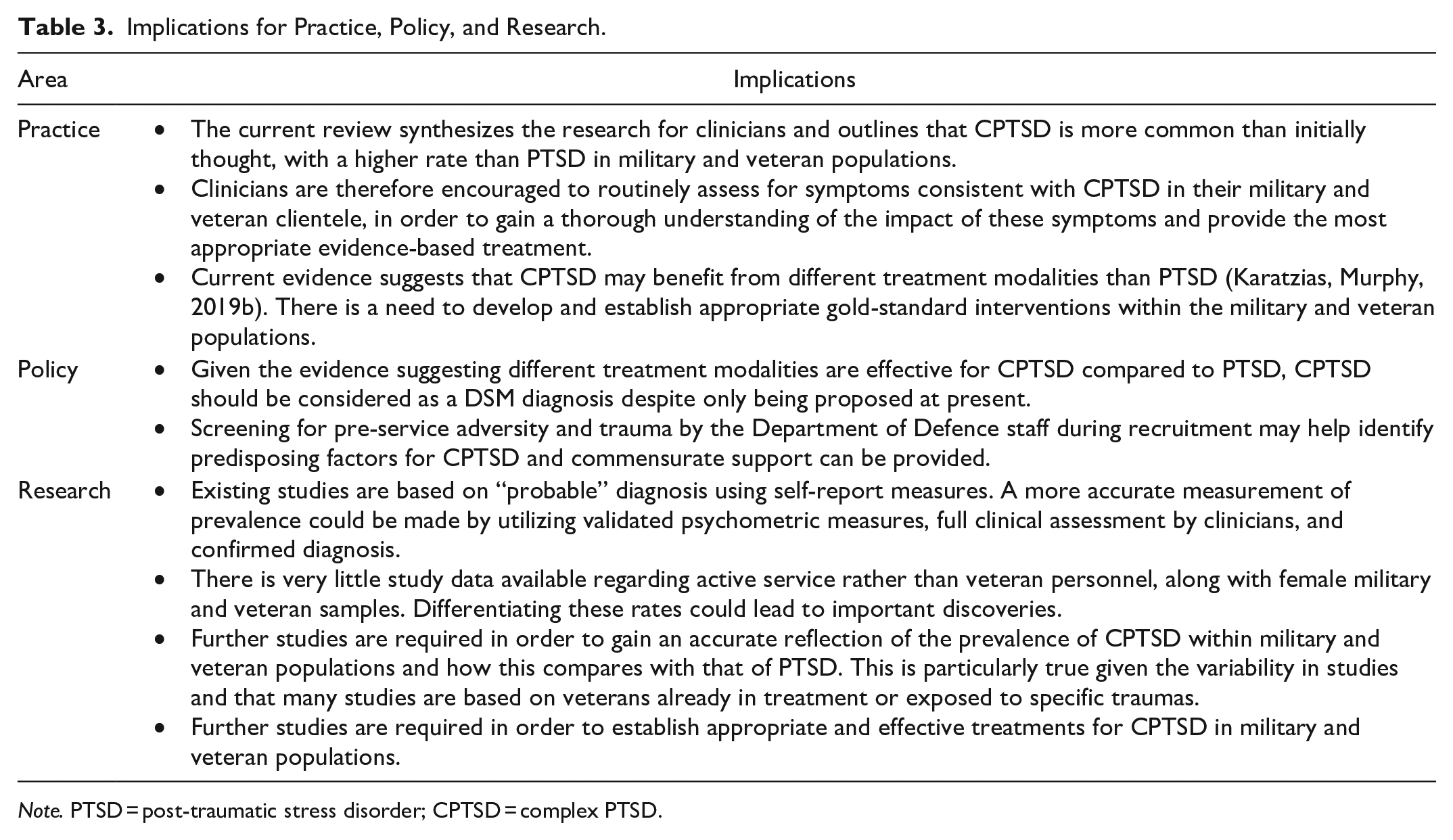
Note. PTSD = post-traumatic stress disorder; CPTSD = complex PTSD.
Limitations
A number of limitations were observed. The lack of available data regarding CPTSD in comparison to that of PTSD. PTSD is a well-established diagnosis whereas CPTSD is a new and ICD-11 only diagnosis. Prevalence studies are therefore more difficult to carry out in that significantly fewer confirmed CPTSD diagnoses have been made. An increase in the number of available studies, particularly utilizing clinician confirmed diagnoses, would improve confidence in the conclusions drawn. There is particularly limited data available regarding serving personnel with the majority of studies targeting veteran populations.
From a methodological perspective, the large variability in study population, and particularly the restricted criteria for inclusion within a number of the studies, resulted in sufficient heterogeneity that meta-analysis was inappropriate. This limited the ability to find a pooled prevalence for the existing studies. The studies included lacked clinician confirmation of diagnoses and relied on self-report measures, which are more open to bias.
Conclusion
The elevated prevalence of PTSD in the military and veteran populations compared to civilian populations is well established. However, there is significantly less data available regarding the prevalence of CPTSD in these same populations. The studies assessed in this review suggest that CPTSD may in fact be more prevalent than PTSD within the veteran population, with limited data available regarding serving personnel. Further research using medically confirmed diagnoses is required in order to make this claim with confidence. This could have particular clinical relevance due to the suggestion that different treatment modalities may be effective with CPTSD and it is suggested that clinicians consider this as a possible diagnosis during assessment and treatment.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241246996 – Supplemental material for Prevalence of Complex Post-Traumatic Stress Disorder in Serving Military and Veteran Populations: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380241246996 for Prevalence of Complex Post-Traumatic Stress Disorder in Serving Military and Veteran Populations: A Systematic Review by Rory Grinsill, Matilda Kolandaisamy, Katelyn Kerr, Tracey Varker and Andrew Khoo in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380241246996 – Supplemental material for Prevalence of Complex Post-Traumatic Stress Disorder in Serving Military and Veteran Populations: A Systematic Review
Supplemental material, sj-docx-2-tva-10.1177_15248380241246996 for Prevalence of Complex Post-Traumatic Stress Disorder in Serving Military and Veteran Populations: A Systematic Review by Rory Grinsill, Matilda Kolandaisamy, Katelyn Kerr, Tracey Varker and Andrew Khoo in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors wish to acknowledge all those who served for their country and experienced trauma as a result, as well as the clinicians and researchers that seek to help trauma recovery. The project was carried out as part of the RANZCP Fellowship requirements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.