
Abstract
The aim of this study was to give an in-depth consideration of the chronic obstructive pulmonary disease (COPD) patients’ subjective view of the impact of pulmonary rehabilitation (PR) on their lives. A systematic review in PubMed, Embase, CINAHL and PsychInfo databases yielded 3306 articles, of which 387 were duplicates, 263 remained after screening abstract and title; of them, 4 were excluded (editorial or due to lacking of full text) remaining a total of 259 for full text reading. Among these, eight studies met the inclusion criteria and were finally included. The meta-ethnography approach synthesized an understanding of the studies, which focused on constructing interpretations and developed a ‘line-of-argument’ synthesis. The psychosocial support of PR contributes to the patients’ strength and desire for participation and the health education leads to illness-perception learning. Both psychosocial support and health education develop patients’ empowerment, while PR promotes opportunities to health transitions. The empowerment experienced by the patients in taking advantage of these opportunities leads to positive impacts over time. If they do not exploit these occasions, negative impacts arise in their life, which make the treatment assistance or follow-up more difficult. The COPD patients’ feedback revealed that PR promotes a better ‘way of life’, well-being and important behavioural changes towards health promotion.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) progressively affects patients by causing physical constraints, psychosocial disturbances and an economic burden. 1 –5 Therapeutic options are centred on smoking cessation, pharmacologic therapies and other treatments such as rehabilitation, oxygen therapy, ventilatory support and surgical treatments. 2 Pulmonary rehabilitation (PR) programme is a multidisciplinary and structured intervention to optimize the physical and social functioning of patients with chronic respiratory impairment. 6 It can be applied to inpatient, 7 outpatient 8 or home environments. 9 Duration, frequency of sessions and protocols differ according to the health-care professional team, setting and resources available, 7 –9 and the minimum length of an effective PR programme is 6 weeks. 2 Its principal components are exercise training, which is considered the cornerstone of PR, education and psychosocial support. 6 Elements of education and, in particular, self-management, substantially reduce hospitalization, emergency department and unscheduled physician visits among patients at risk. 10 Psychological support in a PR reduces incapacity, anxiety and depression in large groups of patients suffering from these symptoms. 11 Integration of occupational therapy can improve independence in activity, while nutritional intervention should be considered for underweight patients or those with body composition abnormalities. 12 Reduced dyspnoea sensation, improvements in exercise tolerance and quality of life (QoL) in COPD patients are some of the positive impacts of PR programmes. 6,8,9
Despite the fact that these impacts have been well evaluated and established in quantitative studies, 8,9,13,14 the overall understanding of PR and the psychosocial problems generated by this chronic illness from the patients’ perspective are limited. The benefits, difficulties or barriers of treatment as understood or perceived by the participants during and/or after treatment, as well as their opinions about the intervention, have been only scantly examined. 15 –22 A systematic synthesis of qualitative studies about COPD and PR may provide additional knowledge, which has not been revealed by a single study, by identifying common recurrent themes. This understanding of the experiences of COPD patients provides relevant information for health professionals, family members and/or caregivers, who must deal with those patients. It will help them to better understand the patients’ needs and expectations and concerns to give support for better treatment and care. Consequently, adjusting the COPD treatment according to the patients’ constraints and needs may contribute to their adherence to PR programmes. 16 Qualitative studies with COPD and PR may complement quantitative findings as quantitative research tries to explain the nature and strength of associations or relationships; qualitative studies also tend to develop an ever-widening explanation. 23 Qualitative studies have a specific methodology that, when applied properly, is a promising method to provide understanding of clinical settings. 24 Qualitative methods 25 –27 permit the exploration of patients’ lived experiences – their perspectives, beliefs and feelings – disclosing subtle details and meanings not identified using quantitative methods alone. In fact, a combination of both qualitative and quantitative research in a mixed methods study often offers the most comprehensive approach. 28
Thus, the aim of this systematic review is to provide in-depth consideration for the subjective view of COPD patients on the impact of PR on their lives, exploring the lived experiences and identifying the benefits, negative and positive aspects perceived during and/or after participation in PR programmes.
Methods
Search strategy
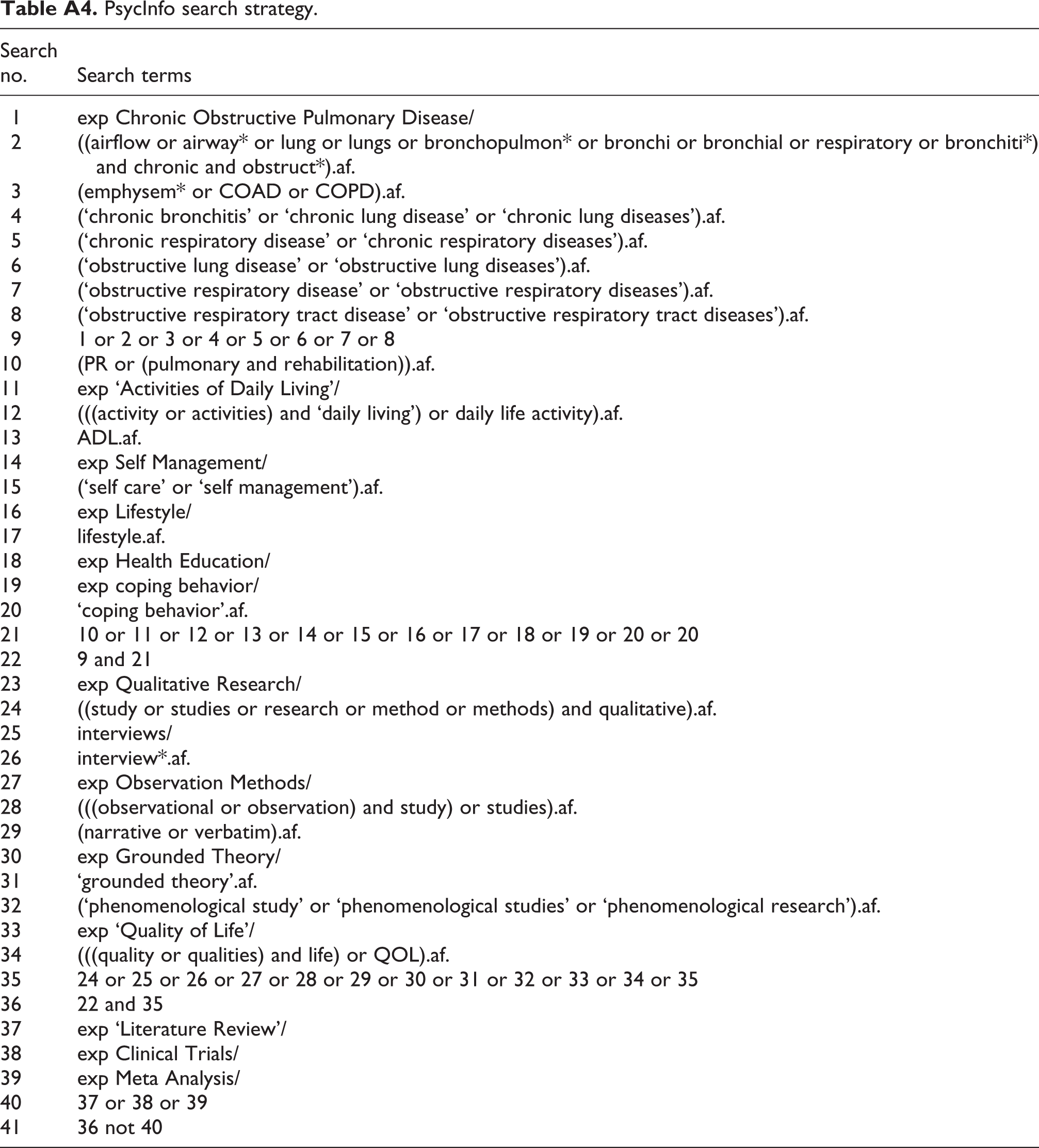
The search process was performed in PubMed, Embase, CINAHL and PsychInfo electronic databases from December 2011 to January 2012 using specific search strategies specified in the Appendix Tables A1–A4. Two reviewers (JMSP and AMN-N) conducted an independent title and abstract screening followed by an agreement reached between them on the selection of studies. Reviewers JMSP, AMM-N, MTAPM and TEPMM carried out the full text reading to identify articles to be included in the review.
Inclusion criteria
We included studies that described the COPD patient’s experiences with PR – positive or not – related to the programme itself as well as to participant’s feelings and behavioural changes. The studies had to meet the following criteria: (1) articles using a qualitative methodology according to the existing guidelines 24 that report qualitative research only (using typical research methods such as interviews, focus groups or participant observation) or research using a mixed method (qualitative and quantitative methods) that describes qualitative findings (in this case, just qualitative findings were analyzed), (2) group of participants formed only by COPD patients or that included patients with COPD (in this case, just COPD patients’ reports were analyzed), (3) studies that applied any kind of PR (outpatient or hospital-based) and (4) articles published in English, Spanish or Portuguese. Both articles for which the full text was not obtained and editorials were excluded.
Methodology assessment
To assess the methodological characteristics of all the articles, a previous modified checklist 29 was used based on the content of the qualitative methodology, in order to get a methodological overview of the studies. This analysis allowed for a description of the research quality of all the articles. The assessment was conducted independently by three reviewers (JMSP, MTAPM and TEPMM) and any differences were solved by discussion and consensus.
Article analysis
Three reviewers (JMSP, MTPM and TEPMM) independently analyzed the article; discussions were necessary in order to define final results. The meta-ethnography approach, originally described by Noblit and Nare, 30 was used as it is a well-developed method for synthesizing qualitative data in small groups of articles that are closely related. 31 It is based on the interpretive paradigm and synthesizes an understanding of the studies focused on constructing interpretations – not analyses. This approach provides an alternative to traditional aggregative methods of synthesis 32 and includes the following phases: (1) getting started (identifying the subject to be investigated), (2) deciding what is relevant to the initial interest, (3) reading the studies, (4) determining how the studies are related, (5) translating the studies into one another, (6) synthesizing translations and (7) expressing the synthesis. 30
Following this approach, lists summarizing the authors’ original finding, using their concepts and terms, were drawn up for each article. These summaries were abstracted from the appraisal sheets that had been prepared for each article. At the bottom of each list, key concepts were identified. The lists were drawn up by hand, on a long piece of paper, so that they could be easily compared with relationships between concepts in the different studies indicated by arrows and lines. Having identified the main concepts to emerge from each article (primary and secondary themes), a systematic search was undertaken for the presence or absence of these concepts in all the articles to be synthesized. The primary themes are identified from participants’ understanding presented in the Results section of the articles, and the secondary themes are derived from authors’ interpretations presented in the Discussion section of the articles. Primary and secondary themes influenced our approach towards the ‘themes’ (third-order interpretation).
Based on the translated themes, we developed a ‘line-of-argument’ synthesis, 30 which was the most appropriate to depict our understanding of the COPD patients’ experience with PR. The ‘line-of-argument’ is the construction of an interpretation that reveals what is hidden in individualized studies, discovering a whole among a set of parts. 30
Results
The systematic literature search yielded 3306 articles, of which 387 were duplicates, leaving 2919. After screening the title and the abstract, 263 articles remained; of them, 4 were excluded (editorial or lacking of full text), leaving a total of 259 remaining for full text reading. Among these, eight studies met the inclusion criteria and were finally included in the review (Figure 1).

Search process of the systematic review.
Studies description
Of the eight articles, 15 –22 the total number of participants in the studies was 106 (men and women) with ages ranging from 45 to 86 years. The samples were composed of COPD patients, with the exception of one study, 20 which included two patients with bronchiectasis also along with COPD. Just three articles specified COPD severity. 18,20,22 Investigations were conducted in four different countries: five from the United Kingdom, 16,18-20,22 one from the United States, 15 one from Canada 17 and one from Norway. 21 Patients were researched between 6 and 11 months after completing their PR, 15 within 2 weeks of the post-rehabilitation, 17 before and after the PR programme, 18 or within 2 months after the programme and during a follow-up interview (1 year later). 22 Participants in the studies were those who attended the PR over the previous 2 years of the study, 16 patients who attended PR within the 4 months prior to the data collection, 19 patients who were either on the maintenance programme or who had recently (within the 4 months) completed it. 20 Five articles used semi-structured interviews, 15 –18,22 one used an interview without specification, 21 two used focus groups 19,20 and one used participant observation associated with a semi-structured interview. 22 More characteristics of the studies included in the review are detailed in Table 1.
Characteristics of the studies included in the systematic review.

COPD: chronic obstructive pulmonary disease.
Characteristics of the studies’ methodology
The application of the checklist about the studies’ methodology revealed that all data were transcribed verbatim; the articles described how research themes were identified, presented quotations from the data and reported an ethical review of the study. Predefined questions were used in most interview studies. 15 –18,21,22 One 19 of the two studies using focus groups applied a trained facilitator. In the majority of the studies, the saturation of themes was not reported. 15,17,18,20,21 In almost all of them, 15 –17,19,22 findings were analyzed in duplicate and one 21 mentioned whether member checks had occurred. All characteristics of the studies’ methodologies can be seen in Table 2.
Characteristics of the studies methodology.
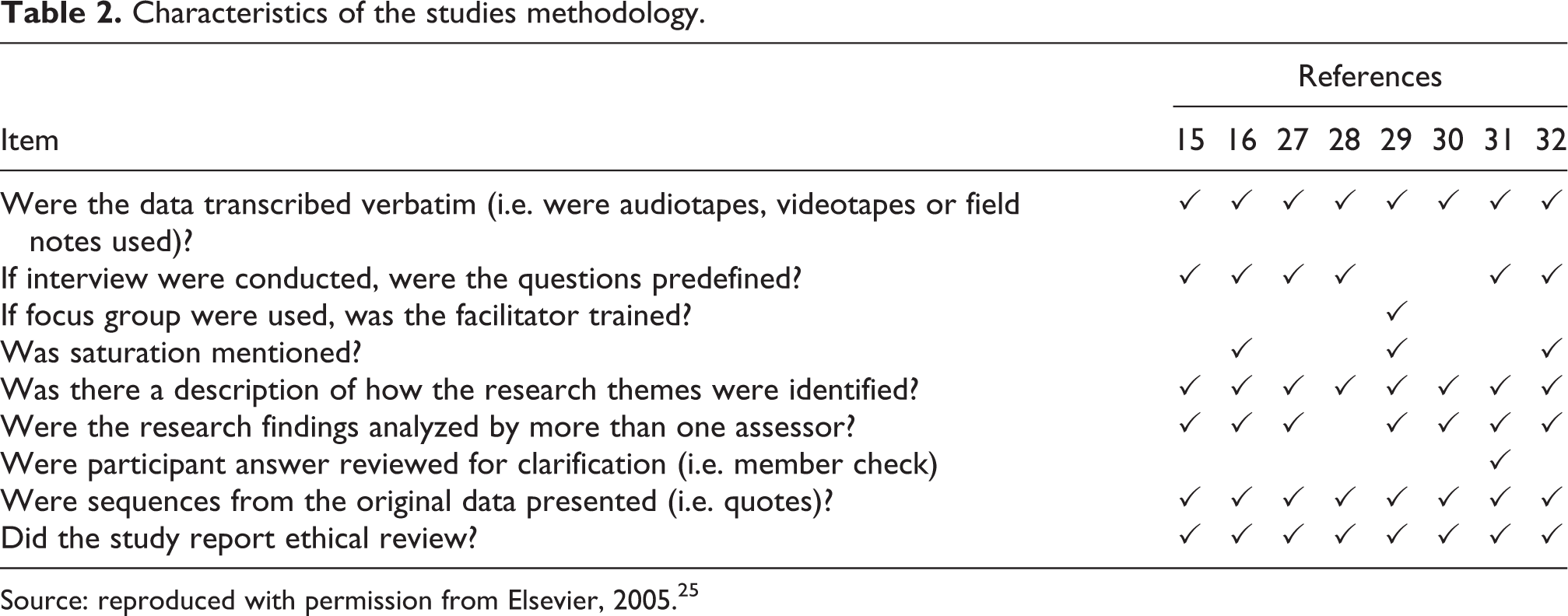
Source: reproduced with permission from Elsevier, 2005. 25
Description of themes
Five primary themes and four secondary themes were identified. From those, five third-order interpretations were defined as ‘themes’ (Table 3): (1) support during the PR, (2) learning process through education sessions, (3) the opportunity for health transition, (4) barriers, difficulties and negative points and (5) the benefits of the PR.
Synthesis including themes, primary themes and secondary themes.

COPD: chronic obstructive pulmonary disease; PR: pulmonary rehabilitation; QoL: quality of life.
Support during PR
The COPD patients identify three scopes of support: health professionals, peer groups and family. 15,16,18 –21 The multidisciplinary team of most programmes stimulates and encourages patients to achieve a new goal of exercise and self-management. The safe and motivating environment of the programmes, social encounters and group sessions with peers also encourage participants as well as family assistance. 15,16,18 –21
The health professionals supervise patients’ performance through close monitoring, giving them positive reinforcement and encouragement, which is the basis of the learning process; 15 they also motivate patients to continue exercising at home. The staff provide feedback regarding the progress of patient activities, which is ‘painfully slow’, increasing patients’ self-confidence; they stimulate participants to continue with the treatment and identify their own limits. 15,19 This feedback characterizes a clear professional–patient communication, which restores patients’ confidence, as a patient reports: ‘Having someone persisting, cheerfully encouraging me to go on and do it, you know, I began to feel, “I can do that.” And that was the feeling of confidence, increasing feeling of strength’. 15 The health professional support influences the patient’s capacity to recognize health improvements.
Some participants had never met anyone else with COPD before initiating PR: ‘Up until then I hadn’t met anyone else with it, you think you are the only one’. 16 Consequently, the peer group psychologically helps them as they meet new people with the same conditions and problems. 16,18,19 The group support also provides ‘encouragement’, ‘motivation’ and ‘social times’ through which participants increase socialization. 16,18 One patient remembers: ‘It was lovely and we got on well, … and I used to look forward to meeting them and telling a few jokes and making them laugh, you know’. 18 Peer support builds up companionship; patients share their problems, experiences and histories of health and illness. 19 They do not feel alone or isolated anymore. 20 ‘Useful talks’ 19 make it possible for participants to express their feelings and opinions with no recrimination or judgment; conversations with peers are strengthened throughout the sessions. 21 In addition to the staff and peer support, in one study, 19 the patients’ family support during rehabilitation was enhanced: ‘I mean my wife sometimes comes and has a coffee while I have it you know what I mean but at least she makes sure, she says “I know you’re going then,” you know’. 19
Learning process through education sessions
Five of the eight articles 15,17,19,21,22 showed that education sessions are significant part of PR. In general, the sessions included illness management: breathlessness control, breathing exercises, practical tips, COPD information and use of medication and medical devices. 15,17,19,21,22 One patient explains his learning about medication: ‘I learned that Ventolin takes effect in five minutes or so, and the other one, Atrovent, it doesn’t start working for about 15 minutes … [Now I’m] leaving a little more time between taking the puffers … ’. 17 COPD patients affirm they use some energy conservation strategies taught, such as coordinating breathing with stair climbing, organizing the environment (such as stocking closets with seasonal clothes only), pacing meal preparation, sitting to rest during or between activities, arriving early for appointments, seeking help and so on. 15
Participants also learned to overcome inactivity by healthier routines and habits to carry out the exercise protocols and breathing strategies. Allison increased her use of the treadmill, which is nowadays a daily priority for her: ‘I go downstairs every day to do the treadmill … I never miss the treadmill, to me, that’s top priority’.
15
Peter is also well disciplined to exercise every day, comparing its importance with others daily-life activities: It’s like I get up, I brush my teeth, I get dressed and I get on the treadmill before I even go downstairs … I know if I’m going to do it, I’ve got to get into a routine – a routine that’s comfortable, that’s going to work for me – and then stick to it.
15
Patients got a new life through the education sessions. ‘Practical tips’ were included in daily activities, as Mrs M states: It’s fantastic because you have the practical exercise and then you have the education, and that is as important because I knew nothing about it [COPD] until then and I learned so much and how to cope. […] they tell you: “Don’t use a towel, use a toweling dressing gown,” it’s fantastic, it’s such a simple thing and you think: “Well, am I stupid that I didn’t think of that?”.
22
Simple orientations guided the patients to cope with their limitations.
The opportunity for health transition
Patients recognize PR as an opportunity for changes in their lives; some of them accept it as a new acquisition for their ‘life plan.’ Others modify habits or restructure the way they notice their current health condition by reorganizing future plans. 15 –18,21,22 Before even starting sessions, PR programmes 16 promote the opportunity for patients to ‘get out of home’ and help themselves; as one participant affirms: ‘…giving me the opportunity to help myself and do something positive instead of just taking this, taking that [medication]’. 16 It is an opportunity to take some ‘control’ of their functional status. At the time patients initiate PR, they have a chance to meet ‘new people’ – other COPD patients – and insert themselves in a social context. 16,18 Consequently, this is an opportunity for improving their health and well-being; it is a chance to start the process of disease self-management. 21 PR programmes also promote reflection about the individuals’ personal conditions 21 involving chronic and progressive lung disease.
Experiencing PR offers future challenges to participants; they are ‘hopeful’ of health and future, of maintaining ‘controlled breathing skills, increased activity tolerance and walking endurance’ through follow-up rehabilitation. They recognize the power and progress acquired with the programme what encourage them, as Peter reports, to fight for conquest: It’s like you’re fighting uphill all the way. But I feel hopeful because I feel that in spite of that, I have made some progress … It’s like when you’re as stricken as this, you want as much as possible available to try if it’s there.
15
One patient emphasized her return to a dancing group with a friend as a new goal for the near future: We’re gonna have a go at line dancing, at Christmas, well we’re gonna start in the winter, I’m gonna go, [husband] will take us and we’re gonna go around at the school and have a go at line dancing so that will be my dancing debut.
18
Education sessions give a chance for a new ‘way of life’ to COPD patients, who assume different behaviours and routine adjustments. 15,17,21
The benefits of PR
All the reviewed articles 15 –22 describe PR benefits in the physical and psychosocial dimensions of the patients’ life. Participants experience increased physical ability and decline assistance for certain tasks once they have more confidence; they have more energy for outdoor activities and experience less breathlessness. 15,16,19 The participants notice health improvements in their overall physical and emotional well-being. 20,21 Their ability to control symptoms avoids the need for emergency attention; 16,17,19,21 they are more sociable persons, regain their family role 18 and recognize better QoL. 21
Improvement of physical ability was clearly described as a relevant gain after the programme.
18,20
Enhanced physical mobility and the ability to work around the house were identified as the principal benefit of physical activity. One patient reports increasing the level of mobility as compared to their past condition: but now I walk … I go all the way around the village and come in the other side, which takes me about 20 minutes, so it’s a 20 minute walk I have every day, which is something I never used to do before.
18
Benefits with household-related activities, both inside the house and in the garden, changed individuals’ dependency on family members.
18
Activities requiring physical effort, which the patients had stopped performing, now form part of their routine as one patient affirms: …definitely doing more than I was … I mean before that I hadn’t cut the grass for two years, my wife was doing it, I must admit I’m not doing it all the time now but I will go out and have a little bit of a go.
18
In a psychological dimension, patients gain confidence, self-esteem and a better mood; some regain a positive self-image and self-surveillance, and others are hopeful for the future despite having a chronic illness. 15 –22 One patient acknowledges that PR is responsible for their psychological change: ‘I think psychologically I got really low without realizing it … it [PR] was a real turning point…I improved 100% in being able to get around’. 16 The ability to cope with the limitations of COPD enhanced their ‘control’ and ‘management.’ Feelings of ‘fear’ and ‘frustration’ were replaced with those of ‘safety’ and ‘confidence,’ as two patients affirm: ‘You can understand it, so you can cope;’ 19 ‘It [PR] gives you confidence to do things.’ 20 Patients notice fewer infections and less medication 19,20 with considerable improvements in general health.
Barriers, difficulties and negative points
Although all reviewed articles described the PR benefits, in half of them, 16,19,21,22 some patients also identify barriers and difficulties that are related to PR access, professional–patient relationship, education sessions and psychological affectation. Transport and parking difficulties are inconveniences for participating in PR, although they do not directly affect participants’ adherence 16 to the programme, which may occur to those who become housebound due to problems with breathlessness. 22 The lack of push or encouragement during the sessions was the reason for one patient to drop out the programme: ‘Being on my own there is no one to give me a bit of a push or encouragement.’ 16 She acknowledged, however, that this happened as a result of her isolation in the group. The day of the sessions is a barrier for one patient to participate as he uses that particular day to go to a community course, which he cannot miss: ‘I would do it but not on Fridays ’cause I go to a community course. It’s great, we really enjoy it so I’m not going to miss that’. 16
Even though many patients recognized the support received in the PR as stimulated and motivated, others consider the ‘lack of support’ after PR to be an obstacle to the follow-up. Some COPD patients express a need for continued professional support after rehabilitation as this period provides a ‘temporal security and support’ and after that it is a ‘period of uncertainty and vulnerability’. 21 Another patient defines the end of the programme as ‘the end of any formal support’: ‘You’ve had somebody sort of caring for you for six weeks and then being interested in you and then it’s just gone you know’. 19 To adjust to this point, the same patient suggests extra classes at the community hospital when the PR finishes: ‘It would be nice to have a class to come to every week, I think it would help everyone’. 19 During a focus group in the same study, 19 several patients negatively classify the programme as short: ‘I don’t think that six weeks is long enough I don’t, it ought to be a bit longer’. 19 Another patient points out the lack of comprehensive instructions for inhalers, counselling services to overcome psychological problems and clear written material: ‘But I do find leaflets, what you’ve been given here or there, they’re not exactly in plain English and they do take a lot of understanding, you think what’s that word mean you know’. 19 Some patients do not appreciate working in groups as comparing themselves with more severely ill persons may unleash a fear of becoming more severely disabled. 21
The ‘line-of-argument’ description
The psychosocial support given to the COPD patients by the health professionals, peer groups and family during PR favourably contributes towards their strength, desire and motivation to be involved in PR. The health education associated with this support leads to a learning process, which provides knowledge and consciousness of the illness perception, including symptoms and progress, to the patients. Both psychosocial support and health education work together in PR treatment to contribute towards the development of patients’ empowerment. On the other hand, the PR itself promotes opportunities for health transitions in the patients’ life. So, if the COPD patients apply this developed empowerment to those opportunities, they achieve and perceive positive impacts over time. If they do not get physically and psychologically involved in this process of treatment and changes, negative impacts arise during the intervention, which makes their assistance or follow-up treatment more difficult. The ‘line-of-argument’ is represented in Figure 2.
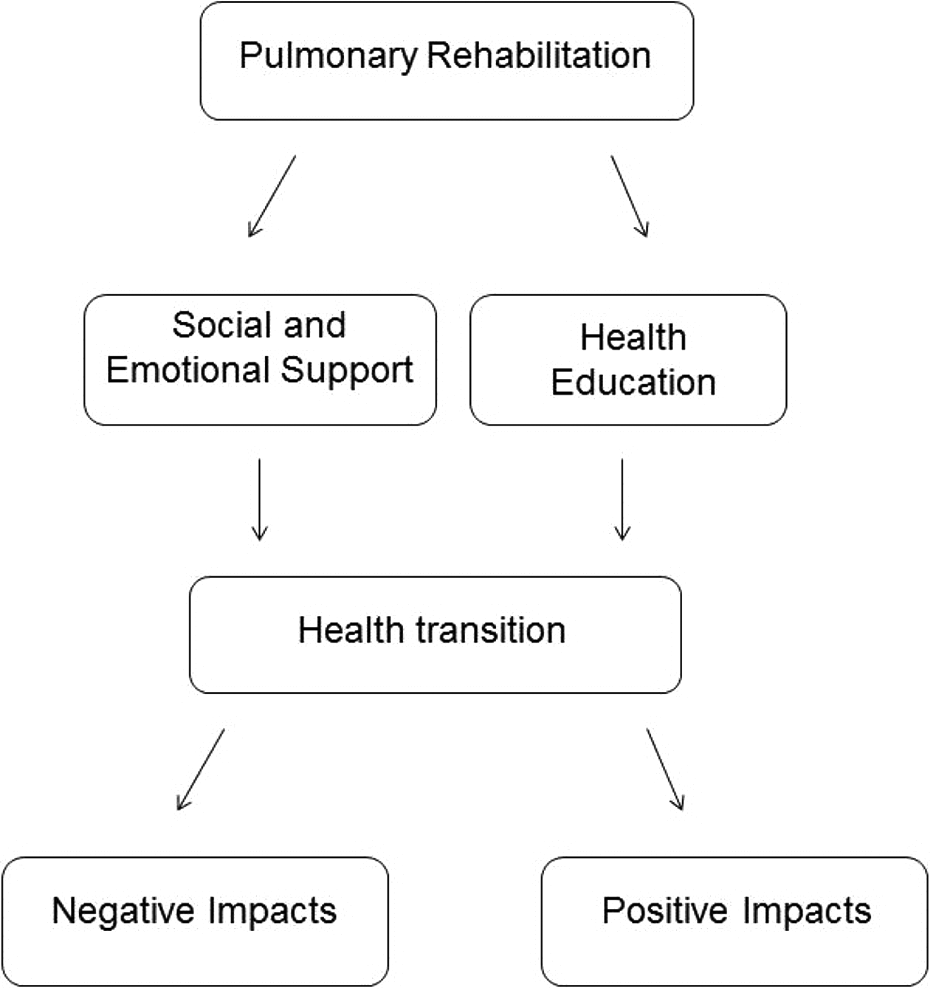
‘Line-of-argument’ of the COPD patients experience with the pulmonary rehabilitation. COPD: chronic obstructive pulmonary disease.
Discussion
This systematic review disclosed the lived experience from the point of view of COPD patients who completed a course of PR. They experienced a feeling of being supported by health professionals, peer groups and family; they learned new knowledge about their illness and how to overcome the suffering caused by it and they took advantage of the opportunities given by rehabilitation to promote considerable physical and psychosocial changes. These positive impacts of PR marked the patients’ ‘health transitions’. 33
While the patient’s voice expresses their treatment experience, it underpins the meanings in their social circle in response to bodily indications perceived as symptoms, that is, the illness behaviour. 34 Although the COPD illness behaviour represents their suffering, the participants from this review were able to control the dynamics of the symptoms and their physical inabilities through PR. Thus, the PR programmes applied in the studies reviewed follow the orientation of the World Health Organization towards a New Public Health and Health Promotion. 35
Although the PR can be applied in a group setting, this treatment depends on each patient’s condition and is planned individually. The ‘health education’ applied through education sessions aims to stimulate the consciousness, illness control and behavioural changes in each individual to promote health improvements. These individual changes indicate that the PR achieves the Health Promotion adopted in 1986 in Ottawa, Canada, 36 defined as ‘the process of enabling people to increase control over and to improve their health’, with the focus on the individual behavioural changes that can be based on health education. Although it is an important part of the PR, it is worth considering that the education process alone does not necessarily lead to behavioural changes. 37
Additionally, the value given to the education sessions and the recognition of the positive impacts of PR by the COPD patients in this review indicates the contribution towards empowerment, part of the Health Promotion, 38 for the treatment of chronic diseases. 39 Here, the empowerment can be identified by the strength of the patients to fight for new achievements and the hope for the future reported by some of them. It reflects the self-efficacy and control promoted by PR. Pulvirenti et al. 40 argue that the process of empowerment involves the use of resources and that special attention must be paid to structural barriers that may affect the individuals’ health condition and their ability to care for and find mechanisms to deal with these barriers. Here, the resources available in PR contributed to patient empowerment; the individuals were able to recognize difficulties and barriers to start or follow the programme, and they also gave possible solutions for them. A literature review points out that the empowerment associated with planned visits and care coordination improves outcomes of COPD treatment. 41 Rohrer et al. 42 highlight the adoption of a direct measure of empowerment, that is, the patients’ own perception of being in control of their own health. Moving in this direction, our systematic review revealed the patients control of their health state.
A systematic review about the influence of illness perceptions on the promotion of self-management in COPD patients who participated in interventions different from PR 43 disclosed that the perceived lack of control over the course of the illness reduces QoL, creates anxiety, leads to social isolation and reduces the motivation to acquire knowledge and skills for self-control. The author underscores that the lack of motivation, the inability to recognize cognitive and instrumental capabilities and the support of social and health professionals influence the low illness self-control and even non-adherence to therapy. Our review showed that the perceptions of COPD patients related to an effective intervention (PR) promotes opposite gains from these findings. In contrast to that study, most of the patients from this review recognized motivation, emotional and instrumental abilities, social and health professionals’ support and control over the COPD. The perception of the PR described here positively influenced the self-management of COPD patients. A qualitative study in Sweden with 12 people with rheumatic diseases 44 revealed the phenomenon of health-promoting self-care as a ‘way of life.’ Similarly, PR, which also provides self-care among other benefits to people with chronic lung disease, 8,9,13,14 was recognized as a new ‘way of life’ by COPD patients. Through the self-care, Swedish chronic patients were ready to understand and respond to the signals their bodies sent out as a result of their illness. 44 After PR, the participants from our review avoided emergency attention due to a better understanding of COPD and the strategies to cope with the symptoms.
One topic regarding qualitative studies that require special attention is the selection bias of participants once they are likely ‘success cases.’ It is not possible to disregard selection bias in favour of those likely to be positive about the subject investigated. 45 If, for example, patients with a negative attitude towards participating in PR or who have experienced little effect despite significant investment are not selected in the sample, information will be lost. In this review, we found that in addition to showing the positive benefits of PR, some articles 16,19,21,22 also revealed the difficulties or problems suffered by the patients during the course of the programme.
Our systematic review has some implications for further research and clinical care in COPD patients. Assessing patients’ ‘treatment-perceptions’ will contribute significantly to a better understanding of the effects of intervention on the illness behaviour and of the adjustments of the negative points identified by the patients. We would encourage PR health professional teams to try to subjectively evaluate their patients in order to know their treatment expectations, their necessities during the intervention and, more importantly, the results achieved with a health intervention, which in this case is PR, although a more tailored approach, need further elaboration in busy clinical settings.
One limitation of this systematic review is the amount of articles included. Even though qualitative studies on COPD have been recently growing, 18,27,28,46 we limited our review to those related to COPD and PR, which gave us a final number of just eight. Nevertheless, our review provided knowledge of COPD patients’ own perception of PR, which was recognized by the patients as an important tool to make physical and psychosocial changes in their daily living with a progressive illness. The importance of investigating patients’ points of view using a systematic review of qualitative articles was the key to understanding what this experience represented to their chronic reality. Thus, the COPD patients’ voice revealed that PR promotes a better ‘way of life’, well-being and important behaviour changes towards Health Promotion 35,36 in chronic disease treatment.
Future considerations
Future qualitative studies in the field of COPD and PR are needed to better understand the impact of this intervention on patients’ lives. Qualitative results may contribute to the treatment modifications or adaptations according to the perspective of the actual beneficiaries.
Footnotes
Appendix
PsycInfo search strategy.
| Search no. | Search terms |
|---|---|
| 1 | exp Chronic Obstructive Pulmonary Disease/ |
| 2 | ((airflow or airway* or lung or lungs or bronchopulmon* or bronchi or bronchial or respiratory or bronchiti*) and chronic and obstruct*).af. |
| 3 | (emphysem* or COAD or COPD).af. |
| 4 | (‘chronic bronchitis’ or ‘chronic lung disease’ or ‘chronic lung diseases’).af. |
| 5 | (‘chronic respiratory disease’ or ‘chronic respiratory diseases’).af. |
| 6 | (‘obstructive lung disease’ or ‘obstructive lung diseases’).af. |
| 7 | (‘obstructive respiratory disease’ or ‘obstructive respiratory diseases’).af. |
| 8 | (‘obstructive respiratory tract disease’ or ‘obstructive respiratory tract diseases’).af. |
| 9 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 |
| 10 | (PR or (pulmonary and rehabilitation)).af. |
| 11 | exp ‘Activities of Daily Living’/ |
| 12 | (((activity or activities) and ‘daily living’) or daily life activity).af. |
| 13 | ADL.af. |
| 14 | exp Self Management/ |
| 15 | (‘self care’ or ‘self management’).af. |
| 16 | exp Lifestyle/ |
| 17 | lifestyle.af. |
| 18 | exp Health Education/ |
| 19 | exp coping behavior/ |
| 20 | ‘coping behavior’.af. |
| 21 | 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 20 |
| 22 | 9 and 21 |
| 23 | exp Qualitative Research/ |
| 24 | ((study or studies or research or method or methods) and qualitative).af. |
| 25 | interviews/ |
| 26 | interview*.af. |
| 27 | exp Observation Methods/ |
| 28 | (((observational or observation) and study) or studies).af. |
| 29 | (narrative or verbatim).af. |
| 30 | exp Grounded Theory/ |
| 31 | ‘grounded theory’.af. |
| 32 | (‘phenomenological study’ or ‘phenomenological studies’ or ‘phenomenological research’).af. |
| 33 | exp ‘Quality of Life’/ |
| 34 | (((quality or qualities) and life) or QOL).af. |
| 35 | 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 |
| 36 | 22 and 35 |
| 37 | exp ‘Literature Review’/ |
| 38 | exp Clinical Trials/ |
| 39 | exp Meta Analysis/ |
| 40 | 37 or 38 or 39 |
| 41 | 36 not 40 |
Acknowledgements
The authors would like to thank Jens De Groot of the Biomedical Library at KU Leuven for the assistance with the literature search strategy and Prof. Fabienne Dobbels of the Centre for Health Services and Nursing Research for her contribution with the study.
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This work was financially supported by a scholarship from the Ministerio de Asuntos Exteriores (MAE), Spain.