
Abstract
Forensic mental health treatment represents a specialized form of care aimed at stabilizing psychiatric illness, reducing hospital readmission risk, and supporting reintegration into the community. Various factors are consistently associated with forensic mental health and treatment planning. One relevant factor is exposure to an interpersonal potentially traumatic event (PTE), which is common among forensic inpatients. We analyzed data from 5,105 forensic hospital admissions in Ontario, Canada, between 2013 and 2023, examining whether exposure to sexual, physical, and/or emotional abuse relates to psychiatric symptom severity (i.e., aggression, positive symptoms, depressed mood, and manic symptoms). After accounting for confounding factors (age, gender, education), any exposure to PTE was associated with increased severity of positive symptoms, depressed mood, and manic symptoms, but not aggressive behavior. Timing of PTE exposure (within 1 year versus more than 1 year ago) did not relate to outcomes. Effects were more pronounced among sufferers of polytrauma, highlighting the cumulative burden of PTE exposure. PTE exposure was related to greater symptom severity in men and women, but it was associated with aggression and higher symptom severity in cases of polytrauma among women only. These findings underscore the importance of trauma-informed care and gender-responsive approaches in forensic mental health services.
Public Significance Statement
This study examined how exposure to potentially traumatic interpersonal events (PTEs; physical, sexual, and emotional abuse) affects forensic inpatients, with attention to differences between men and women. PTE, and especially having multiple PTE, was associated with more severe psychiatric symptoms in men and women; among women, PTE was linked to higher symptom severity and increased aggression. These findings underscore the importance of trauma-informed care for forensic inpatients with histories of interpersonal trauma.
Introduction
Interpersonal potentially traumatic events (PTEs), including physical, sexual, and emotional abuse, are prevalent among incarcerated adults (Grady et al., 2024; Morrison et al., 2024) and forensic inpatients (McKenna et al., 2019). Notably, exposure to PTE has been associated with more severe mental health difficulties in justice-involved populations (Leidenfrost & Antonius, 2020), increased violence and other behavioral problems among incarcerated and forensic populations (Molina-Coloma et al., 2022), and heightened risk of admission to forensic mental healthcare facilities (Stinson et al., 2021). Thus, forensic inpatients with a history of PTE may represent a particularly vulnerable population, presenting with aggressive behavior and severe psychiatric symptoms, including depression and psychosis (e.g., D’Orta et al., 2023; Jeffery et al., 2024). Behavioral interventions for individuals with a history of PTE have shown beneficial effects for incarcerated adults (e.g., Grady et al., 2024); however, barriers to trauma-informed care have been identified in forensic settings, such as potentially retraumatizing environments and practices, nursing caseloads, and a reactive approach to managing challenges (Seitanidou et al., 2024). Although there is a broad understanding that an association exists between PTE and psychiatric symptoms among forensic care (McKenna et al., 2019; Molina-Coloma et al., 2022; Morrison et al., 2024), questions remain about the role of specific aspects of the PTE including its timing (e.g., recency) and type (e.g., polytrauma), as well as whether there are gender differences. An understanding of the association of PTE with psychiatric symptomatology among forensic inpatients could inform trauma-informed care practices and motivate their implementation in forensic settings. The present study examined a range of PTE and their relation to clinical presentation, including psychiatric symptoms and aggressive behavior, among men and women assessed on admission to hospital.
Forensic inpatient settings attempt to strike a delicate balance between fostering a therapeutic environment that supports recovery while also implementing safety measures to prevent violence toward the patients themselves and to others (Marklund et al., 2020); however, these settings pose the potential for retraumatization for individuals with a history of PTE (Seitanidou et al., 2024), particularly for women who are forensic inpatients (Grimbos et al., 2016; Nicholls et al., 2015). Forensic facilities, compared to other inpatient hospital settings, appear to enforce stricter security protocols that limit privacy, restrict movement and visitation, and reduce access to the outside world (Nicholls et al., 2015; Rodwell & Frith, 2024). Staff also frequently rely on coercive interventions, such as restraint and seclusion (Ham et al., 2025), which can inadvertently trigger traumatic responses and exacerbate psychiatric symptoms. Scholars have argued that these practices are particularly distressing for individuals with a history of PTE and may ultimately worsen mental illness, perpetuating the very behaviors that require risk management (Rodwell & Frith, 2024). There is also evidence that violence risk management differs by gender in that women are more likely to be placed in seclusion than men (Nicholls et al., 2009) and more likely secluded after multiple attempts to use acute control medications (Mathias & Hirdes, 2015), raising the need for gender-responsive treatment approaches. Improved understanding of PTE and their relation to aggressive behavior and psychiatric symptoms in men and women is needed to support trauma-informed risk management in forensic settings.
Gender differences in aggressive behavior and psychiatric symptoms among forensic inpatients are also poorly understood (Grimbos et al., 2016; Nicholls et al., 2015; Streb et al., 2021). Preliminary evidence suggests that women show more sequelae of PTE than men, including more severe aggressive behavior (Grimbos et al., 2016; Nicholls et al., 2015) and mental health difficulties (Grimbos et al., 2016; Karlsson & Zielinski, 2020). However, gender differences in PTE exposure have been largely understudied, partly due to the overrepresentation of men in general forensic research (Nicholls et al., 2015; Streb et al., 2021) as well as a failure to contextualize PTE in relation to symptoms and behavior (Morrison et al., 2024). Furthermore, while research on forensic inpatients who are women often focuses on PTE, this factor is not often considered in men who may also be significantly affected yet less likely to disclose PTE (de Vogel et al., 2025; Hine et al., 2021; Sorsoli et al., 2008). This work highlights ways in which both women's and men's experiences are often underrecognized in the literature and the need for further attention to PTE exposure and gender differences in psychiatric symptom severity.
While PTE have been consistently associated with psychiatric diagnoses like borderline personality disorder (de Vogel & de Ruiter, 2005; Rodwell & Frith, 2024), with differential effects between men and women depending on the type of exposure (Bohle & de Vogel, 2017), their relationship to behavior and symptom expression remains less well understood. This is a significant gap, as the assessment of behaviors and symptoms is essential for informing treatment and care planning in forensic inpatient mental health services (Hirdes et al., 2020). A few studies have examined specific characteristics of PTE that may be particularly likely to exacerbate psychiatric behaviors and symptoms, including event timing and type. For instance, exposure to PTE in childhood has been shown to more strongly predict forensic hospital readmission in men than exposure in adulthood (Jeffery et al., 2024). In contrast, others have found that adulthood exposure to PTE is a stronger predictor of psychiatric symptoms (Wolff & Shi, 2012). Similarly, Behdinan et al. (2024) reported that, among psychiatric inpatients, recent PTE exposure (within the past year) was associated with greater severity of aggressive behavior, positive symptoms, depressed mood, and manic symptoms compared to exposure that occurred over a year ago (i.e., remote exposure). Together, these findings suggest a possible association between the recency of exposure and variations in psychiatric outcomes, which has yet to be explored among forensic inpatients.
Among victimized youth, polytrauma (i.e., exposure to multiple types of interpersonal PTE) was more strongly associated with symptoms of anxiety, depression, and anger than exposure to a single type of PTE (Finkelhor et al., 2007). The cumulative effect of childhood adversity has also been implicated in forensic mental health outcomes, with greater exposure to PTE associated with more severe mental health problems (McLachlan et al., 2024). For incarcerated men, exposure to any single form of interpersonal PTE was associated with psychopathological problems (e.g., aggression), though physical abuse was a stronger predictor than sexual abuse (Wolff & Shi, 2012). Conversely, sexual abuse was found to be the only type related to personality disorder diagnosis in men who were forensic inpatients (Bianchini et al., 2022). However, these studies focused only on men or youth populations. Similarly, Behdinan et al. (2024) did not observe any differences by PTE type, although forensic inpatients were excluded from their analysis and gender differences were not considered. Given these gaps, there remains a need to understand how interpersonal PTE exposure differentially impacts forensic inpatient psychiatric behaviors and symptoms based on the timing and type of exposure. Moreover, greater attention to gender-specific patterns is needed to improve the efficacy of risk assessment for forensic inpatient populations (Nicholls & Goossens, 2017).
Present Study
The present study examined an extensive healthcare database of men and women admitted to forensic hospitals across an entire Canadian province. We examined whether having a history of interpersonal PTE was associated with the severity of aggressive behavior and psychiatric symptoms, including positive symptoms, depressed mood, and mania. We hypothesized that having a history of PTE would be positively associated with all clinical measures (Hypothesis 1). We further examined whether this relationship varied by timing and type of exposure. We hypothesized that timing (i.e., recent or remote) and type (i.e., sexual, physical, or emotional abuse, or a combination of two or more) of exposure will be related to greater behavior and symptom severity on all clinical measures, with stronger associations for recent PTE compared to remote PTE (Hypothesis 2), and for polytrauma (i.e., both recent and remote exposure) compared to exposure to a single type (Hypothesis 3), respectively. We also explored gender differences in the presence of a history of PTE and its association with aggressive behavior and psychiatric symptom severity. We hypothesized that gender differences would be observed, with symptoms more severe in women than in men (Hypothesis 4).
Methods
Open Science and Transparency
This population-based, cross-sectional cohort study used routinely collected data on all individuals admitted to forensic inpatient hospital beds in Ontario, Canada, between April 2013 and March 2023. Data were extracted from the Ontario Mental Health Reporting System, which includes detailed sociodemographic and assessment information documented by clinicians for all adults admitted to designated psychiatric beds in the province of Ontario. Disclosure of health system information within the Ontario Mental Health Reporting System does not require patient consent under the Personal Health Information Protection Act (2004). The use of these data for secondary analysis was reviewed and approved by the Research and Ethics Board of Waypoint Centre for Mental Health Care (protocol number HPRA 24.07.29), a specialized psychiatric hospital that served as the hub for data collection and collation. The study was not preregistered, and the data are not publicly available due to restrictions under the Personal Health Information Protection Act (2004).
Study Design
In Canada, individuals with mental illness who become involved in the criminal justice system and are deemed unfit to stand trial or not criminally responsible (NCR) are diverted into the forensic mental health system (Criminal Code, 1985; Mental Health Act, 1990). In Ontario, the Ministry of Health funds 10 hospital-led forensic mental health programs, including some of the largest in the country (Chaimowitz et al., 2022), as mandated under the Criminal Code of Canada (Criminal Code, 1985). These programs provide a range of services to treat and facilitate safe reintegration into the community, with lengths of stay varying according to clinical need, ranging from short-term assessments (∼3 days) to extended admissions lasting a year or more (Bettridge & Barbaree, 2012).
Data from the Resident Assessment Instrument-Mental Health (RAI-MH) were extracted for analysis. The RAI-MH is a standardized assessment tool completed by trained clinical staff (e.g., nurses, social workers) within the first 3 days of admission. Early completion of the RAI-MH is intended to support timely identification of patient needs and risk factors, facilitating appropriate intervention and care planning. Information is gathered through structured interviews with the patient and family members, as well as input from other clinicians. The RAI-MH provides a profile of the patient across multiple domains, including physical and mental health, social supports, healthcare utilization, and general hospital care relevant to the functioning of admitted mental health inpatients (Canadian Institute for Health Information [CIHI], 2023).
The RAI-MH has demonstrated consistent evidence of interrater reliability and validity, making it a useful tool for research examining various psychiatric behaviors and symptoms (Hirdes et al., 2020). Moreover, a key advantage of this tool is its inclusion of validated clinical scales measuring psychiatric symptoms, including the Aggressive Behavior Scale (ABS; internal consistency Cronbach's α = .60–.77), the Positive Symptoms Scale-Long version (PSS; α = .71–.74), the Depression Severity Index (DSI; α = .71–.89) and the Mania Scale (α = .61–.77; Hirdes et al., 2002, 2020). Additionally, the RAI-MH collects patient-reported stressful life events, including three items assessing physical, sexual, or emotional abuse. For each type of PTE, items indicate when each event occurred: more than 1 year ago, 31 days to 1 year ago, 8 to 30 days ago, 4 to 7 days ago, or within the last 3 days (CIHI, 2023).
Study Population
The original sample included 9,756 forensic patient admissions. Duplicate admissions were identified using the encrypted Ontario health identification number. Patients admitted without an Ontario health identification number (e.g., out-of-province cases) had a nonunique identification number and we excluded them from the analysis (n = 472). For patients with multiple admissions, we retained only the first admission based on the date the initial assessment was recorded (day/month/year). We excluded 4,177 cases as they represented duplicate data for those with multiple admissions (n = 1,837), and two cases were removed due to gender identity listed as “other.” This resulted in a final sample of N = 5,105 participants, including women (n = 868, 17%) and men (n = 4,237), aged 17 to 95 years (M = 37.3, SD = 13.2).
Interpersonal PTE was defined as any exposure to physical abuse or assault, sexual abuse or assault, or emotional abuse prior to hospital admission documented on the RAI-MH. To analyze PTE characteristics, exposure was grouped according to type (exposure to only physical, sexual, or emotional abuse) or a combination of two or more (polytrauma). 1 PTE timing data were categorized as remote (more than 1 year ago) or recent (1 year to within the last 3 days) for analysis, in accordance with previous research (Behdinan et al., 2024). Patients without a history of interpersonal PTE served as the control group for reference in the analyses.
Outcome Variables
The outcome variables include admission scores from the RAI-MH, including the ABS, PSS, DSI, and Mania Scale. All items on each measure are scored from 0 (not exhibited) to 3 (exhibited daily). The ABS measures aggressive behavior across four items (verbal abuse, physical abuse, socially inappropriate/disruptive behavior, resistance to care), with a total score ranging from 0 to 12. The PSS measures positive symptoms across eight items (hallucinations, command hallucinations, delusions, abnormal thought process/form, inflated self-worth, hyperarousal, pressured speech, abnormal/unusual movements), with a total score ranging from 0 to 24. The DSI measures depressed mood across five items (sad or pained facial expressions, negative statements, self-depreciation, guilt/shame, hopelessness), with a total score ranging from 0 to 15. Lastly, the Mania Scale measures manic symptoms across seven items (inflated self-worth, hyperarousal, irritability, increased sociability/hypersexuality, pressured speech, labile affect, sleep problems due to hypomania), with a total score ranging from 0 to 20 (Canadian Institute for Health Information, 2023; Hirdes et al., 2020). These variables were analyzed continuously, with higher values indicating greater symptom severity.
Covariate Variables
Certain variables were also extracted from the RAI-MH to control for potential confounding effects, and included age, gender, education, income, primary psychiatric diagnosis, and substance use (Akram et al., 2020; Girasek et al., 2022), and to describe the sample (Chaimowitz et al., 2022). These variables are indicated as covariates in the literature due to their established associations with psychiatric outcomes (Akram et al., 2020; Girasek et al., 2022), and PTE exposure (Behdinan et al., 2024). Education was categorized based on the highest level of attainment: high school or less (i.e., no formal schooling, 8th grade or less, 9th to 11th grade, completed high school), and more than high school (i.e., some college or university, diploma or bachelor's degree, technical or trade school, graduate degree or higher) or is unknown. Income was grouped into two categories: no income and some form of income (i.e., pension, disability, social assistance, employment, employment insurance, multiple income sources, or other). Primary psychiatric diagnosis was categorized according to Diagnostic and Statistical Manual of Mental Disorders (DSM)-4 or DSM-5 criteria (American Psychiatric Association, 2013), including psychotic disorders, substance use disorders, mood and anxiety disorders, neurocognitive disorders, personality disorders, neurodevelopmental disorders, other, or not applicable. Substance use was grouped based on recent use (within the past year) of alcohol or any drug, including opioids, cannabis, stimulants, cocaine, hallucinogens, and inhalants. Please refer to Table 1.
Descriptive Statistics.
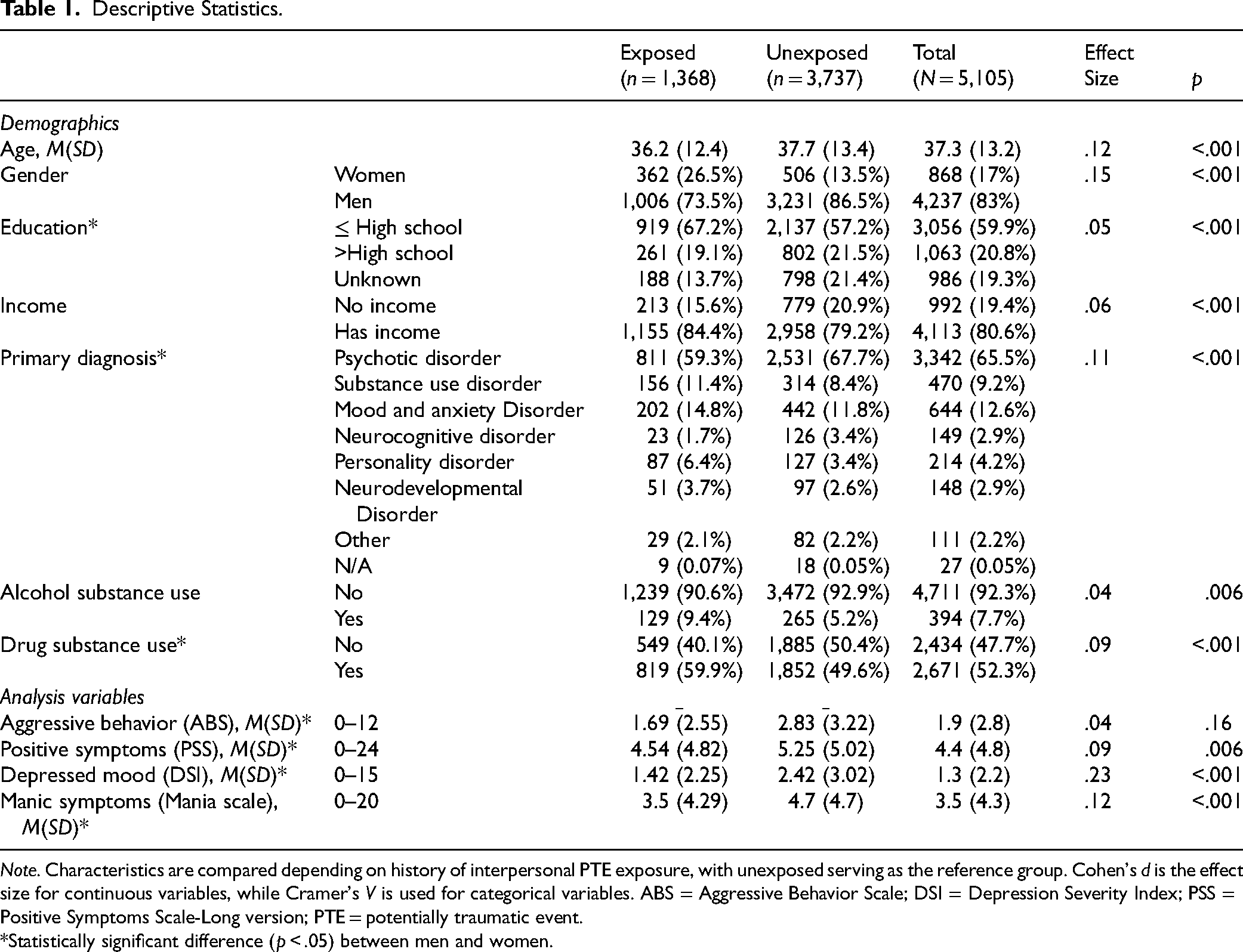
Note. Characteristics are compared depending on history of interpersonal PTE exposure, with unexposed serving as the reference group. Cohen's d is the effect size for continuous variables, while Cramer's V is used for categorical variables. ABS = Aggressive Behavior Scale; DSI = Depression Severity Index; PSS = Positive Symptoms Scale-Long version; PTE = potentially traumatic event.
*Statistically significant difference (p < .05) between men and women.
Statistical Analyses
Statistical analyses were conducted in SPSS, version 30. Independent samples t-tests and chi-square analyses were used to assess group differences for descriptive characteristics and to examine gender differences. The strength of relationships was estimated with Cohen's d and Cramér's V for continuous and categorical outcomes, respectively (Ben-Shachar et al., 2023). First, we hypothesized that any history of interpersonal PTE would be positively associated with all clinical outcomes. To test this, we followed the approach in the literature (Behdinan et al., 2024) and conducted a multifactorial general linear model (GLM) that included trauma exposure (exposed, unexposed [referent]) as the predictor, all outcome measures (ABS, PSS, DSI, and Mania Scale) as dependent variables, and all covariates. Second, we hypothesized that recent PTE exposure would be more strongly associated with clinical outcomes than remote exposure. This was tested using another multifactorial GLM, instead with timing of PTE exposure (recent, remote, unexposed [referent]) as the predictor. Third, we hypothesized that polytrauma would show a stronger association with clinical outcomes than exposure to a single type of PTE. A third multifactorial GLM was conducted, instead using type of PTE exposure (sexual abuse, physical abuse, emotional abuse, polytrauma, unexposed [referent]) as the predictor. Lastly, we hypothesized that clinical outcomes would be more severe among exposed women compared to exposed men. To examine this, we stratified the dataset by gender and conducted three additional multifactorial GLMs to compare the effects of each PTE exposure predictor between men and women, using the same outcomes and covariates. For each multivariate analysis (six total), all outcomes were included simultaneously in the model. All reported mean differences were adjusted for covariates. Confidence intervals are reported at 95% with statistical significance set at p < .05. Although there were no missing data, some cases had unknown values for education (n = 986, 19.3%), which were treated as having education (i.e., the control group).
Assumption Checks
Preliminary analyses were conducted to evaluate whether the assumptions of a multivariate GLM were met. Inspection of residual plots indicated that normality was generally satisfied, with only slight deviations in skew (skewness range = 1.10–2.39). Such deviations are unlikely to substantially bias parameter estimates in samples over 500, and variable transformations were not applied to avoid introducing unnecessary error or bias (Knief & Forstmeier, 2021). However, homogeneity of covariance matrices was violated, as indicated by a significant Box's M test, M = 91.9, F(10, 31608454.71) = 9.18, p < .001). Therefore, Pillai's Trace was used because of its relative robustness to covariance heterogeneity (Nimon, 2012; Olson, 1976). To address violations of homogeneity, nonparametric bootstrapping with 2,000 resamples and 95% confidence interval (CI) around mean values was performed to obtain more accurate estimates (Eck, 2018; Fox, 2016).
Results
Descriptive Characteristics
Approximately 27% (n = 1,368) of the sample reported PTE exposure. Characteristics for both exposed and unexposed (n = 3,737) forensic inpatients are presented in Table 1.
Main Effects
Association of PTE Exposure with Symptom Severity and Aggression
On average, forensic inpatients with PTE exposure (n = 1,368, 27%) had statistically significantly higher scores on the PSS, the DSI, and the Mania Scale compared to those without exposure (n = 3,737, 73%). However, no significant differences were found for the ABS. Inpatients with any history of interpersonal PTE exposure had higher scores on the PSS (adjusted mean difference [aMD] = 0.43, 95% CI [0.14, 0.72], p = .004), DSI (aMD = 0.37, 95% CI [0.23, 0.51], p < .001), and Mania Scale (aMD = 0.34, 95% CI [0.08, 0.61], p = .012). See Table 2 and Figure S1 for an overview of these results.
Results for All Symptoms and Potentially Traumatic Event Characteristics.
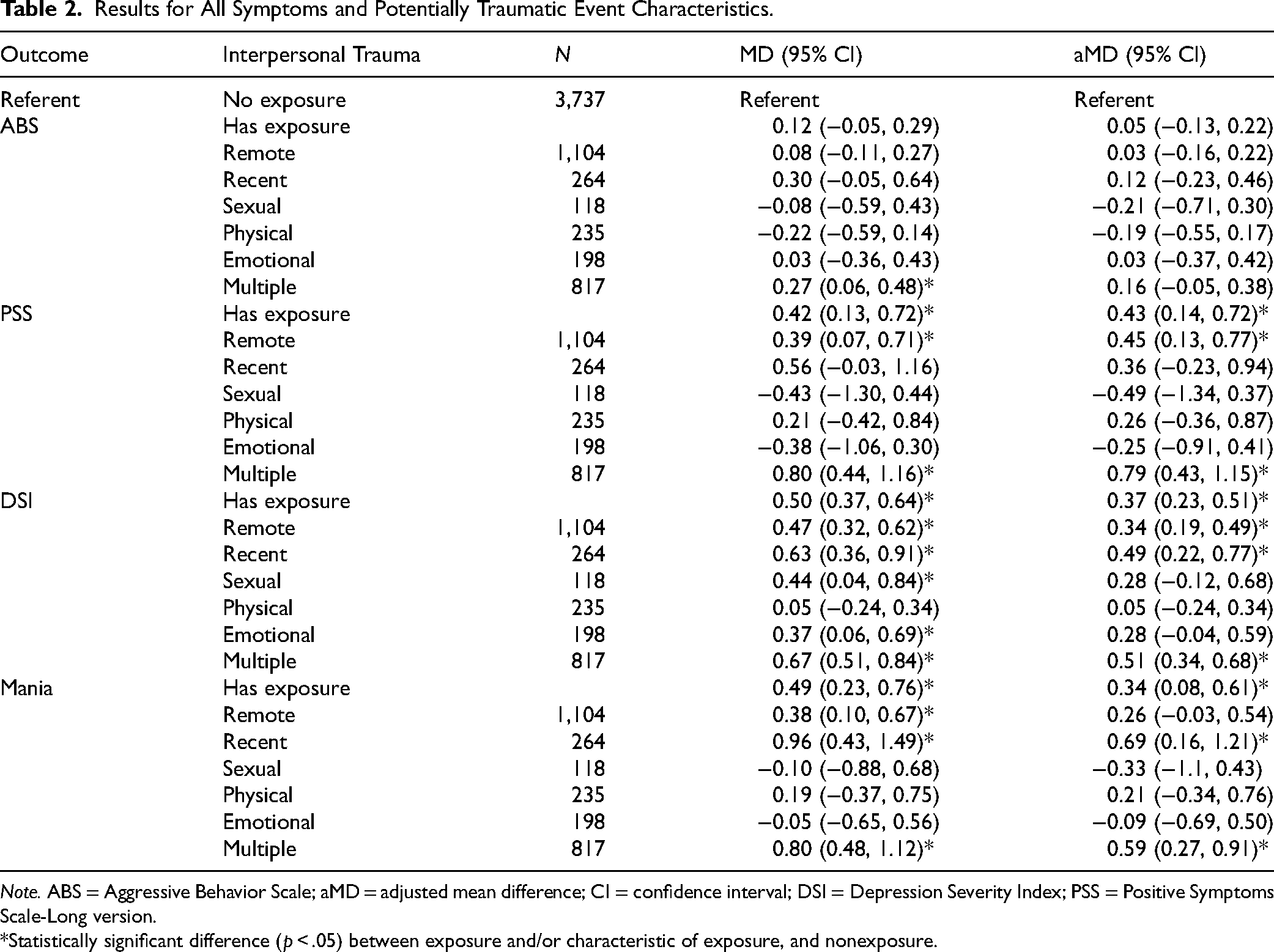
Note. ABS = Aggressive Behavior Scale; aMD = adjusted mean difference; CI = confidence interval; DSI = Depression Severity Index; PSS = Positive Symptoms Scale-Long version.
*Statistically significant difference (p < .05) between exposure and/or characteristic of exposure, and nonexposure.
PTE Characteristics Associated with Symptom Severity and Aggression
First, timing was considered based on recent (n = 264, 19%) or remote (n = 1,104, 81%) exposure. Again, no significant effects were observed for scores on the ABS. For the PSS, inpatients with remote exposure had higher scores than those without exposure (aMD = 0.45, 95% CI [0.13, 0.77], p = .006), but no significant difference was observed for those with recent exposure (aMD = 0.36, 95% CI [−0.23, 0.94], p = .23). For the DSI, having both remote (aMD = 0.34, 95% CI [0.19, 0.49], p < .001) and recent (aMD = 0.49, 95% CI [0.22, 0.77], p < .001) exposure was associated with increased symptom severity compared to those without exposure, but no significant difference was found between remote and recent exposure (aMD = 0.24, 95% CI [−0.14, 0.45], p = .31). For the Mania Scale, recent (aMD = 0.69, 95% CI [0.16, 1.21], p = .01), but not remote (aMD = 0.26, 95% CI [−0.03, 0.54], p = .08) exposure was related to higher scores compared to those without exposure. Regarding type, significantly higher scores were observed among inpatients with polytrauma (n = 817, 60%), for the PSS (aMD = 0.79, 95% CI [0.43, 1.15], p < .001), DSI (aMD = 0.51, 95% CI [0.34, 0.68], p < .001), and Mania (aMD = 0.59, 95% CI [0.27, 0.91], p < .001), but not the ABS (aMD = 0.16, 95% CI [−0.05, 0.38], p = .13). No significant effects were found for isolated exposure to physical (n = 235, 17%), sexual (n = 118, 9%), or emotional abuse (n = 198, 15%). See Table 2 and Figure S2 for an overview of these results.
Gender Differences in the Relation Between PTE Exposure, Symptoms, and Aggression
Aggressive Behavior
Women with PTE exposure (n = 362, 26%) had higher ABS scores (aMD = 0.49, 95% CI [0.06, 0.92], p = .03) than women without exposure (n = 506; 14%). This effect was observed for women with remote exposure (n = 274, 76%; aMD = 0.47, 95% CI [0.00, 0.94], p = .05), but not recent exposure (n = 88, 24%; aMD = 0.54, 95% CI [−0.17, 1.26], p = .14). Women exposed to polytrauma (n = 255, 70%; aMD = 0.90, 95% CI [0.22, 1.18], p = .005) had higher ABS scores, but not those exposed to one type of PTE, including sexual (n = 38, 11%), physical (n = 28, 8%) or emotional (n = 41, 11%) abuse. No significant differences in aggressive behavior as a function of PTE were observed for men.
Positive Symptoms
Among women with PTE exposure (n = 362, 26%), only those with polytrauma (n = 255, 70%) had significantly greater PSS scores than those without exposure (n = 506, 14%; aMD = 0.88, 95% CI [0.13, 1.64], p = .02). For exposed men (n = 1,006, 74%), those with any exposure had greater PSS scores than those without exposure (n = 3,231, 86%; aMD = 0.46, 95% CI [0.14, 0.79], p = .006), particularly those with remote exposure (n = 830, 83%; aMD = 0.44, 95% CI [0.09, 0.80], p = .01) or polytrauma (n = 562, 56%; aMD = 0.75, 95% CI [0.33, 1.16], p < .001) but no effects were observed for recent exposure (n = 176, 18%), nor for exposure to only sexual (n = 80, 8%), physical (n = 207, 21%), or emotional (n = 157, 16%) abuse.
Depressed Mood
Both women and men with PTE exposure showed greater symptom severity compared to those without exposure, with a stronger effect observed for women (aMD = 0.74, 95% CI [0.38, 1.10], p < .001) compared to men (aMD = 0.27, 95% CI [0.12, 0.41], p < .001). Both remote (women: n = 274, 76%; aMD = 0.76, 95% CI [0.36, 1.15], p < .001; men: n = 830, 83%; aMD = 0.23, 95% CI [0.07, 0.39], p = .005) and recent (women: n = 88, 24%; aMD = 0.69, 95% CI [0.09, 1.29], p = .02; men: n = 176, 18%; aMD = 0.42, 95% CI [0.11, 0.74], p = .008) exposure was associated with higher DSI scores. For women, exposure to sexual abuse (n = 38, 11%; aMD = 0.95, 95% CI [0.04, 2.05], p = .03), emotional abuse (n = 41, 11%; aMD = 1.01, 95% CI [0.18, 1.90], p = .02), or polytrauma (n = 255, 70%; aMD = 0.76, 95% CI [0.36, 1.17], p < .001) was associated with higher DSI scores. For men, only those with polytrauma (n = 562, 56%) had higher DSI scores (aMD = .41, 95% CI [0.22, 0.60], p < .001).
Manic Symptoms
In general, only men with PTE exposure (aMD = 0.31, 95% CI [0.02, 0.61], p = .04) had statistically significantly higher Mania scores than those without exposure, and only men with recent (n = 88, 18%; aMD = 0.75, 95% CI [0.13, 1.37], p = .02), but not remote (n = 274, 83%; aMD = 0.22, 95% CI [−0.10, 0.53], p = .18) exposure. For both genders, polytrauma exposure was associated with greater symptom severity, with a stronger effect observed for women (n = 255, 70%; aMD = 0.91, 95% CI [0.20, 1.62], p = .01) compared to men (n = 562, 56%; aMD = 0.45, 95% CI [0.08, 0.82], p = .02). See Table 3 for an overview of these results.
Adjusted Mean Differences by Gender.
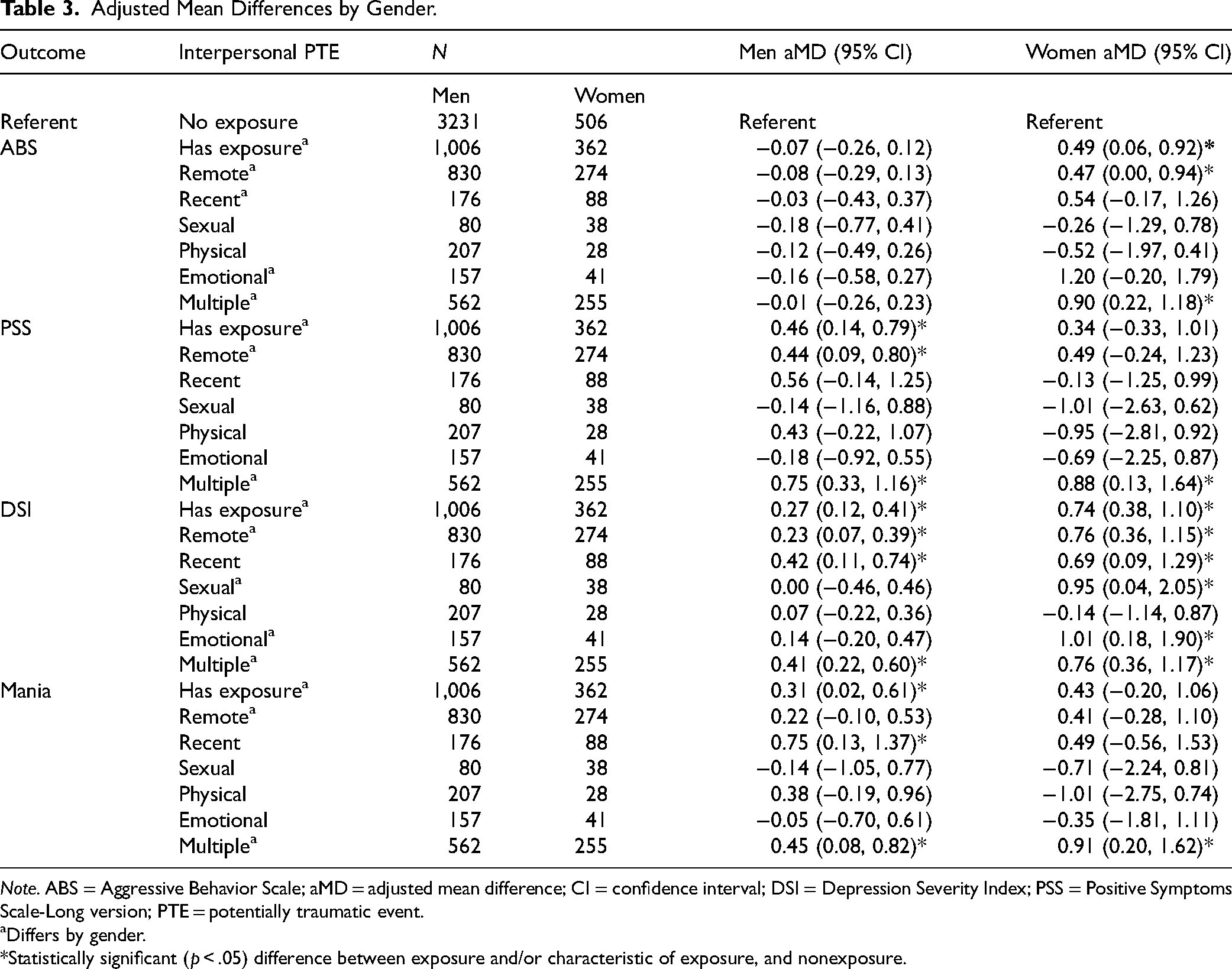
Note. ABS = Aggressive Behavior Scale; aMD = adjusted mean difference; CI = confidence interval; DSI = Depression Severity Index; PSS = Positive Symptoms Scale-Long version; PTE = potentially traumatic event.
Differs by gender.
*Statistically significant (p < .05) difference between exposure and/or characteristic of exposure, and nonexposure.
Discussion
Inspired by previous findings that forensic inpatients experience severe psychiatric symptoms affecting their treatment trajectory and recovery (Chaimowitz et al., 2022; D’Orta et al., 2023) and that these symptoms are related to interpersonal PTE (Behdinan et al., 2024), we examined the relationship between interpersonal PTE and psychiatric symptom severity in a secondary analysis of healthcare assessments among forensic inpatients in Ontario, Canada. First, we compared aggressive behavior and psychiatric symptom severity in exposed and unexposed inpatients. Then, we examined how timing and types of exposure related to these outcomes, followed by an analysis of gender differences. All findings were adjusted for potential confounding factors, including age, gender, education, income, psychiatric diagnosis, and substance use.
We found that PTE exposure was associated with increased severity of positive symptoms (as measured by the PSS), depressed mood (as measured by the DSI), and manic symptoms (as measured by the Mania Scale), but not aggressive behavior (as measured by the ABS). No significant differences in symptom severity by exposure timing were observed. However, only remote exposure was associated with greater severity of positive symptoms, while recent exposure was related to significantly greater severity of manic symptoms. The effects were most pronounced among those with polytrauma (vs single types), underscoring the cumulative impact of PTE. This cumulative effect of PTE has been well-documented, with greater exposure often relating to more severe outcomes (Finkelhor et al., 2007; Zoromba et al., 2024).
In our sample, approximately 27% reported exposure to at least one form of interpersonal PTE. Although this rate is higher than that reported among general psychiatric inpatients assessed using the RAI-MH (22.4%; Behdinan et al., 2024), it is lower than estimates from prior studies of forensic inpatients who had a personality disorder (36.5%; Bohle & de Vogel, 2017), were women with intellectual disabilities (58%; de Vogel & Didden, 2022), and men reporting childhood interpersonal PTE (61.5%; Fosse et al., 2021). Given that our sample included more men than women, men may have underreported exposure to interpersonal PTE, which could have affected prevalence estimates (de Vogel et al., 2025). Indeed, men may be less likely to disclose experiences of abuse due to societal expectations surrounding masculinity. These norms often discourage expressions of vulnerability and frame victimization as inconsistent with masculine identity, leading to fears of ridicule, blame, or disbelief that can affect reporting behavior (Hine et al., 2021).
Beyond differences based on exposure, additional gender-specific patterns emerged. Among women, PTE exposure was associated with greater severity of aggressive behavior, depressed mood, and positive and manic symptoms in cases of polytrauma. Among men, exposure was associated with increased severity of depressed mood, positive symptoms and manic symptoms, but not aggressive behavior. With respect to PTE timing, no significant differences were observed between genders in recent and remote exposure groups. However, among women, only remote exposure was related to aggressive behavior, whereas in men, remote exposure was related to positive symptoms and recent exposure to manic symptoms. For both genders, experiencing polytrauma was associated with greater symptom severity, though only women with polytrauma showed significantly greater aggressive behavior. Furthermore, symptom severity in women, but not men, was associated with isolated types of PTE, with emotional or sexual abuse related to greater severity of depressed mood.
These findings highlight nuanced gender differences that extend previous research on forensic inpatients. Earlier work has reported inconsistent results, with some studies finding no gender differences in aggression (de Vogel & de Ruiter, 2005; Nicholls et al., 2009; Streb et al., 2021), positive symptoms (Nicholls et al., 2015), or depressed mood (Streb et al., 2021). Conversely, Mathias and Hirdes (2015) reported that women had lower scores for aggression, depressed mood, and manic symptoms than men (Mathias & Hirdes, 2015). Additionally, Grimbos et al. (2016) identified gender differences, noting that among forensic populations, women may be particularly vulnerable to risk factors for violent behavior, such as lack of social support and stress. However, these studies did not account for interpersonal PTE, which the present study suggests may help inform differences observed in psychiatric symptom severity across men and women.
Although aggression did not overall differ based on PTE exposure, a gender-specific pattern emerged, such that only women with exposure had greater aggressive behavior. Notably, among those with reported polytrauma, women showed greater symptom severity across all outcome measures, with greater effects observed compared to men. This aligns with prior work suggesting that women who are forensic inpatients are especially impacted by PTE (Grimbos et al., 2016; Nicholls et al., 2015). It is possible that other factors more strongly predict aggressive behavior among men, such as meanness (Eisenbarth et al., 2021) or moral cognition (Badruddin et al., 2024). For instance, compared to women, men's responses to emotionally salient moral judgements are more often oriented towards harming others to achieve perceived justice, whereas women's responses are more often aimed at avoiding harm to others (Efferson & Glenn, 2018; Fumagalli et al., 2010). If predisposing orientations are particularly strong among men, it could explain the null effects of PTE on aggression for men in the present study, but the relation appears more complex for women. Future research that examines both predisposing characteristics and environmental exposures could further elucidate the role of PTE in aggression among men and women.
Several contextual factors may also contribute to these apparent differences. Depressive symptoms are less frequently identified in men than in women, and men may find PTE more difficult to disclose, potentially obscuring trauma-related effects (de Vogel et al., 2025). In addition, differences in care practices may influence how symptoms are observed and recorded. For example, among forensic inpatients, women are more often placed under enhanced observation than men. This can not only exacerbate distress but may also increase the likelihood that clinical staff document incidents, potentially inflating apparent symptom severity (Lawrence et al., 2025). Further, while greater positive and manic symptom severity was observed for men with any history of exposure, this effect was only observed in the presence of polytrauma among women. Timing effects also varied by gender: remote exposure was associated with aggressive behavior in women, while in men, remote exposure was associated with positive symptoms and recent exposure with manic symptoms. Thus, trauma-related effects observed in forensic inpatients may vary by pattern of exposure and across genders, highlighting the need for further investigation to clarify risk profiles.
Practice and Policy Impact
Trauma-informed treatment has been proposed to improve forensic mental health services, address psychiatric symptoms, and reduce the risk of readmission (Grimbos et al., 2016; Jeffery et al., 2024; Seitanidou et al., 2024; Simjouw et al., 2024). Failing to consider PTE in this population may have serious consequences, including an increased risk of retraumatization and provoking an unsafe environment (Rodwell & Frith, 2024). The coercive and controlling practices used in forensic care settings may resemble past PTE experiences, leading to distress that is misinterpreted as a symptom of mental illness rather than a trauma response. This can create a cycle wherein staff respond with further coercion, potentially worsening disruptive behaviors (Lawrence et al., 2022; Rodwell & Frith, 2024). In contrast, trauma-informed care practices have the potential to improve both environmental safety and patient treatment outcomes (Seitanidou et al., 2024; Simjouw et al., 2024).
Although research on trauma-informed treatment in forensic inpatient populations remains limited, the existing evidence is promising. It has been successfully implemented in other inpatient and acute mental health settings (Beckett et al., 2017), as well as juvenile justice health systems (Branson et al., 2017). Its implementation has led to greater collaboration between staff and patients, reduced stress and greater sense of safety among patients, and less use of restraints (Simjouw et al., 2024). Findings from our study suggest that patterns of PTE exposure may differentially relate to mental health difficulties in forensic inpatients, particularly between men and women, highlighting the need to explore trauma-informed practices tailored to this population.
Researchers have expanded on gender-responsive care frameworks and provided recommendations for forensic mental health treatment (e.g., de Vogel et al., 2025; Nicholls et al., 2017). These frameworks emphasize that gender differences influence not only the manifestation and recognition of symptoms but also the accessibility and effectiveness of interventions. To provide individualized treatment, interventions should therefore be tailored to account for gender-specific needs and experiences. This has important implications for policy and clinical practice; integrating trauma-informed and gender-responsive approaches to diagnosis, risk assessment, and treatment represents the next crucial step for the field. For example, de Vogel and colleagues (2025) advocate for gender-sensitive forensic environments that acknowledge gender differences while promoting safety and equity, such as curating carefully structured mixed-gender settings that balance opportunities for interaction with protections against potential risks. Incorporating assessments of PTE and trauma-related symptoms into diagnostic evaluations is essential, alongside recognition of gender diversity, to ensure care is both inclusive and responsive to the gender experiences in forensic populations (de Vogel et al., 2025; Nicholls et al., 2017).
Strengths
Our study has several notable strengths. First, our analysis includes a large sample size representing forensic inpatient populations over a decade from a diverse province in Canada. We employed a statistical model that controls for multiple confounding factors associated with psychiatric symptoms, thereby enhancing the validity of our findings. Notably, we include a substantial sample of women, contributing to a better understanding of outcomes among women who are forensic inpatients and how they compare with men—an area in need of further research. Our findings help fill a critical gap in the literature concerning gender differences in forensic populations and expand previous research by identifying various characteristics that may inform our understanding of their risks and treatment needs.
Limitations and Future Directions
Despite these strengths, our study is not without limitations. First, the use of secondary data limited the inclusion of additional factors. For instance, we were unable to distinguish between childhood PTE (i.e., ages 0 to 18) and adulthood PTE. Similarly, our analysis of timing was restricted to PTEs that occurred more than a year ago and those that occurred within the past year. This reduced the specificity with which we could analyze the timing of exposure (e.g., exposure occurring many years prior or in childhood). Accordingly, we adopted the approach used by Behdinan et al. (2024), who similarly used the RAI-MH to assess psychiatric outcomes. Consistent with prior research (e.g., Behdinan et al., 2024; McKenna et al., 2019; Wolff & Shi, 2012), PTE was analyzed categorically. However, we acknowledge that categorization can reduce variability and may increase false-positive error rates (Thoresen, 2019). Future research should consider a more detailed assessment of PTE timing across the lifespan to better understand how temporal patterns of interpersonal PTE relate to clinical outcomes and employ continuous indices of exposure to capture cumulative severity.
Second, limitations in data collection may have affected the accuracy of self-reported information. Further, all information reported on the RAI-MH is collected during the first three days of admission, and patients’ acute stress during this period could affect their ability to provide accurate information and potentially reduce the reliability of their reports (Thomas & Wulff, 2024). It is unknown whether the reports of PTE exposure were validated by family members or documentation from other sources. Consequently, these findings should be replicated using validated reports of PTE exposure or through self-report data collection methods that ensure individuals have had time to acclimatize to the inpatient setting and are supported through trauma-informed research methods (Goldstein et al., 2024).
Third, our analyses were limited to data from participants’ first hospital admission during the study period, even for cases with more recent data. As such, our findings may differ depending on the number of admissions. Future work should examine differences in outcomes between initial and subsequent admissions to explore the longitudinal relationship between PTE exposure, symptom severity, and repeated hospitalizations, and to assess treatment effects over time. In addition, because data collection occurred only upon admission, we were unable to assess changes in psychiatric symptoms from admission to discharge. This limitation prevented us from investigating, for instance, the efficacy of treatment addressing psychiatric symptoms. Future studies that include both admission and discharge data are needed to explore whether trauma history influences treatment response or recovery trajectories. Future work could also incorporate analyses of lived experiences shared by forensic inpatients by directly exploring their perspectives on care needs, to better understand whether unique considerations exist for survivors of PTE. When education status was unknown, these cases were collapsed with the reference category to retain sample size and provide a conservative adjustment. Prior methodological work has shown that ad hoc handling of unknown covariate values in observational studies may introduce bias, and results should therefore be interpreted cautiously (Groenwold et al., 2012). Future studies with more complete data or alternative approaches to missing data are warranted.
Further, our gender analysis was also limited to comparisons between men and women due to the small number of participants identifying with other genders (n = 2). In addition, although ethnicity and culture are central to understanding PTE and psychiatric outcomes, these variables were not available in the present dataset. Data were collected across a decade, during which substantial societal and methodological shifts occurred in how ethnicity and cultural identity are conceptualized and recorded within the RAI-MH. More broadly, the RAI-MH's operationalization of PTE prioritizes discrete, individual-level events and may fail to capture forms of trauma that are particularly salient for Black, Indigenous, and other racialized individuals, including intergenerational trauma, institutional and systemic violence, and trauma related to criminalization and perpetration—limitations that are especially consequential in forensic settings where Black, Indigenous, and People Of Color (BIPOC) are disproportionately represented (Heberle et al., 2020). Accordingly, the absence of analyzable cultural data in this study reflects structural measurement constraints rather than a lack of relevance, underscoring the need for future forensic mental health research to adopt culturally responsive, trauma-informed data practices that more fully capture identity and cultural context.
Conclusion
In this study, we analyzed data on 5,105 forensic inpatients admitted to forensic hospital beds in Ontario, Canada. Our findings indicate that a history of interpersonal PTE was generally associated with positive symptoms, depressed mood, and manic symptoms, particularly among individuals exposed to polytrauma. Gender differences also emerged, such that women with a history of interpersonal PTE exhibited greater severity of aggressive behavior and depressed mood, while men showed increased depressed mood, positive symptoms and manic symptoms. Timing of PTE was also associated with symptoms, with remote exposure related to aggressive behavior in women and positive symptoms in men, and recent exposure related to manic symptoms in men. For both men and women, exposure to polytrauma was related to greater severity across all outcomes, except aggressive behavior which was not greater in men. These findings highlight the importance of gender-specific, trauma-informed approaches in forensic inpatient settings. Future research should further examine how interpersonal PTE relate to treatment and recovery to better inform risk assessment.
Supplemental Material
sj-docx-1-fmh-10.1177_14999013261435128 - Supplemental material for Interpersonal Trauma, Gender, and Psychiatric Symptom Severity: Insights from Forensic Psychiatric Inpatient Data in Ontario, Canada
Supplemental material, sj-docx-1-fmh-10.1177_14999013261435128 for Interpersonal Trauma, Gender, and Psychiatric Symptom Severity: Insights from Forensic Psychiatric Inpatient Data in Ontario, Canada by Bailey J. Thompson, Elke Ham, N. Zoe Hilton and Tisha J. Ornstein in International Journal of Forensic Mental Health
Footnotes
Acknowledgments
The authors kindly acknowledge and thank authorities of Waypoint Centre for Mental Health Care for providing source information on health data for use on this research for the year (2024–2025).
Ethical Considerations
This study received ethical approval from the Waypoint Centre for Mental Health Care Institutional Review Board (approval HPRA 24.07.29) on July 29, 2024, with a waiver of the requirement for consent based on meeting the criteria in the Tri-Council Policy Statement (TCPS 2, 2022). This is an Institutional Review Board-approved retrospective study, and all patient information was deidentified. Patient data will not be shared with third parties.
Consent to Participate
This study used secondary data obtained from the Ontario Mental Health Reporting System. In accordance with the Personal Health Information Protection Act, individual participant consent was not required.
Consent for Publication
This study used secondary, deidentified data obtained from the Ontario Mental Health Reporting System. In accordance with the Personal Health Information Protection Act, consent for publication was not required.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Positionality
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.