
Abstract
Background:
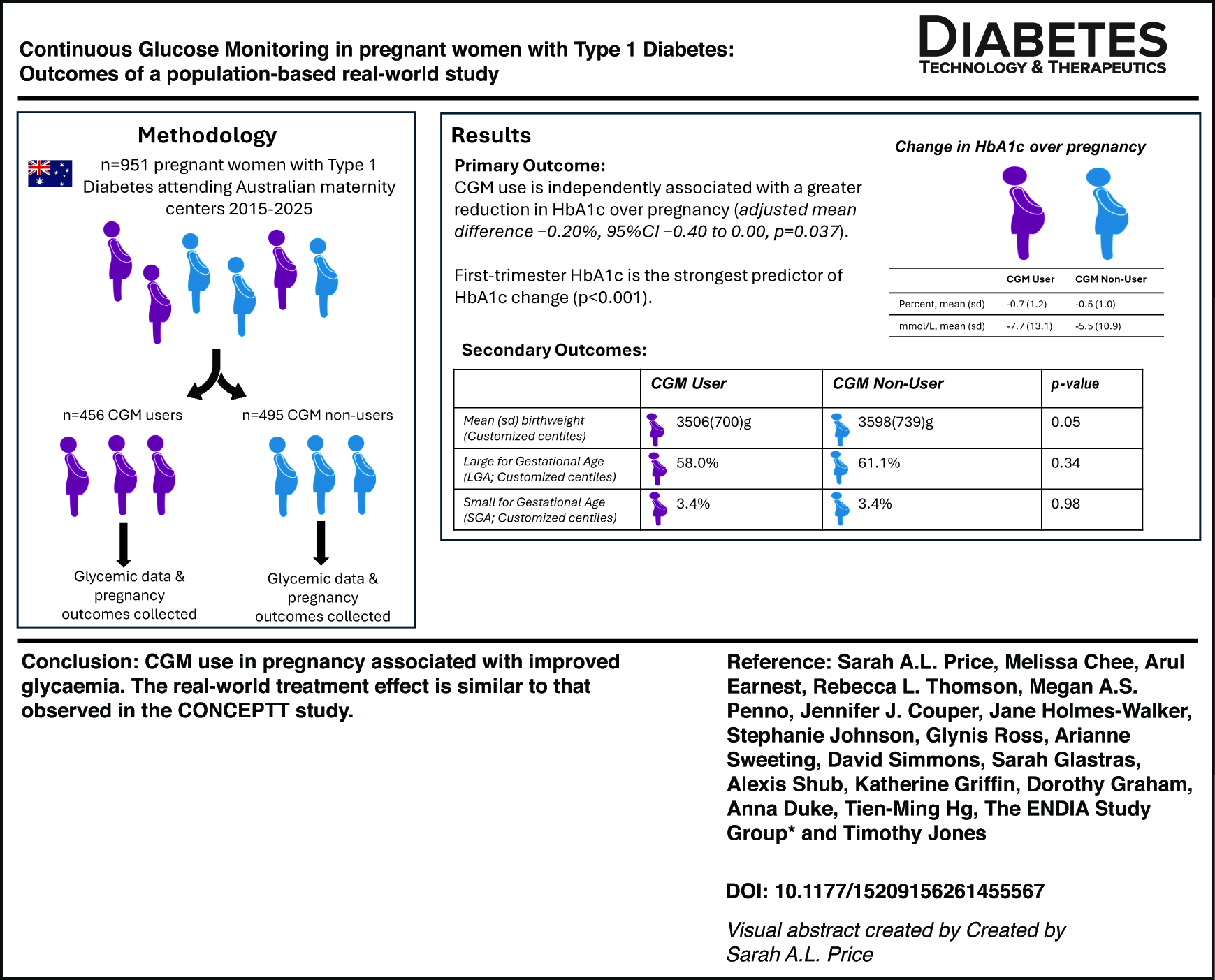
Continuous glucose monitoring (CGM) is increasingly used by women with type 1 diabetes (T1D) during pregnancy, but there are limited data on glycemic and pregnancy outcomes in large real-world cohorts.
Methods:
We collected glycemic and pregnancy outcome data from women with T1D across Australian centers between 2015 and 2025. The primary outcome was change in HbA1c from the first to the third trimester of pregnancy. Prespecified secondary outcomes included trimester-specific mean HbA1c, the proportion of women achieving HbA1c ≤6.5% (≤48 mmol/L) and ≤7.0% (≤53 mmol/L) in the third trimester, and a range of maternal and neonatal health outcomes.
Results:
Among 951 women, 456 (48%) were CGM users. Demographics and baseline characteristics were similar between CGM users and nonusers. For the primary outcome, adjusted linear regression models accounting for first-trimester HbA1c and insulin regimen demonstrated that CGM use was independently associated with a greater reduction in HbA1c over pregnancy (adjusted mean difference −0.20%, 95% confidence interval [CI] −0.40 to 0.00, P = 0.037). First-trimester HbA1c was the strongest predictor of HbA1c change (P < 0.001).
After adjustment for first-trimester HbA1c, first-trimester body mass index, insulin regimen, parity and year of delivery, CGM use was not associated with large- or small-for-gestational-age offspring and there was no significant difference between the groups in mean birthweight. Among primiparous women, CGM use was associated with lower odds of cesarean section after adjustment for confounders (adjusted odds ratio 0.22, 95% CI 0.08–0.58, P = 0.002).
Conclusions:
CGM use in pregnancy is associated with improved glycemia. The treatment effect of CGM in this real-world study is similar to that observed in the CONCEPTT study, thus supporting CGM use in pregnant women with T1D.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.