
Abstract
Objective:
Insulin requirements for people with type 1 diabetes (T1D) may vary with changes in age, pubertal status, and weight. There are limited data to assess insulin requirements based on age, sex, and body mass index (BMI) with modern treatment paradigms, especially among those using advanced technologies for the treatment and management of T1D. This study estimated total daily insulin dose (TDD) in children, adolescents, and young adults with T1D.
Materials and Methods:
This retrospective study analyzed electronic health records of people with T1D aged 2–25 years from the T1D Exchange Quality Improvement Collaborative. TDD (IU/kg/day) was reported and stratified by age, sex, BMI, glycated hemoglobin (HbA1c), and insulin delivery method.
Results:
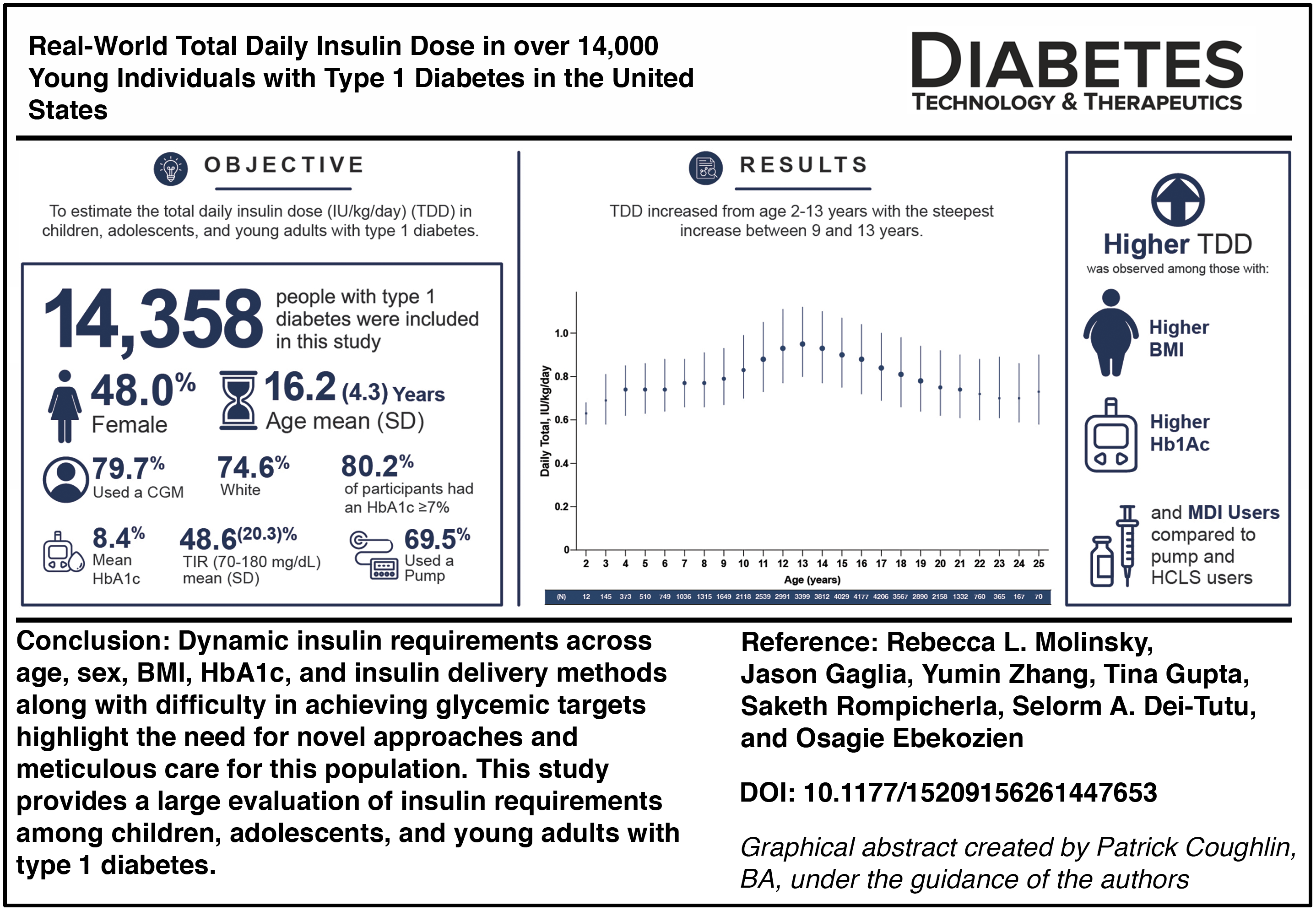
This study included 14,358 people with T1D. Mean (SD) age of 16.2 (4.3) years, 48% were females, 74.6% were White, and 80% used a continuous glucose monitor. Mean HbA1c was 8.4%, and 80.2% of participants had an HbA1c ≥7%. TDD increased from age 2–13 years, with the steepest increase from 9–13 years. In females, the peak TDD was at age 12 years compared to age 14 years for males. Higher TDD was observed among those within higher BMI and HbA1c categories and in multiple daily injections (MDI) users compared to insulin pump (non-hybrid closed loop system [HCLS]) and HCLS users.
Conclusions:
Dynamic insulin requirements across age, sex, BMI, HbA1c, and insulin delivery methods, along with difficulty in achieving glycemic targets, highlight the need for frequent reassessment of TDD, especially during puberty.
Introduction
About 2 million people in the United States live with type 1 diabetes (T1D), of which approximately 314,000 are children and adolescents. 1 Glucose monitoring is integral to the management of T1D, enabling people with T1D to achieve the American Diabetes Association/European Association for the Study of Diabetes (ADA/EASD)-recommended glycemic targets (glycated hemoglobin [HbA1c] <7%). 2 Monitoring glucose levels can prompt adjustments of insulin dosing, which can prevent the development and progression of diabetes related microvascular complications (e.g., retinopathy, nephropathy, and neuropathy). 3 In the last decade, continuous glucose monitors (CGMs) have emerged as a standard of care tool to provide real-time assessment of interstitial glucose concentrations, aiding in adjustments to insulin administration. The use of CGM among people with T1D has increased from ∼20% in 2010–2013 to ∼50% in 2016–2019. 4
Insulin requirements for people with T1D change with age, puberty, and weight.5,6 Despite an evolving treatment landscape for T1D, there have been limited studies to estimate insulin requirement in a pediatric population stratified by age, sex, body mass index (BMI), HbA1c, and insulin delivery method. Older reports predate the latest standards of care, while newer reports are often limited to a single insulin delivery method and lack granularity.7,8 Given substantial uptake in technology to treat and monitor T1D in recent decades, we conducted a contemporary study among children, adolescents, and young adults to offer insights into current insulin needs.
Materials and Methods
Study design and participants
This was a retrospective, observational study that analyzed electronic health record (EHR) data from the T1D Exchange Quality Improvement Collaborative (T1DX-QI) from 2011 to 2023. The study population included those aged 2–25 years who were diagnosed with T1D for at least 2 years and had at least one total daily insulin dose (TDD) reported. Participants were able to contribute multiple units of analysis at multiple ages. Those who were pregnant, used antihyperglycemic medication other than insulin, or used calcium channel blockers were excluded.
Study outcomes
Outcomes included estimating the TDD (IU/kg/day) in children, adolescents, and young adults with T1D at each year of age (years), across sex (male, female), BMI categories (underweight [2–20 years: <5th percentile; 21–25 years: <18.5 kg/m2], healthy weight [2–20 years: 5th to <85th percentile; 21–25 years: 18.5 to <25.0 kg/m2], overweight [2–20 years: 85th to <95th percentile; 21–25 years: 25.0 to <30.0 kg/m2], and obese [2–20 years: ≥95th percentile; 21–25 years: ≥30.0 kg/m2]); HbA1c categories (<7%, 7% to <9%, and ≥9%), and insulin delivery method (multiple daily injections [MDI], insulin pump, and hybrid closed loop system [HCLS]).
Data sources and data collection
Fifty-four endocrinology clinics in the United States contributed standardized EHR and diabetes-specific data to T1DX-QI through data use agreements. The data were combined across centers and standardized for use. All available data that met eligibility criteria were used, with the earliest records going back to 2011 and extending to 2023.
Statistical analysis
This analysis was conducted on all available data in T1DX-QI among those who met the inclusion criteria. All analyses were descriptive in nature. Categorical variables were summarized using counts and percentages. Continuous variables were summarized using the size of the subsample (n), mean, standard deviation (SD), median, and first (Q1) and third (Q3) quartiles. For TDD (IU/kg/day), the unit of analysis was the daily insulin requirement at a given year of age. Thus, individuals may contribute multiple units of analysis at multiple ages if they have eligible insulin records accrued over more than 1 year of age. TDD was summarized at each age stratified by sex (male, female), BMI categories (underweight, healthy weight, overweight, and obese), and insulin delivery modalities (MDI, insulin pump, and HCLS). Of note, MDI were reported as injections per day and was self-reported. HbA1c target of <7% for people with T1D was used as per the ADA/EASD. 8
Results
Participant characteristics
Data from 14,358 people with T1D were included in this study. The mean (SD) age was 16.2 (4.3) years, 48.0% were female, 74.5% were White, and 58.3% had private insurance. Mean (SD) diabetes duration was 7.8 (4.2) years, and 70% of participants used an insulin pump, of which 27.6% used HCLS. Mean (SD) TDD among participants was 0.86 (0.32) IU/kg/day, and those who used MDI had a mean (SD) number of 3.6 (2.0) injections per day (Table 1).
Demographics and Clinical Characteristics among Children, Adolescents, and Young Adults with Type 1 Diabetes

Ambulatory care is defined as an encounter where the patient visits the practitioner in his/her office.
BMI category defined by CDC pediatric percentiles (age 2–20: underweight: <5th; healthy: 5th–<85th; overweight: 85th–<95th; obese: 95th) and adult thresholds by kg/m2 (age 21–25: underweight: <18.5; healthy: 18.5–<25.0; overweight: 25.0–<30.0; obese: 30.0).
N = 8622 had time in range data.
The overall summary is based on the most recent encounter of each individual.
N = 2840 had the number of injections data.
BMI, body mass index; CGM, continuous glucose monitor; HbA1c, glycated hemoglobin; Q1 and Q3, first (Q1) and third (Q3) quartiles; SD, standard deviation; TIR, time in range; US, United States.
Mean (SD) HbA1c was 8.4% (2.0%) with 80.2% of the participants having HbA1c ≥7%. About 80% of the participants used a CGM and had a mean (SD) time in range (TIR) (70–180 mg/dL) of 48.6% (20.3%); 79% of the participants who used CGM did not achieve ADA/EASD-recommended TIR of >70% (Table 1). 8
Total daily insulin dose by age, stratified by sex and BMI
Median TDD increased starting from age 2 (0.63 IU/kg/day) to 13 years (0.95 IU/kg/day) and then stabilized around 0.70 IU/kg/day with the steepest increase occurring between age 9 (0.79 IU/kg/day) and 13 years (0.95 IU/kg/day; Fig. 1a). Specifically for females, median TDD peaked at 12 years (0.98 IU/kg/day) and, for males at 14 years (0.96 IU/kg/day). Overall, TDD was higher in females until age 13 years, but thereafter, males reported a higher TDD (Fig. 1b). In addition, those in a higher BMI category (i.e., overweight or obese) had higher median TDD than those in a lower BMI category (i.e., underweight or healthy weight) (Fig. 1c); however, this trend was nominal. This relationship stayed constant even after stratifying by sex with an increase in TDD being more pronounced at age 14/15 years among males and at age 12/13 years among females (Fig. 2). Also refer to Supplementary Table S1 (mean, median [Q1, Q3], minimum, and maximum TDD) and Supplementary Table S2 for n (%) by dose range category (IU/kg) corresponding to Figure 1a–c.

Median total daily insulin dose (TDD; IU/kg/day) by age, sex, and body mass index (BMI) category.
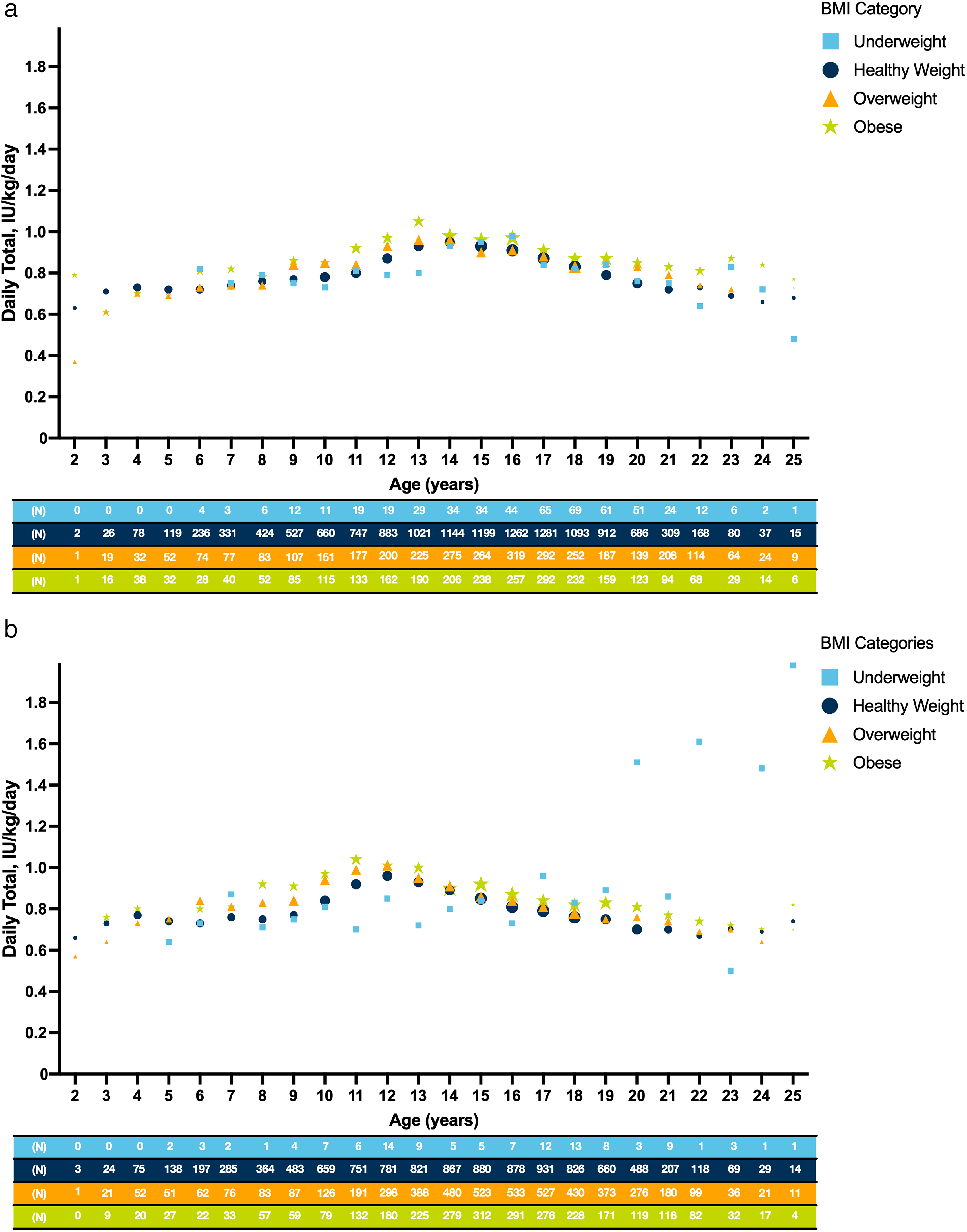
Median total daily insulin dose (TDD; IU/kg/day) by age, sex, and body mass index (BMI) category.
Total daily insulin dose by age and HbA1c stratified by sex
Total daily insulin dose (TDD) by age and HbA1c category (<7%, 7% to <9%, ≥9%) is presented in Figure 3a. Starting from age 7 years, people with T1D with HbA1c <7% generally had a lower median TDD than those with higher HbA1c (7% to <9% or ≥9%). TDD peaked for females at 12 years across all HbA1c categories, while for males, it peaked at 15 years of age among those with an HbA1c <7%, 14 years of age among those with an HbA1c 7% to <9%, and at 13/14 years of age among those with an HbA1c of ≥9% (Fig. 3b and c).
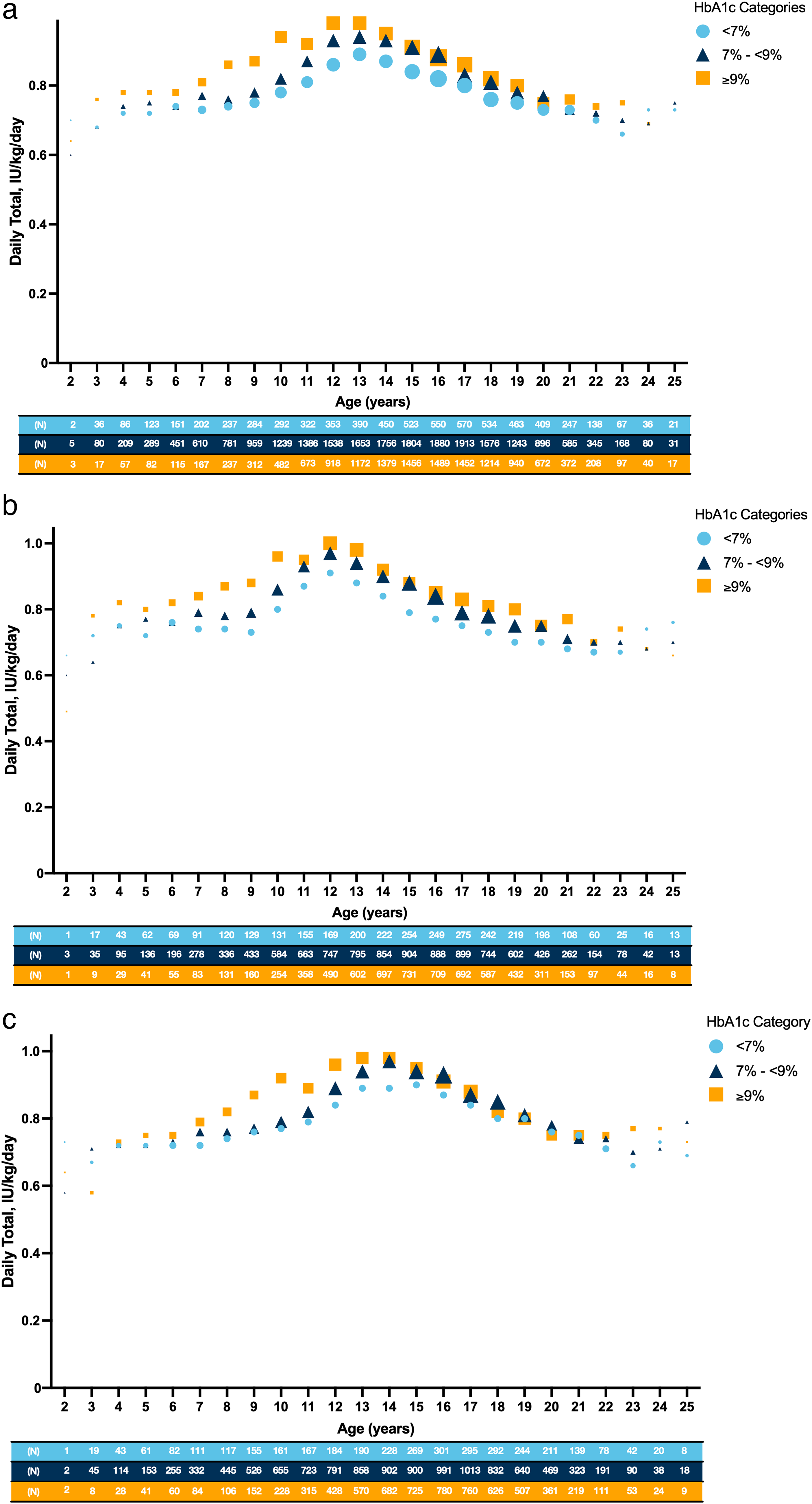
Median total daily insulin dose (TDD; IU/kg/day) by age and HbA1c, glycated hemoglobin (HbA1c) category.
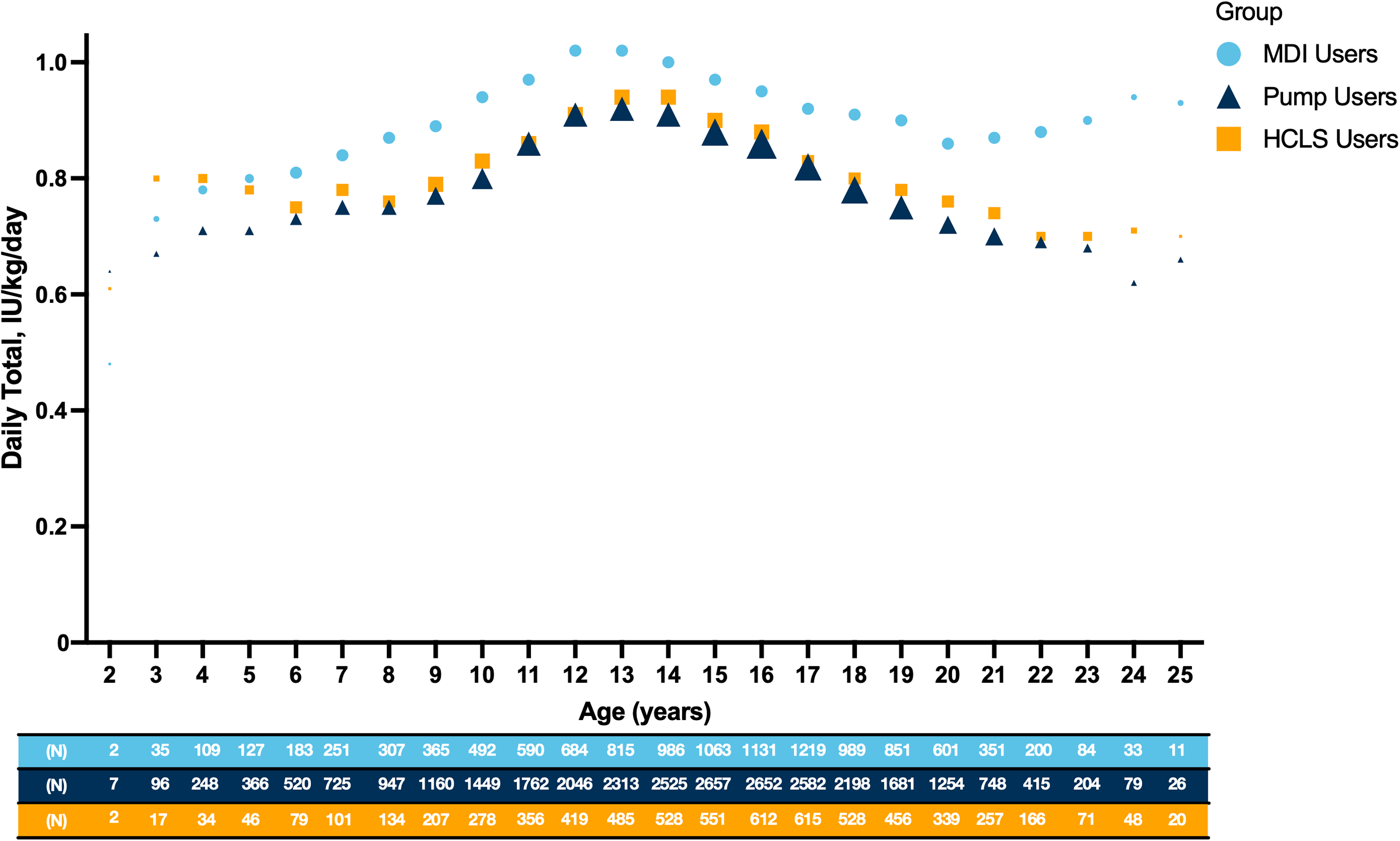
Median total daily insulin dose (TDD; IU/kg/day) by age and method of insulin delivery. This figure illustrates the distribution of TDD in IU/kg/day at each year of age by insulin delivery method (multiple daily injections [MDI], insulin pump, and hybrid closed loop system [HCLS]) from 2 to 25 years. Each data point represents the median IU/kg/day for the respective age group, with the symbol size being proportional to the sample size. The rows at the bottom of the figure indicate the total number of people contributing data at each age (N). Refer to Supplementary Table S1 for the mean, median (first [Q1], third [Q3] quartiles), minimum, and maximum total daily insulin dose corresponding to Figure 4.
Total daily insulin dose by age and method of insulin delivery
TDD by age and method of insulin delivery (MDI, insulin pump, and HCLS) is summarized in Figure 4. Starting at 5 years of age, MDI users had a higher median TDD compared to insulin pump (excluding HCLS) and HCLS users. Also refer to Supplementary Table S1 for mean, median (Q1, Q3), minimum, and maximum TDD corresponding to Figure 4.
Discussion
This study evaluated TDD across age, sex, BMI, HbA1c, and insulin delivery methods in people with T1D during childhood, adolescence, and young adulthood. A total of 14,358 participants were included, the majority of whom were male, White, and covered by private health insurance. Technology use was high, with 70% using an insulin pump and 80% utilizing CGM. However, despite the use of CGM, 79% of users with data available did not achieve the ADA/EASD-recommended TIR of >70%. 8 Few studies have explored TDD trends in pediatric populations, yet understanding these trends is critical given the hormonal, growth, and weight changes that influence insulin needs during these developmental stages.
Differences in TDD were observed across age, sex, and BMI. Consistent with prior reports,9,10 a steady increase in TDD was seen until ages 12–14 years, with the steepest increases occurring between ages 9–13 years. A similar pattern was seen after stratifying by sex, with females reporting their highest TDD at around 12 years, while males reported their highest TDD at around 14 years. Insulin requirements increase at the onset of puberty, during growth spurts, and with an increase in BMI as a result of insulin resistance mediated in part by increased growth hormone secretion.11,12 A cross-sectional study assessing insulin resistance in children reported an increase in insulin resistance in girls from ages 5–13 years and boys from ages 5–14 years. 13 This rise in insulin requirement coincides with insulin resistance owing to hormonal and developmental changes during puberty. 14 In our study, TDD was higher in females until 13 years of age; after which, males had higher TDD, which may be attributed to differences in pubertal timing, consistent with the literature. 6 We also observed that overall, those with a higher BMI tended to have a higher TDD compared to those of a healthy weight. However, fluctuations were seen among those who were underweight, which was most likely owing to the small sample size, especially among those aged 2–8 and 23–25 years, where <10 people contributed data. Our study population had a similar BMI distribution to children and adolescents aged 2–19 years in the general United States population, with 16.6% being overweight and 18.5% being obese. 15 Although dynamic increases in insulin resistance related to increasing weight may be driving the observed increase in TDD in this study, this complex interrelationship of BMI and insulin use is not completely understood.
Our results are consistent with the pattern of rising HbA1c observed in a previous study carried out by the T1D Exchange registry, which found that average HbA1c increased through childhood, peaking in adolescence and early adulthood, and then decreased and remained reasonably stable through the rest of adulthood. 16 It has been shown that glycemic control declines during adolescence with higher HbA1c concentrations than at any other time period in the lifespan of people with T1D. 17 In a recent retrospective study of young children using HCLS, achieving target HbA1c was a challenge, and the management of diabetes in young children was found to be complicated by higher variability in insulin requirements.18,19 In our study, TDD was generally lower in people with HbA1c <7% than in those with a higher HbA1c, and these results did not differ by sex. Although 80% of the people in our study were using CGM, roughly 79% did not achieve the target TIR of >70%, indicating suboptimal glycemic control. These findings help illustrate the challenge in achieving glucose targets, particularly in a population with multiple factors affecting insulin needs.
In addition, MDI users had consistently higher median TDD compared to insulin pump and HCLS users. Similar findings were observed in a German study among children and adolescents that reported insulin use on pump therapy was about 10 units lower than insulin use among MDI users after adjusting for age, sex, insulin pump use, and insulin formulation. 20 Prior research has demonstrated that individuals switching from MDI to an insulin pump experienced a 10%–20% decrease in TDD due to pharmacokinetic differences between the modalities. 21
Accurate assessment of insulin use in clinical settings is largely dependent on the assumption that people with T1D are dosing insulin as prescribed by their physician. However, previous research showed that there is often a gap between the dose on the prescription and the actual amount of insulin used. 22 Thus, it is important for physicians to confirm the actual insulin dose prior to adjusting a patient’s insulin dosage. Failure to confirm the actual insulin dose can be dangerous, as an individual may receive a prescription for a regimen that is higher than what the patient is administering, thus raising the risk for hypoglycemia. Beyond assessing for changing insulin needs in the setting of factors such as weight gain, puberty, and insulin delivery method, providers should also consider other elements that could impact the ability to reach glucose targets, including suboptimal HCLS/pump settings, mismatch of insulin to carbohydrate estimation, and diabetes burnout.
This study was designed as a retrospective study and has some limitations. The first is that this analysis, presented by age, sex, and BMI, summarizes population-level trends in the absence of documentation of individual subjects’ pubertal timing. In addition, most centers included in the T1DX-QI were academic-based diabetes practices, and individuals who are followed in academic centers may have more access to resources and multi-disciplinary care. In addition, since this study relied on EHR data, which comes directly from the participating centers, variability in data fields, collection of variables, and definitions (e.g., pump and CGM naming conventions) exists. Analyses were also constrained by missing data. Specifically, pump information, whether participants were on open loop, hybrid closed loop, or predictive low glucose suspend, was missing for 61.9% of people with T1D using pumps. Also, as mentioned above, limited data were available for some stratifications, like males who were underweight, especially at the tails of the age ranges. Although this study took place between 2011 and 2023, and HCLS were not commercially available until September 2016, we were still able to include data from 2,753 (27.6%) HCLS users. Specifically, recent advances in T1D technology including fully automated insulin delivery (AID) systems, which automatically adjust all insulin delivery, should be explored in future analyses as they may help pediatric individuals achieve clinical targets safely despite dynamic insulin requirements. To capture TDD among those using MDI, injections per day were self-reported. Self-reported data is subject to recall bias, and it is important to note that this data is not as objective as insulin data collected by pump users. However, the use of connected insulin pens, though likely small and difficult to capture in these data, has the capability to objectively track insulin doses, making the data they provide more reliable.
Since analyses were performed in combinations of BMI, HbA1c, and insulin delivery method, at each age, missing data led to smaller sample sizes. Furthermore, the groups of individuals who contributed insulin data to different age levels may not be the same; thus, no formal comparisons of insulin requirement between the same participants at different age levels can be made. Lastly, specific markers of puberty were not systematically captured in the data.
Conclusion
This study evaluated insulin requirements among children, adolescents, and young adults with T1D, highlighting the significant variability in insulin needs across age, sex, BMI, and insulin delivery methods. Despite high technology use (70% using pump; 80% using CGM), approximately 80% had an HbA1c ≥7%, underscoring the challenges in achieving optimal glycemic control even with advanced tools. Our findings emphasize the importance of frequent reassessment of TDD, particularly during periods of growth, puberty, weight change, or transition across insulin delivery methods. Individualized dosing informed by a thorough review of pump usage and glucose data, rather than relying solely on prescription records, is essential to ensure optimal care. This large-scale evaluation of insulin requirements among children, adolescents, and young adults with T1D underscores the dynamic nature of insulin requirements in pediatric T1D populations and the need for innovative strategies to help people with T1D achieve glycemic targets safely. Advances in automated diabetes technologies provide significant potential for enhancing clinical outcomes among pediatric individuals with T1D. However, proactive and structured discussions between clinicians and people with T1D about insulin regimens and other facets of the treatment plan remain critical to addressing the evolving needs of this population.
Authors’ Contributions
R.L.M. was involved in the study design, data interpretation, and drafting of the article. J.G. contributed to the study design, analysis, and T1D knowledge and expertise. Y.Z. was responsible for data analysis and interpretation. S.R. contributed to the acquisition of the data, design of the study, analysis, and T1D knowledge and expertise. T.G. contributed to the study design and clinical interpretation of the data. S.A.D.-T. provided critical interpretation, reviewed the output, and contributed to T1D pediatric knowledge and expertise. O.E. contributed to the acquisition of data, design of the study, and analysis, as well as contributed to T1D knowledge and expertise. All the authors approved the final version of the article.
Footnotes
Acknowledgments
The authors are extremely grateful to all the participants with T1D and their families who took part in this study. The authors would like to thank Susan Thapa (T1D Exchange) for her significant role in data analysis; Justin A. Indyk (Nationwide Children’s Hospital, Columbus, OH), Janine Sanchez (University of Miami Miller School of Medicine), Allison Mekhoubad (Northwell Cohen Children’s Medical Center, Queens, NY), and Meredith Wilkes (Icahn School of Medicine at Mt. Sinai, New York, NY) for insights, expertise, and experience as pediatric endocrinologists. Medical writing support was provided by Shivali Arora, PhD, Molly Opferman, MS, and graphical support was provided by Patrick Coughlin, BA, who are employees of Vertex Pharmaceuticals, under the guidance of the authors.
Author Disclosure Statement
R.L.M., Y.Z., and T.G. are employees of Vertex Pharmaceuticals and may own stock/stock options in the company. J.G. has received institutional grants from Sanofi, Biomea Fusion, Diamyd Medical, and Dompé farmaceutici, consulting fees from Vertex Pharmaceuticals, Ascensia, AstraZeneca, Kriya Therapeutics, and Diamyd Medical. J.G. also owns stocks of Vertex Pharmaceuticals. S.R. and O.E. have received medical writing support for the current article from Vertex Pharmaceuticals. S.A.D-T. received medical writing support for the current article from Vertex Pharmaceuticals and is a co-lead of the T1D Exchange QI collaborative HEAL committee.
Funding Information
This study was supported by Vertex Pharmaceuticals.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.