
Abstract
This original study investigated the impact of language on stigmatizing attitudes towards people in forensic mental health services. We recruited a nationally representative UK adult general population sample (N = 668) and used a randomized online survey design with three experimental conditions. We explored the associations between different terms—“mentally disordered offender”, “forensic mental health patient”, and “person working towards recovery using forensic mental health services”—and attitudes related to social distance, perceptions of community risk, stereotypes, compassion, and diminished responsibility. Our results showed that person-first, recovery-oriented language was associated with reduced desire for social distance and increased perceptions of responsibility for behavior. These findings make a significant contribution to knowledge, adding new data to demonstrate that person-first, recovery-oriented language is linked to attitudes toward stigmatized groups. This research supports the Lancet Commission's call for the use of person-first language. Further, our findings provide a valuable guide, shaping the direction of future research relating to the effects of language on stigma, real-world behaviors, and interventions designed to reduce stigma towards people in forensic mental health systems.
Plain language summary
This study looked at how the words we use affect public attitudes toward people who use forensic mental health services (such as those involved in the criminal justice system and receiving mental health care). We asked a representative group of UK adults to respond to descriptions using different terms—like “mentally disordered offender” or more positive phrases like “person working towards recovery using forensic mental health services.” We found that when person-first language was used, people felt more compassionate, saw these individuals as more responsible for their actions, and were more willing to accept them in society. The findings support the idea that using person-centred language can help reduce stigma and improve public attitudes.
Introduction
In 2022, a Lancet Commission called for the eradication of stigma towards people with mental health conditions (Thornicroft et al., 2022). Stigma leads to a range of negative social, interpersonal, and health-related outcomes. It refers to a “deeply discrediting” attribute that reduces a person “from a whole and usual person to a tainted, discounted one” (Goffman, 1963). Stigma is contingent on social power dynamics; it involves the appraisal of certain characteristics, typically held by people with less social power, as negative by groups in positions of power. According to Link and Phelan (2001) this power-contingent social process plays out over several phases. A personal- or group-level trait is identified and labeled (e.g. mental illness, criminal record, disability); behaviors and qualities are ascribed to this trait, stereotyping those with the trait; and individuals are separated physically, linguistically and symbolically as “others” and excluded from full social citizenship. This leads to status loss, dehumanization, and discrimination across a range of life domains (e.g. accommodation, employment, relationships).
People in forensic mental health services have multiple stigmatized traits. They have been described as carrying triple stigma as mentally ill, substance abusing, and criminal (Mezey et al., 2016). To these could be added stigma relating to ethnicity, socioeconomic status, educational attainment, and neurodivergence. Some people report stigma being worse than their stigmatized condition e.g. mental health diagnosis (Thornicroft et al., 2022). It can affect people in forensic services at the individual level through self-stigmatization, reduced quality of life, hindered service use, and increased stress and self-harm (Corrigan et al., 2005; Moran, 2012; West et al., 2018). Health and social care can suffer through worsened health outcomes, prolonged conditions, and low public investment in mental health (Link & Phelan, 2006). Structurally, it impacts education, employment, family life, housing, legal and human rights, and policy participation—in other words: social citizenship (Thornicroft et al., 2022).
The Lancet Commission specifically addressed the role of language use in reducing stigma. It called for person-first language, the roots of which can be traced to the disability rights movement of the 1970s (Jensen et al., 2013). Person-first language is “a form of linguistic expression relying on words that reflect awareness, a sense of dignity, and positive attitudes about people with disabilities” (cited in Jensen et al., 2013, pp. 146–147). It aims to promote empowerment, agency, and citizenship of all people. The language used to describe people with mental health conditions can discursively promote and maintain their place in a social hierarchy, reflecting the power dynamics involved in the stigmatization process referred to previously.
There has been a proliferation of guidance, training, and calls for the use of person-first language. This has been issued by, amongst others, Everymind, Australia; the National Institute on Drug Abuse and the Centres for Disease Control, USA; Mind, UK; See Change, Ireland; and the Mental Health Commission of Canada. It is important, however, to note that person-first language is not the preferred linguistic choice for all advocacy and support groups. In 1993, the National Federation of the Blind, USA, issued a statement opposing person-first language (Bickford, 2004). They argued that the term “blind person” demonstrates respect for blind individuals without minimizing the condition or denying the reality of the disability. Research has found that autistic people who identify strongly with their diagnosis preferred identity-first language over person-first (e.g. “autistic person”) (Bury et al., 2022). Some argue that person-first language emphasizes negative perceptions of disability instead of embracing these conditions and that it is more commonly applied to people with disabilities than to those without, further reifying difference (e.g. doctor vs person who practices medicine; Dwyer, 2022; Gernsbacher, 2017).
Several studies have explored whether the use of person-first language is associated with or influences attitudes and behaviors. This work spans criminal justice involvement, mental illness, substance abuse and disabilities. Most were experimental, using randomized survey designs; some included vignettes to replicate real-life situations (Ashford et al., 2018; Goodyear et al., 2018; Martinelli et al., 2020). Overall, findings demonstrated a positive influence of person-first language on attitudes and perceptions. Kelly and Westerhoff (2010) found that terms such as “person with a substance use disorder” elicited more favorable attitudes than terms such as “addict.” Their findings suggested that person-first expressions encourage viewing substance use as a condition rather than “a moral failing.” Granello and Gibbs (2016) reported that terms such as “the mentally ill” were associated with reduced levels of tolerance when compared to the phrase “people with mental illness.” Several studies have found that person-first language is associated with greater support for treatment and rehabilitation programs, and less support for punitive and restrictive policies, and endorsement of fewer negative stereotypes (Harris & Socia, 2016; Jackl, 2023; Kelly et al., 2010; Lowe & Willis, 2022).
However, other studies did not find significant differences in attitudes by language condition or that differences are attributable to demographic and professional characteristics (Bernoski, 2023; Boland, 2022; Williams et al., 2022). A randomized survey by Granello and Gibbs (2016) distributed to three groups—undergraduate students, adult community members, and counselors—found that the use of person-first language to describe mental illness was associated with less restrictive and authoritarian attitudes but was not linked to benevolent attitudes and levels of support for community-based care among undergraduate students and counselors. By contrast, in the adult community sample, the use of person-first language was positively associated with support for community-based care, but no significant effects were found for restrictive and authoritarian attitudes. Denver et al. (2017) reported that the perceived risk of reoffending depends on the type of previously committed offence, and person-first language was demonstrated to lower reoffending expectations when used to describe people who had committed violent offences but not non-violent offences.
To our knowledge, no study has been conducted exploring the impact that person-first language has on attitudes towards people in forensic mental health services. This study is the first to fill this gap by testing whether the terms “mentally disordered offender,” “forensic mental health patient” or “person working towards recovery using forensic mental health services” were associated with differences in a UK, general population sample's desire for social distance, negative stereotyping, support for rehabilitation and compassion, perceptions of community risk and diminished responsibility. To the extent that the language used in clinical settings (e.g. hospital records) and everyday conversation can impact the quality of care and social inclusion policies, it is important to measure its effect in shaping attitudes and perceptions towards individuals with mental health problems or criminal justice system involvement.
Research Question
To what extent is person-first, recovery-oriented language associated with a desire for social distance and attitudes towards people in forensic mental health services in a U.K. general public sample when controlling for covariates?
Hypotheses
There will be significant differences in scores across the three language conditions on perceptions of: community risk, diminished responsibility, rehabilitation and compassion, negative stereotypes, and desire for social distance when controlling for covariates.
Participants in the person-first, recovery-oriented language condition will report more positive/supportive attitudes than the other two language conditions when controlling for covariates.
Participants in the forensic mental health language condition will report more positive/supportive attitudes than the mentally disordered offender condition, when controlling for covariates.
The control variables in our hypotheses include: age, gender, ethnicity, personal experience with mental illness, personal criminal conviction, personal or family experience of victimization in the past 5 years, quality of interactions with people with mental illness, hostility towards ethnic minorities, and quality of interactions with people with criminal justice involvement.
Methods
Study Design
A cross-sectional, randomized online survey methodology was used to recruit a nationally representative sample of the UK adult population. Data were collected over one week in April 2024. The American Psychological Association (APA) Journal Article Reporting Standards (JARS) Quant reporting guidelines are used to describe the study (Appelbaum et al., 2018).
Data Collection
Recruitment
The online research participation website “Prolific” was used to recruit participants. Participants were existing members of the Prolific platform who were anonymous to the researchers. The study was advertised on Prolific and participants who expressed an interest were taken to an information sheet and consent page. All participants were 18+. The study remained open until a representative sample of the UK population was recruited. According to Prolific, a representative sample is one that matches the UK population on the variables age, gender, and ethnicity, using the most recent data published by the UK Office of National Statistics. Participants were randomly allocated to one of the three language condition surveys hosted on “Jisc Online Surveys” via the website URL randomizer “Nimble Links.” Participants were not aware of experimental manipulations, all researchers were aware. They were paid £1.50 for their participation. Using G*Power's a priori “ANCOVA: Fixed effects, main effects and interactions” test, with a error probability = .05, f = 0.25, power = 0.8, numerator df = 2, number of groups = 3, and nine covariates, a minimum sample size of n = 158 was suggested.
Screener Question
Studies have found that various factors affect respondents’ answers to online surveys, including time and day of completion, age, and degree of attention (Sauermann & Roach, 2013). To mitigate the risk that respondents did not pay close attention to questions in the survey, we included a screener question (Berinsky et al., 2014). This question asked participants to select an answer according to their preference but then instructs respondents, in an accompanying text explanation, to ignore this instruction and select specific answers.. However, research has found that excluding screener failures can introduce systematic bias relating to demographic factors (Berinsky et al., 2014). Therefore, we conducted a primary analysis on respondents who passed the screener and a secondary analysis on everyone who participated, i.e. those passing and failing the screener. We considered the results found in both analyses more robust.
Demographic, Covariate, and Background Variables
Prolific collects and provides the following data: age, gender, ethnicity, first language, current country of residence, nationality, country of birth, student status, and employment status. All participants stated they spoke English fluently.
Personal experience of mental illness was measured with a single yes/no question: “Have you ever had personal experiences with mental health problems that significantly affected your ability to live your life the way you wanted to?”
Personal criminal conviction was measured with a single yes/no question: “Have you personally been convicted of a criminal offence?”
Experience of victimization was measured via the question: “Have you or a person in your family been a victim of crime in the previous 5 years?”
Questionnaires
Quality of interactions with people who have criminal justice system involvement and quality of interactions with people who have experience of mental illness (adapted from Jackl, 2023). Higher scores represent better quality interactions. Two variables were calculated that summed respondents’ scores on 4-point Likert items which asked how frequently (“Never” to “Most of the time”) respondents’ interactions have been “Friendly,” “Pleasant,” “Cooperative or supportive,” “Voluntary” and “As persons of equal status.”
Social distance (adapted from Jackl, 2023). A higher score indicates greater desire for social distance. A variable was calculated that sums respondents’ scores on five 5-point Likert items (“Very willing” to “Very unwilling”) which ask about respondents’ willingness live next door to, spend an evening socializing with, being friends with, and working together with people in the criminal justice system who receive treatment for mental health needs or for someone in this population to marry into their family.
Attitudes towards mentally ill offenders (ATMIO; Brannen et al., 2004). This has 23 6-point Likert scale items (from “Disagree strongly” to “Agree strongly”). It is used to measure attitudes towards criminal justice-involved individuals with mental health conditions. The scale assesses four attitudinal domains: “negative stereotypes” (10 items, e.g. “If you give a mentally ill offender an inch, he or she will want to take a mile”); “rehabilitation/compassion” (five items, e.g. “Mentally ill offenders need affection and praise just like anybody else”); “community risk” (five items, e.g. “If a mentally ill offender does well in prison, he or she should be let out on a parole”); and “diminished responsibility” (three items, e.g. “Mentally ill offenders are not completely responsible for their crimes”). Scores on each domain and the total scale are summed. Higher scores indicate more positive/less stigmatizing attitudes. Past studies have demonstrated good psychometric properties with evidence of internal reliability and convergent validity: Cronbach's α coefficients ranging from .73 (Brannen et al., 2004) to .88 (Church et al., 2009); though the internal reliability of the “diminished responsibility” domain has been found to be weak-moderate and below the customary .7 threshold (Tremlin & Beazley, 2024; Weaver et al., 2019).
Hostility towards racial minorities. This was measured via the question: “Would you mind or not mind if one of your close relatives were to marry a person of black or West Indian/Asian origin?” with the response options: “Would mind,” “Would not mind”, “Not sure” and “Prefer not to say” (adapted from Ford, 2008).
Language Conditions
Three language conditions were tested in this survey: “mentally disordered offender”, “forensic mental health patient”, and “person working towards recovery using forensic mental services”. All three language condition surveys had the same questions and definition of the population. The only manipulation was the term used to describe the population. A definition of the randomized term was presented to participants and then this term was embedded into the stem of the questions measuring social distance and the ATMIO questionnaire.
The definition presented to participants was: “The term "_______” is used in this study. This term refers to someone in the criminal justice system who is receiving treatment for mental health needs. This might include treatment offered in police custody, prison, psychiatric hospitals, approved premises, or in community out-patient settings.”
The choice of these three terms was influenced by past research, knowledge of routine practice, and a patient and public involvement and engagement (PPIE) session held in January 2024 with five people who were using forensic mental health services as in- or out-patients and one carer. Participants in this PPIE session found “offender” to be the most stigmatizing term, while “mental” was also considered stigmatizing. They emphasized the importance of putting the person-first, noting that any label can be detrimental and individuals should have the autonomy to choose how they are referred to. They felt person-first language is preferred by patients, labels should not focus on past actions and should focus on current actions (hence our use of recovery-oriented language). “Mentally disordered offender” is prevalent in the academic literature and reports from bodies like His Majesty's Prison and Probation Service (2022) and the Care Quality Commission (2022) and “forensic mental health patient” is used often by researchers and clinicians. Therefore, these terms were chosen as comparators. While recognizing the disadvantages of generalizing labels, there is value in exploring the attitudes associated with different terms used by staff, patients, and the public.
Data Analysis
Missing data was recorded for 0.91% of questionnaire item responses (i.e. ATMIO, social distance, quality of interactions with others), and 4.6% of background questions (i.e. age, gender, ethnicity, education, work, personal experience with mental illness and criminal justice involvement, victimization) for the total data set (N = 668).
Thirteen items on the ATMIO were reverse coded (Brannen et al., 2004). Sum scores were calculated for the total ATMIO and its domains, and the social distance and quality of interactions questions. To ensure there were enough observations per group in the independent variables in the ANCOVAs, the following categorical variables were recoded into dichotomous variables: ethnicity (White; Asian, Black, Mixed, Other) and employment (Full-time, and Part-time; Not in paid work, Unemployed and job seeking, and Due to start work in next month). All demographic data before and after recoding are presented in Table 1. “Don’t know” response options were recoded into missing data for the ANCOVAs.
Overview of Participant Background and Demographic Data, N = 668.
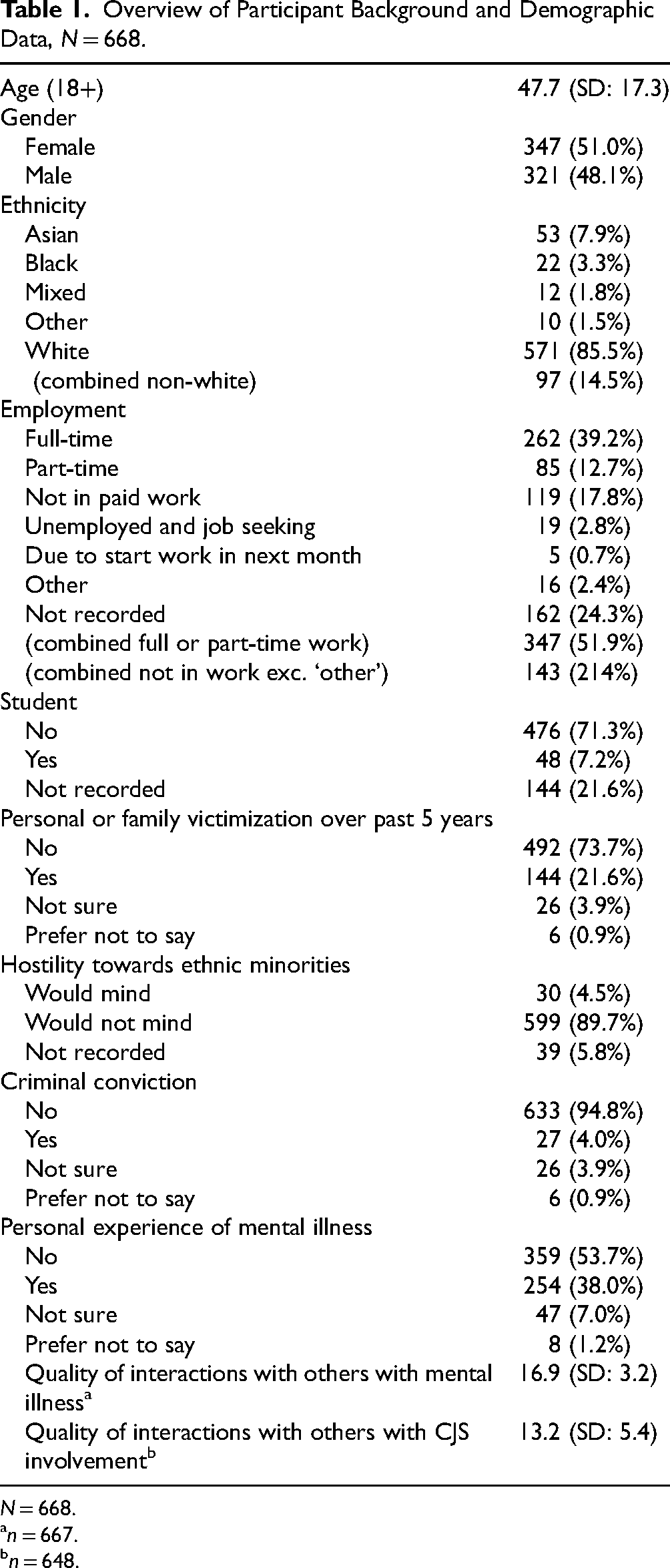
N = 668.
n = 667.
n = 648.
Background and demographic data are summarized descriptively. T-tests and chi-square analyses were conducted to explore whether there were significant differences between respondents who passed and those who failed the screener question. ANOVAs were conducted to compare participants in the three language conditions on demographic variables prior to testing hypotheses. Cronbach's α was calculated to investigate the internal reliability of the ATMIO, its domains, and the social distance summed score (Table 2).
Overview of Mean Sum Scores, SDs, and Cronbach’s α Scores for ATMIO and Social Distance Outcome Measures.
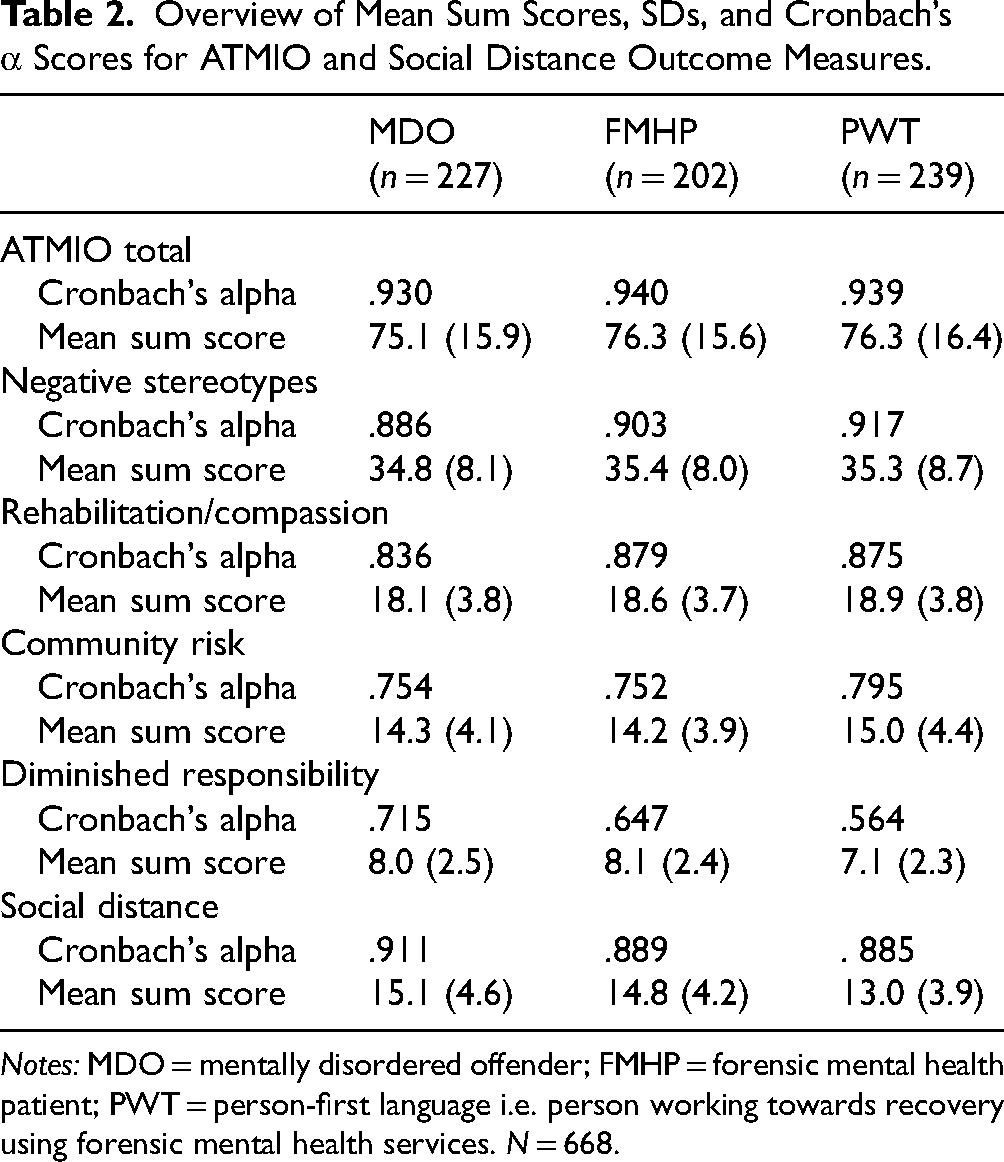
Notes: MDO = mentally disordered offender; FMHP = forensic mental health patient; PWT = person-first language i.e. person working towards recovery using forensic mental health services. N = 668.
Five bootstrapped ANCOVAs using SPSS's Bootstrapping with 1000 samples function were conducted to examine the impact of language condition (predictor variable) social distance and ATMIO domains (outcome variables), controlling for covariates. Bootstrapping was chosen as this offers a more robust analysis but also helped account for non-normality in the data (Field, 2024), which was observed on several outcome variables.
Partial eta squared (η2) effect sizes are reported; η2 = .01 indicates a small effect, η2 = .06 indicates a medium effect, and η2 = .14 indicates a large effect. Post-hoc comparisons were conducted using the Bonferroni correction to identify significant differences between language conditions. Bootstrapped 95% Confidence Intervals are reported for mean outcome scores. The same procedure was undertaken for the primary and secondary analyses (i.e. attention screener passers only and the whole sample respectively).
Ethical Approval
Ethical approval for the study was granted by the University of Greenwich's University Research Ethics Board. The study was conducted in line with the Helsinki Declaration of 1964.
Results
Median completion time was 8 min 41 sec, similar to piloting by the research team. A total of N = 668 completed the survey; n = 196 (29%) failed the screener question leaving n = 472 for the primary analysis. Respondents passing the screener were significantly more likely to be older (p < .001; d = .346) and to have been a victim of crime in the past 5 years or a member of their family to have been a victim of crime over the same period (p = .003; OR = 1.48). They were significantly less likely to be male (p < .001; OR = .53), unemployed (p = .008; OR = .53), and a student (p = .002; OR = .5). No significant differences between language conditions were found for age, gender, ethnicity, student status, victimization, or employment status. The mean sum total scores, standard deviations, and Cronbach's α for the ATMIO total scale and domains, social distance, and quality of interactions scores are shown in Table 2.
Primary Analysis of Respondents Passing the Attention Screener Question
Table 3 shows the results of the five ANCOVAs, including adj-R2 scores, F-scores, p-values, and effect sizes for each independent variable. When controlling for the specified covariates (e.g. age and gender etc.), significant differences by language condition were observed for desire for social distance (p < .001; η2 = 0.067), and perceptions of community risk (p = .006; η2 = 0.028) and diminished responsibility (p = .007; η2 = 0.027). No significant differences by language condition were observed for negative stereotypes or rehabilitation/compassion.
ANCOVA Results with Language Condition and Personal Factors as Predictor Variables and Attitudes as Outcome Variables for Primary and Secondary Analysis.
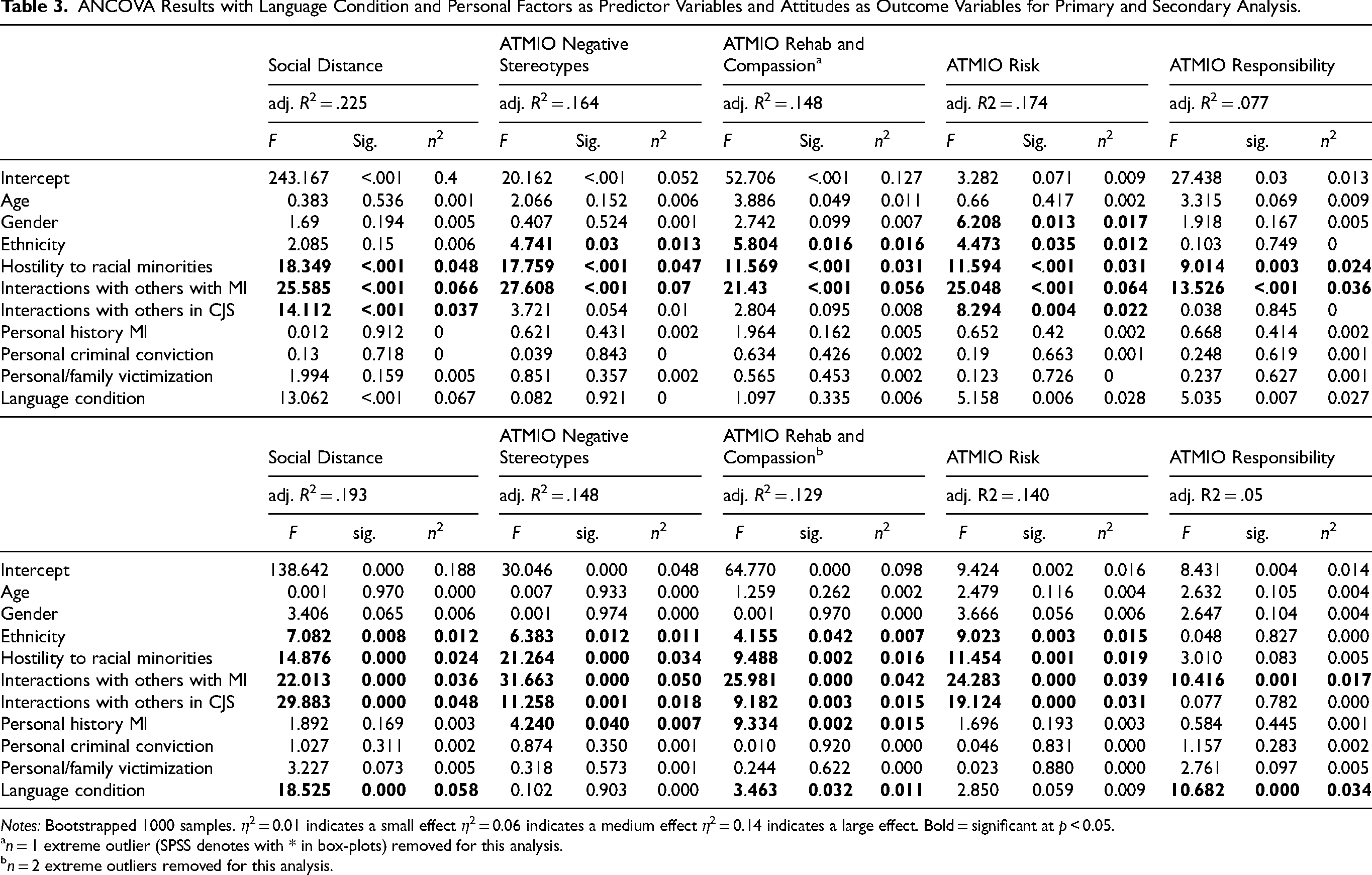
Notes: Bootstrapped 1000 samples. η2 = 0.01 indicates a small effect η2 = 0.06 indicates a medium effect η2 = 0.14 indicates a large effect. Bold = significant at p < 0.05.
n = 1 extreme outlier (SPSS denotes with * in box-plots) removed for this analysis.
n = 2 extreme outliers removed for this analysis.
Where significant differences were observed, post-hoc analysis showed that the person-first, recovery-oriented language was associated with significantly lower desire for social distance scores (M = 12.9) than both “forensic mental health patient” (M = 14.4) and “mentally disordered offender” (M = 15.1), both at p < .001. Person-first, recovery-oriented language was associated with significantly higher perceptions of community risk scores (i.e. meaning lower risk; M = 15.3) than “forensic mental health patient” (M = 13.7) at p < .001. Person-first, recovery-oriented language was associated with significantly lower scores on diminished responsibility (i.e. suggesting higher levels of responsibility for behavior; M = 6.7) than “mentally disordered offender” (M = 7.6) at p = .004. No other significant differences were observed in the post-hoc analyses.
Secondary Analysis of all Respondents (i.e. those Passing and Failing the Attention Screener Question)
We replicated our ANCOVA analyses on the whole sample, including respondents who failed the attention screener question (N = 668). This is shown in Table 3. When controlling for covariates, significant differences by language condition were observed for desire for social distance (p < .001; η2 = 0.058), perceptions of diminished responsibility (p < .001; η2 = 0.034), and support for rehabilitation/compassion (p = .032; η2 = 0.011). No significant differences by language condition were observed for negative stereotypes or perceptions of community risk (though this latter variable neared significance, p = .059; η2 = 0.009).
Where significant differences were observed, post-hoc analysis showed that the person-first, recovery-oriented language was associated with significantly lower desire for social distance scores (M = 12.9) than both “forensic mental health patient” (M = 14.8) and “mentally disordered offender” (M = 15.1), both at p < .001. Person-first, recovery-oriented language was associated with significantly lower scores on diminished responsibility (i.e. suggesting higher levels of responsibility for behavior; M = 7.1) than “mentally disordered offender” (M = 8.1) and “forensic mental health patient” (M = 8.0) at p < .001. Person-first, recovery-oriented language was associated with significantly higher scores on support for rehabilitation/compassion (M = 19.2) than “mentally disordered offender” (M = 18.3) at p = .01. No other significant differences were observed in the post-hoc analyses. Bootstrapped mean scores and 95% CIs for both analyses are reported in Table 4.
Mean Sum Scores on Outcome Measures Across Language Conditions in Primary and Secondary Analysis.
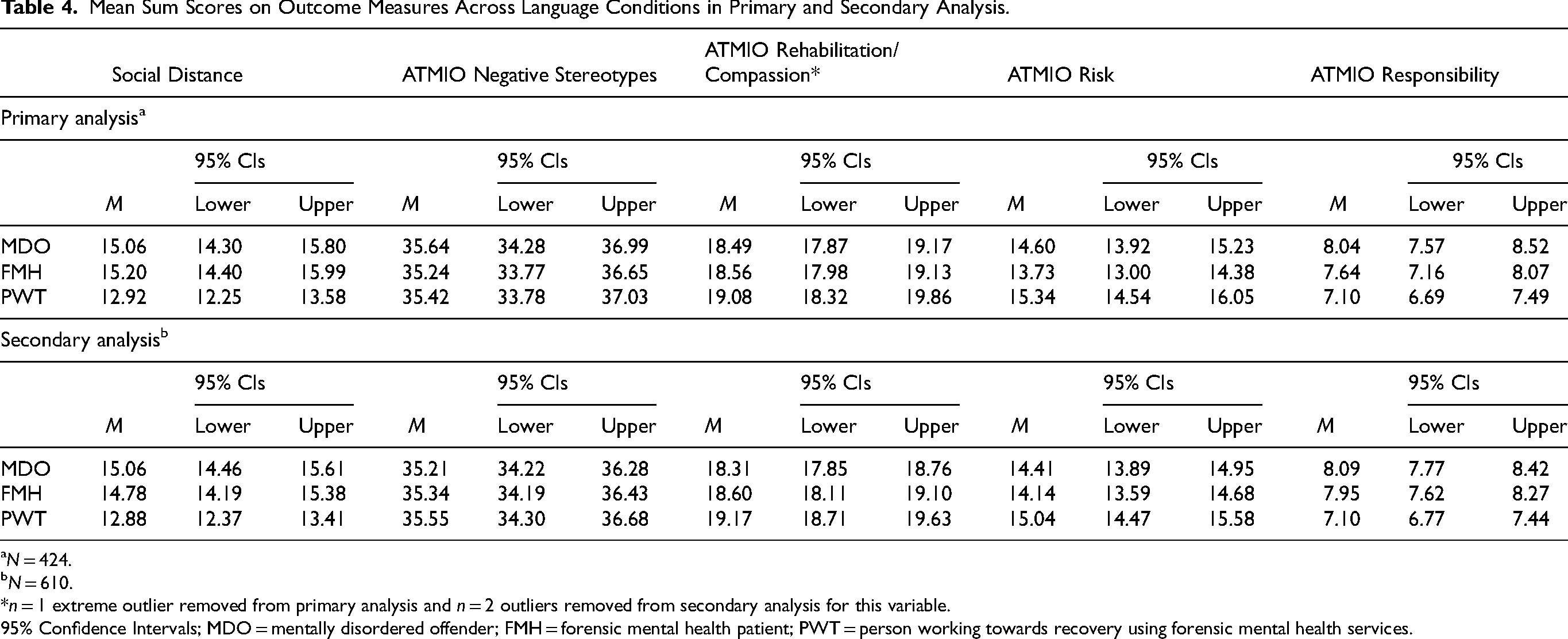
N = 424.
N = 610.
*n = 1 extreme outlier removed from primary analysis and n = 2 outliers removed from secondary analysis for this variable.
95% Confidence Intervals; MDO = mentally disordered offender; FMH = forensic mental health patient; PWT = person working towards recovery using forensic mental health services.
As with the primary analysis, the secondary analysis reported significant associations between language condition and desire for social distance and perceptions of diminished responsibility. The secondary analysis differed from the primary analysis in two respects: 1) perceptions of community risk were not significantly linked to language condition and 2) the relationship between support for rehabilitation/compassion became significant. Hypotheses 1 and 2 were partially supported and there was no evidence to support hypothesis 3 in both the primary and secondary analyses.
Discussion
Our findings suggest that different language used to describe people in forensic mental health services was associated with differences in desire for social distance and perceptions of diminished responsibility in the UK general public.
Specifically, we found that when controlling for other factors, person-first, recovery-oriented language was associated with less desire for social distance, implying more willingness for proximity than the terms “mentally disordered offender” or “forensic mental health patient.” This carried a medium effect size and was found in both our primary and secondary analyses. Greater willingness for proximity to people with mental health disorders or who have offended when described using person-first language has been found in other studies (Baker et al., 2022; Granello & Gibbs, 2016; Granello & Gorby, 2021; Jackl, 2023), though not all (Ashford et al., 2018; Cheema, 2018; Mallinson et al., 2022).
In both our primary and secondary analyses, we found that individuals described using person-first, recovery-oriented language were considered to have more responsibility for their actions than individuals described as mentally disordered offenders. Fausey and Boroditsky (2010) found that using agentive language results in higher attributions of blame and responsibility than non-agentive language. Martinelli et al. (2020) reported a link between person-first language use and stronger attributions of blame. These findings may support the notion that person-first language prioritizes the individual above their condition, emphasizing perceptions of agency. However, studies investigating person-first language in relation to substance use found that person-first language was linked to lower responsibility perceptions by respondents, due in part to attributions linked to neuropsychological problems (Goodyear et al., 2018; Kelly et al., 2010). Research into person-first language use and perceptions of responsibility is therefore mixed and context dependent.
Individuals described using person-first, recovery-oriented language were considered less risky than those described as forensic mental health patients in our study (this result was significant in our primary analysis and neared significance in our secondary analysis). This link has been reported in several studies investigating person-first language and perceptions of recidivism risk in people who have committed violent and sex offences (Harris & Socia, 2016), and general threat in people who use substances (Kelly et al., 2010). However, not all studies have found a significant association between person-first language and risk perceptions (Denver et al., 2017; Goodyear et al., 2018; Martinelli et al., 2020). This mixed evidence might, in part, be due to sample demographics. The different findings across our primary and secondary analysis might be explained by the fact that screener failures were significantly younger; more likely to be male, unemployed, and currently in higher education; and less likely to be a victim of crime in the past 5 years. We found no differences by language condition on negative stereotypes and mixed evidence for attitudes towards rehabilitation and compassion. Unlike our study, Jackl (2023) reported a small link between person-first language use and a reduction in negative stereotypes for people leaving prison. This may be due to the different terms tested by Jackl, for example, “returning citizens,” “person who was formerly incarcerated” and “ex-convict”. Our inclusion of mental illness as a relevant factor may elicit different emotional responses, which may be differentially linked to negative stereotypes. Our findings in relation to perceptions of rehabilitation and compassion place our results in a minority of studies reporting no link. A scoping of the literature found one other study reported no link between person-first language use (Goodyear et al., 2018) and eight reporting a positive relationship between person-first language and support for rehabilitative efforts and/or compassion (Baker et al., 2022; Cheema, 2018; Granello & Gibbs, 2016; Granello & Gorby, 2021; Harris & Socia, 2016; Kelly et al., 2010; Kelly & Westerhoff, 2010; Lowe & Willis, 2022). All those studies employed the same or similar methods to our study design (e.g. vignettes) and the majority used general population samples. However, none of the studies explored attitudes towards people in forensic mental health services. Moreover, these studies used scales specifically designed to measure attitudes towards certain groups (e.g. people with addictions, people who have committed crimes of a sexual nature, or people with mental health conditions outside of forensic services) which are different from the ATMIO. Therefore, items related to support for rehabilitation or compassion were different from the items included in ATMIO, potentially explaining the difference with our findings.
A finding that warrants further examination and understanding is the higher scores measuring perceptions of responsibility when person-first, recovery-oriented language was used. According to the ATMIO measure used in our study, higher responsibility scores in the person-first, recovery-oriented language condition indicate more negative attitudes. In our study, this might mean that people in this language condition were more likely to be seen as responsible for their actions and, by extension, more blameworthy. This might also have implications for how staff view patients and how much responsibility they are ascribed in managing their recovery. Research has found that where language used by clinicians ascribes patients with greater levels of responsibility, these clinicians were less assertive in managing pain for patients with sickle cell disease (Goddu et al., 2018). Our findings raise interesting questions around how we can understand mental illness as a mitigation of responsibility for offending but not use this understanding to deprive patients of taking agency in their own recovery.
Limitations
First, online survey methods are not accessible to many members of the public, and our method of recruitment through the platform Prolific is self-selecting. It is also possible that two or more attention checks would have improved our ability to discern respondents who were paying close attention to the survey and providing more considered answers. Second, the domain of the ATMIO used to measure diminished responsibility had Cronbach's α scores below the customary .7 threshold in two of the language conditions (.647 and .564), suggesting that a better indicator of responsibility could be developed and used. Third, our categorical measure of hostility towards ethnic minorities was highly imbalanced. The primary analysis had 18 and 424 observations in each response category and the secondary analysis had 30 and 599 observations. The reliability of findings relating to this question could be also be affected by social desirability bias or the applicability of this question for people belonging to the “ethnic minority” groups referred to. Finally, collapsing the non-white ethnicities into a single category for inclusion in the ANCOVAs might tell us something about differences between white and non-white people but precludes any comment on differences between people identifying as Asian, Black, Mixed, and Other.
Recommendations for Practice
Use of language is an important but small component of the broader social context within which stigmatizing attitudes and behaviors exist. There are some recommendations for practice relating to language use that can be taken from our study and the wider literature. Studies exploring the quality of forensic mental health documentation found that nurses largely used language that was inappropriate, paternalizing, and lacking a person-centred approach (Martin et al., 2020; Martin & Ricciardelli, 2022). These studies recommend improvements in writing style and vocabulary to increase the positive emotional valence of patient notes and promote more positive impressions of patients (Martin & Stanford, 2020). Healy et al. (2022) proposed that when writing and talking about patients, staff should use language that respects autonomy, avoids pejorative terms like “offender,” acknowledges patients’ multiple identities and conditions to reflect an orientation towards inclusivity, avoids labels like “non-compliant” or “manipulative”, and focuses instead on specific actionable barriers. The authors further recommend that quotes from service users should be used with caution because they may include stereotypical vernacular that elicits attitudes linked to views on socio-economic or ethnic status. Staff should also avoid the use of social identifiers without context, for example, mentioning race/ethnicity without providing a rationale for why this is relevant; avoid blaming terms, such as “refusing” without including reasons for these; and finally be mindful of neutral verb choice, for example writing “patient states” rather than “patient claims” in their notes.
Based on our study's findings, we recommend that person-first and recovery-oriented language should be used by individuals, services, organizations, and policymakers. For example, adopt person-first language in patient notes, information packs provided to patients and carers, and hospital and service models of care. The use of person-first and recovery-oriented language, if incorporated in documents relating to the commissioning of services, on provider websites, international policy documents, legislation and guidance, and in academic scholarship, would enhance respect and appreciation of the person behind any mental health condition or criminal involvement, which is core to person-centred care. Therefore, we recommend that services review internal and external facing documentation. The net consequences of these efforts might benefit stigma reduction and increase willingness of the public and staff to support people in forensic mental health services to reintegrate into their local communities. This would be a small but important aid to recovery.
Recommendations for Future Research
Our research and the suggestions for practice leave open several lines of further inquiry. We found that person-first, recovery-oriented language was positively associated with perceptions of responsibility. This should be explored further in qualitative studies with people in the criminal justice system with mental health conditions and the general public. It was not clear in our study what informed respondents’ attribution of causality and how this was linked to mental health and criminal responsibility. This work should also investigate how people in the criminal justice system with mental health conditions more broadly experience mental health and criminal responsibility, how this is shaped by personal characteristics, how this has/hasn’t changed over time, and what role they see it playing in their recovery. This work should also test the links between social attitudes and both person-first and recovery-oriented language separately as we incorporated both into a single language condition. Future research might replicate our work but assign respondents to different mental health symptoms and conditions to explore diagnostic/symptom-level differences in stigma in the forensic population. Research should longitudinally investigate the links between attitudes, changes in attitudes, and subsequent behaviors e.g. interactions with people in forensic mental health services. Finally, building on the Lancet Commission's recommendations, a stigma reduction intervention should be developed and piloted than seeks to reduce stigma towards people in forensic mental health services.
Conclusion
In conclusion, this novel study makes a significant contribution to knowledge by evidencing the importance of person-first, recovery-oriented language in shaping public attitudes towards people in forensic mental health services. Person-first, recovery-oriented language was associated with less desire for social distance, increased perceptions of responsibility, and more weakly to perceptions of community risk in a nationally representative U.K. sample. These findings add value to existing calls to adopt person-first language by providing robust evidence to demonstrate its links to public attitudes. Our findings will be of interest to other fields where healthcare, social care, or criminal justice staff work with marginalized groups. Further research should explore how stigmatizing attitudes shape real-world behaviors and evaluate the efficacy of interventions developed to reduce stigma towards this population.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding to support this study was provided by the University of Greenwich's Institute for Inclusive Communities and Environments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.