
Abstract
Objective
Guided by the medication literacy conceptual model, this study represents an interpretive exploration of medication literacy among patients with Chronic Obstructive Pulmonary Disease (COPD) to provide evidence for strategies aimed at improving medication adherence.
Methods
Using purposive sampling, 18 patients were recruited from the respiratory department and outpatient clinics of a tertiary general hospital in Shanxi Province between March and July 2025. Data were collected via semi-structured interviews and analyzed using directed content analysis method.
Results
The analysis yielded four primary themes: functional, communicative, and critical medication literacy, as well as medication numeracy. These findings indicate that medication literacy in COPD patients is influenced by multidimensional factors, highlighting the complex challenges and subjective barriers in both cognitive and behavioral domains.
Conclusion
These findings suggest that future interventions could prioritize patient-centered, personalized nursing interventions tailored to these specific literacy deficits—particularly in numeracy and critical processing—to effectively enhance treatment adherence and quality of life for COPD patients.
Keywords
1. Introduction
As a leading cause of chronic morbidity and mortality, COPD imposes a substantial global burden, with an annual death toll exceeding 3 million. 1 Long-term standardized pharmacological therapy is essential not only for alleviating clinical symptoms but also for reducing the frequency of acute exacerbations and delaying disease progression. 2 However, the clinical efficacy of these interventions is inextricably linked to patients’ medication literacy. Existing research 3 indicates that COPD patients generally exhibit suboptimal literacy, primarily manifested in poor inhaler techniques, low medication adherence, and deficient self-management capabilities. These deficiencies severely compromise therapeutic outcomes and the overall effectiveness of disease management.
Despite these known challenges, the underlying mechanisms and determinants of medication literacy in this population have yet to be fully elucidated, with a notable lack of in-depth qualitative exploration. To address this gap, the present study utilizes the conceptual model developed by Pantuzza et al. 4 as its theoretical foundation. This framework emphasizes the comprehensive competencies required for medication use, encompassing four dimensions—functional, communicative, and critical literacy, alongside medication numeracy—and five core sub-dimensions: accessing, understanding, evaluating, communicating, and calculating medication information. Utilizing a qualitative design, this study offers an interpretive exploration of medication literacy among COPD patients. Guided by the conceptual model, 4 the research seeks to understand how patients perceive and navigate medication-related tasks rather than assessing them against predefined criteria, thereby providing a foundation for personalized medication management strategies.
2. Subjects and methods
2.1. Study design
A qualitative descriptive study was conducted to gain an in-depth understanding of the medication literacy experiences of patients with COPD. The research employed a directed content analysis approach, framed by the medication literacy conceptual model 4 as a sensitizing framework. This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines to ensure quality and transparency
2.2. Participants and setting
Purposive sampling with a maximum variation strategy was employed. Variation was monitored across age (59–82), gender, place of residence (urban/rural), medical payment method, and duration of illness (see Table 2). Recruitment was iterative, with data analysis informing subsequent sampling to ensure thematic depth. Eligible participants were identified based on clinical criteria; subsequently, informed consent was obtained as a mandatory ethical requirement prior to data collection. The inclusion criteria were: (1) clinically diagnosed with COPD according to the 2021 Revised Edition of the COPD Diagnosis and Treatment Guidelines 5 ; (2) currently prescribed long-term medication for COPD; (3) possessing sufficient cognitive and communicative capacity to engage in a detailed interview. Exclusion criteria involved patients with psychiatric disorders, malignant tumors, or severe uncompensated organ dysfunction (e.g., advanced heart or renal failure).
2.3. The research team and reflexivity
To ensure the credibility of the findings, the research team consisted of two graduate students trained in qualitative methods and one senior clinical expert in respiratory care. The interviewers established rapport with participants through prior clinical interactions, yet maintained reflexivity by keeping a reflective journal to minimize personal bias and ensure linguistic neutrality during sessions.
2.4. Data collection
A semi-structured interview guide was developed based on the four dimensions of the Pantuzza model. Pilot interviews were conducted with two participants to refine the phrasing of questions (data excluded from the final analysis).
Final interviews were conducted in private, quiet rooms to ensure confidentiality. Each session lasted 30–40 minutes and was audio-recorded with permission. Field notes were taken to document non-verbal cues. Data saturation was determined when no new themes or conceptual categories emerged from three consecutive interviews; informational redundancy was achieved after the 18th participant. The general characteristics of the interviewees are presented in Table 2 of Appendix A.
2.5. Data analysis and rigor
Directed content analysis 6 was performed iteratively using NVivo 12.0. A hybrid deductive-inductive approach was used: initial codes were derived from the model, 4 while novel patterns were subsumed into relevant dimensions to maintain coherence.
2.5.1. To ensure trustworthiness (rigor)
Credibility: Member checking was performed by sharing transcripts and preliminary themes with participants for verification.
Dependability &Confirmability: Two researchers independently coded data to ensure rigor. Discrepancies were resolved via consensus or a third party to minimize researcher bias.
2.6. Ethical considerations
The study protocol was approved by the Medical Ethics Committee of the First Hospital of Shanxi Medical University (KYLL-2025-211). All participants provided written informed consent and were assured of their right to withdraw at any time. All data were anonymized (P1–P18) to protect privacy.
3. Results
Themes and sub-themes of medication literacy among COPD patients (based on Pantuzza model).
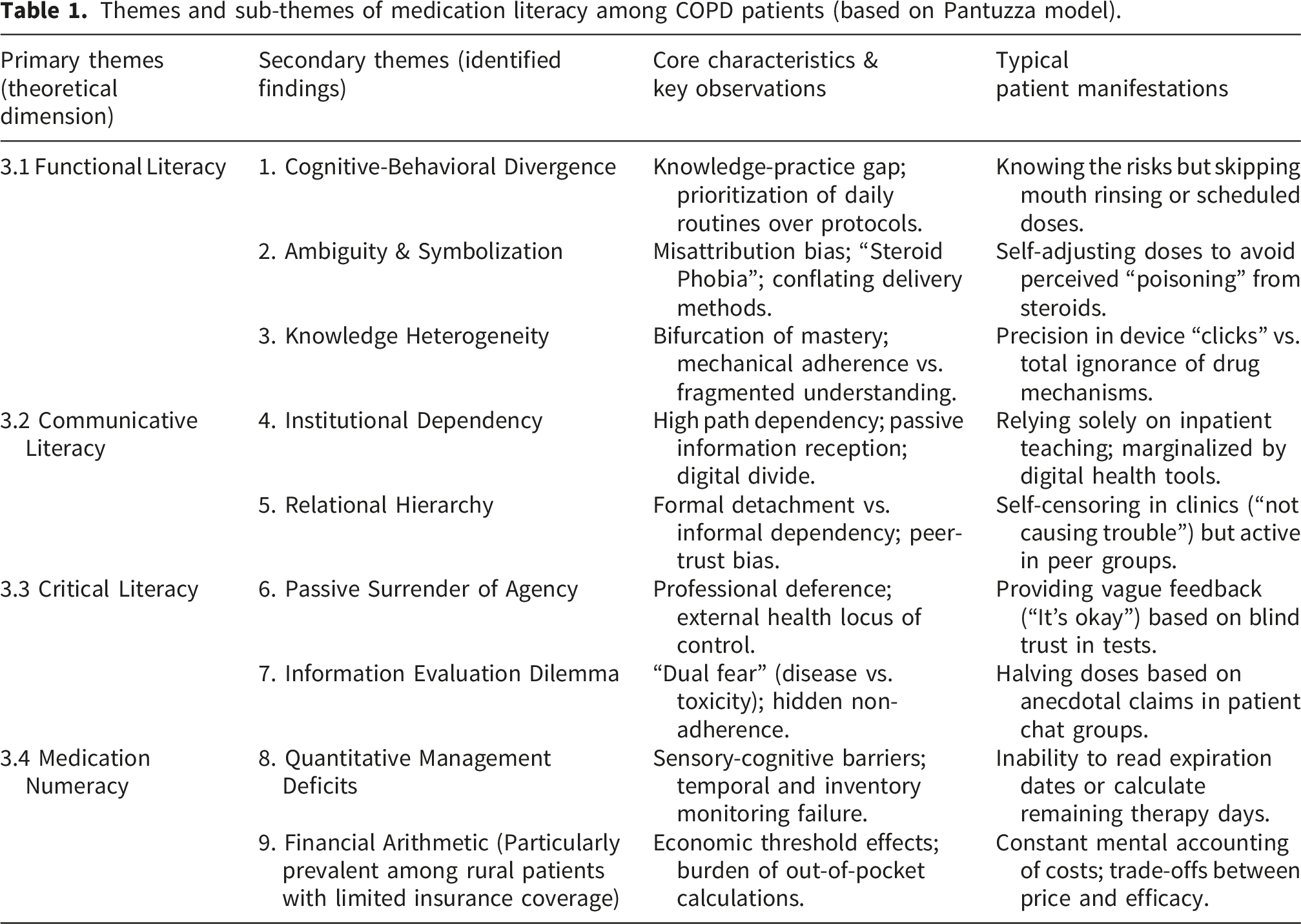
3.1. Theme1: Functional medication literacy
3.1.1. The gap between knowledge and action: “Knowing but not doing”
A “knowledge-practice gap” was evident; participants prioritized life routines over preventive protocols despite awareness of risks.
P1 (Male, 62y): “I usually don’t rinse my mouth... even though I’ve heard it can lead to oral infections.”
P2 (Male, 58y): “I only use it as a ‘pre-work boost’... when I have tasks to complete.”
P7 (Female, 65y): “I thought I could finish chores first... halfway through, I was struggling to breathe.”
3.1.2. Ambiguity and “steroid phobia”
Cognitive biases led to the “symbolization” of side effects, where patients conflated inhaled therapy with systemic steroids to rationalize non-adherence.
P5 (M, 71y): “I feel unwell after using it... this medicine just doesn’t ‘agree’ with my constitution.”
P8 (M, 66y): “It contains steroids... I’ll only use it as a last resort.”
3.1.3. Knowledge heterogeneity
Literacy levels showed a “bifurcation.” While patients with longer disease durations demonstrated high technical proficiency in device operation (the “clicks”), they often lacked a fundamental understanding of the underlying mechanisms, leading to mechanical rather than informed adherence.
P3 (M, 60y): “You must listen for that ‘click’... then inhale forcefully and quickly.”
P14 (M, 74y): “I focus on the ‘what’ and ‘how much’... the underlying mechanism? I’m in the dark.”
P15 (M, 69y): “I feel my inspiratory flow is too weak... I don’t know if it actually went in.”
3.2. Theme2: Communicative medication literacy
3.2.1. Institutional dependency and digital divide
Older participants, particularly those from rural areas, exhibited high “path dependency” on clinical staff. Their marginalization by digital health technology was compounded by both age-related sensory decline and limited infrastructure in rural settings. P9 (Male, 72y): “Precautions were filtered through medical staff. I don’t seek information elsewhere.”
P15 (Male, 69y): “I’m at a loss with smartphones... I’m entirely dependent on doctors or my children.”
3.2.2. Trusting close ties over professionals: “Informal peer support”
A paradox of “formal detachment and informal dependency” emerged, where social proximity dictated information flow over professional expertise.
P5 (Male, 71y): “I only answer what’s asked... I don’t want to be a ‘troublesome’ patient.”
P18 (Male, 68y): “My neighbor has the same condition. We compare notes... I could never ask doctors that.”
3.3. Theme3: Critical medication literacy
3.3.1. Blind trust and relinquished responsibility: “Leaving it all to the doctor”
This passive stance was more pronounced among participants living with supportive children or spouses, where the delegation of health responsibility to both family and physicians reduced the patient’s perceived need for personal agency.
P5 (Male, 71y): “I just say ‘it’s okay’... I feel the doctor knows everything through the tests.”
P11 (F, 67y): “My breathing felt tighter, but I figured if the medicine wasn’t working, the doctor would have seen it in my records... It’s not my place to guess.”
3.3.2. Dilemmas in evaluation
An interpretive theme of ‘Dual Fear’ emerged from the data, reflecting participants’ descriptions of being ‘caught between two fires. Conflicting information created a “dual fear” of disease vs. toxicity, leading to hidden, self-directed dose adjustments.
P4 (Male, 73y): “Doesn’t that poison just accumulate in your system over ten years?”
P15 (Male, 69y): “In patient groups, they say steroids cause bone loss... I halved my dose. If I don’t bring it up, the doctor won’t know.”
3.4. Theme4: Medication numeracy
3.4.1. Struggling with numbers and time: “The burden of tracking”
Sensory decline and cognitive load hindered the interpretation of temporal data and inventory estimation.
P3 (Male, 60y): “My eyesight’s gone... I can’t decipher the tiny numbers [on expiration dates].”
P16 (Female, 72y): “The doctor asks how many days are left, and I freeze. I can’t figure it out.”
3.4.2. The Arithmetic of affordability
Financial arithmetic was a dominant barrier for participants with the New Rural Cooperative Medical Scheme (NCMS) or those who were self-funded. For these individuals, medication management was filtered through a lens of “economic survival,” balancing drug costs against fixed household budgets.
P17 (Male, 70y): “It costs 500 yuan... even with insurance, I pay 200. That’s a significant monthly hurdle.”
P18 (Male, 68y): “Each session costs tens of yuan... I’m constantly doing the math, wondering if I can afford it.”
4. Discussion
4.1. Bridging the knowledge-practice gap: From “knowing” to “competent doing”
This study reveals a pervasive “cognitive-behavioral divergence” among COPD patients, echoing global findings on the “knowledge-practice gap” in chronic care.7–9 While patients possess a baseline awareness of treatment necessity, their functional literacy is compromised by a “bifurcation of competence”: a minority achieve technical mastery, while the majority rely on fragmented, mechanical adherence. This confirms that functional medication literacy is the rate-limiting step for effective administration. 10
To bridge this gap, interventions might transcend didactic information delivery. We advocate for the systematic implementation of the Teach-back method. 11 Unlike passive listening, this feedback-loop approach allows clinicians to validate comprehension and correct inhaler technique in real-time, effectively transforming patients from passive recipients into competent practitioners. Furthermore, addressing the psychological barriers is crucial. These barriers include illness-related stigma, social withdrawal, and catastrophic cognition regarding dyspnea, which often lead to deliberate avoidance of medication information and decreased treatment compliance. 10 To mitigate these, Mindfulness-Based Stress Reduction (MBSR) could be considered for integration. Specifically, techniques such as mindful breathing and body scanning can be utilized to reduce sympathetic nervous system arousal triggered by anxiety. By decreasing breathing frequency and correcting the catastrophic perception of breathlessness, these interventions enhance patients’ emotional self-regulation and self-efficacy, ultimately facilitating the translation of medication knowledge into sustained health behaviors.12,13
4.2. Overcoming information poverty: Digital inclusion and social capital transformation
Our findings highlight a critical state of “information poverty” driven by the digital divide. Consistent with Peng et al., 14 elderly patients’ limited eHealth literacy creates a structural barrier to evidence-based resources. Consequently, patients exhibit a “hierarchical trust pattern,” prioritizing the emotional proximity of “lay referral networks” (family and peers) over professional expertise. While this provides emotional buffering, it introduces significant risks of information distortion and scientific inaccuracy. 15
Addressing this requires a two-pronged strategy. First, healthcare systems could adopt an “age-friendly” design philosophy. Complex pharmaceutical data should be converted into multimodal formats (e.g., infographics, voice-activated reminders) to lower cognitive entry barriers.16–18 Second, strategic leverage of social capital may play a crucial role. Recent qualitative evidence suggests that close connections within family and social networks serve as a primary driver for sustained health management in COPD patients. 19 For instance, patients often derive motivation from their desire to support working children or maintain their roles within the family, while professional guidance embedded in these trusted circles transforms family members into ‘reinforcing agents’ who filter information and supervise medication adherence. 20 This approach shifts the family’s role from a potential source of misinformation to a structured support system that buffers the psychological burden of chronic care. 21
4.3. Rectifying maladaptive agency: From “steroid phobia” to rational decision-making
A profound deficit in critical medication literacy was observed, characterized by low self-efficacy and a reliance on external directives. Paradoxically, when patients did attempt to exercise agency, it often resulted in “maladaptive self-regulation.” Overwhelmed by fragmented information and “steroid phobia”,8,22 patients frequently engaged in unauthorized dose reductions—a behavior they perceived as “proactive risk avoidance” but was fundamentally a dangerous deviation rooted in flawed risk assessment. This aligns with O'Toole et al. , who noted that patients often overestimate drug toxicity while underestimating disease progression. 23
To correct these cognitive distortions, care models could shift from “compliance” to “empowerment.” We recommend self-efficacy-enhancing nursing strategies 24 that utilize motivational interviewing to help patients internalize the rationale for maintenance therapy. Crucially, multidisciplinary collaboration is highly recommended. Pharmacists should be integrated to provide visual, scientific demonstrations that demystify the mechanisms of corticosteroids, transitioning patients from “blind obedience” or “hidden non-adherence” to informed shared decision-making. 12
4.4. Systemic support for management capacity: Mitigating financial and cognitive burdens
Regarding medication numeracy, challenges in the Chinese context are distinct: they center less on complex dosage calculations and more on inventory awareness and temporal monitoring (e.g., expiration dates). Consistent with Zhao et al. , sensory deficits in the elderly exacerbate these management failures. This calls for geriatric-optimized packaging designs (e.g., large-font expiration tags) to reduce cognitive friction. 25
Financially, the “economic arithmetic” of chronic care remains a potent barrier. As noted in Results 3.4.2, “financial toxicity” often forces a trade-off between adherence and household stability. While the State Council’s medical reform policies provide a strategic framework, clinical practice might bridge the “last mile.” Healthcare providers might find it beneficial to implement longitudinal follow-up mechanisms that not only monitor clinical indicators but also assess patients’ “economic resilience” and inventory management capacity, ensuring that policy benefits effectively translate into sustained adherence behaviors. 26
4.5. Limitations
Several limitations warrant consideration when interpreting the findings of this study.
First, the study was conducted at a single tertiary hospital in Shanxi Province using purposive sampling. While this strategy provided rich, in-depth data, the participants may possess higher health awareness or better access to medical resources compared to patients in primary care or rural settings, potentially limiting the transferability of the findings to diverse socioeconomic contexts.
Second, the exclusion of patients with severe cognitive impairments or communication deficits means the study may have inadvertently captured the perspectives of a relatively “more literate” cohort, potentially leading to an underestimation of the severity of literacy deficits in the broader COPD population (selection bias).
Third, the cross-sectional qualitative design provides only a static “snapshot” of medication literacy. It fails to capture the dynamic evolution of literacy as the disease progresses or as cognitive function declines over time.
Finally, as data were collected through face-to-face interviews, response bias—specifically social desirability bias—cannot be entirely ruled out, as participants might have understated their non-adherence to project a “good patient” persona despite the interviewers’ efforts to maintain neutrality. Future research should employ multi-center, longitudinal mixed-methods designs to validate these findings and explore the trajectory of medication literacy throughout the disease course.
5. Conclusion
Grounded in the medication literacy conceptual model, this study elucidates the multi-dimensional nature of medication literacy among patients with COPD, revealing a complex interplay of functional, communicative, and critical experiences. The findings highlight how contextual barriers and subjective perceptions shape medication-taking behaviors, particularly the patterns of ‘passive adherence’ and ‘maladaptive self-regulation.’ These insights offer potential directions for clinical practice to explore transitions from didactic instruction toward more empowerment-based support. Furthermore, healthcare systems might consider enhancing digital literacy for elderly patients to improve information accessibility, while leveraging trusted social circles to foster informed decision-making. Given the single-center design, future research is warranted to further evaluate the efficacy of these literacy-sensitive strategies across diverse COPD populations.
Footnotes
Acknowledgements
We would like to thank research group for their valuable time. We would also like to thank the expert researchers who helped us by evaluating the coding, interview form and content-theme fit of the study.
Ethical considerations
The study had finished the ethical approval by the Medical Ethics Committee of the First Hospital of Shanxi Medical University (Approval No.: KYLL-2025-211).
Consent to participate
The study adhered to the Declaration of Helsinki, had obtained informed consent from all participants before the investigation began.
Author contributions
ZJH: Writing – original draft, Writing – review & editing, Interview Results Compilation and Analysis, Project administration. LJQ: Conduct an interview, Interview Results Compilation. ZY: transcript of interview results. ZRN: Transcript of interview results. GH: Interview Results Analysis.SXQ: Interview Results Analysis.YYP:Methodology, Writing –review & editing.SLP: Analysis of qualitative interview results, Project administration, Resources, Writing-review & editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sets created and/or analyzed during the current study are not publicly available for the aim of protecting informed consent and maintaining confidentiality, but may be obtained from the corresponding author upon reasonable request. All information obtained as a result of the analyses in the study is presented in this paper.