
Abstract
The aim of this article is to understand the reasons for attending a chronic obstructive pulmonary disease (COPD)-specific self-management (SM) programme and how attendance at such programmes might be improved. A total of 20 qualitative semistructured interviews were carried out with patients and with lay programme tutors involved in the Better Living with Long term Airways disease (BELLA) pilot trial. Thematic framework data analysis was used. Common reasons for participant attendance arising from patients and tutors include (1) desire to learn about SM, (2) social benefits of meeting others with COPD and (3) altruism. Patients' reasons for poor attendance include (1) being too ill or not feeling ill enough and (2) practical, physical and emotional barriers. Tutor’s explanations for patients’ poor attendance were (1) failure to accept their condition, (2) fear of making a change, (3) lack of adequate support, (4) guilt about smoking and (5) the ‘scripted’ nature of the course. Suggestions for improving programme participation included (1) having choice of several start dates, (2) minimal delay inviting participant onto courses, (3) planning for ‘special needs’. Participation may be better amongst those who have accepted their condition or who are motivated towards improving their condition or to help others. Providing solutions for practical barriers may improve participation. However, alternatives to group-based interventions need to be developed for people with functional and emotional barriers to attendance.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with multiple problems including physical and psychological morbidity, 1 socioeconomic deprivation 2 and stigma. 3
Current pharmacological treatment of COPD is limited, with only modest reductions in exacerbation frequency at best. 4 Pulmonary rehabilitation (PR) is the recommended nonpharmacological treatment of COPD with considerable evidence of benefit to patients. 5 However, a recent systematic review reported that between 8 and 50% of patients with COPD are not attending PR programmes after referral. 6 In addition, 20–40% of eligible patients fail to complete PR programmes. 7 Self-management (SM) programmes are gaining popularity as another nonpharmacological intervention, with evidence showing that they may reduce hospital admissions. 8 In the UK, the flagship SM intervention is the Expert Patients Programme (EPP), a version of the Chronic Disease Self-management Programme (CDSMP) developed by Lorig and Holman in Stanford, California, USA, 9 which is underpinned by the sociocognitive, self-efficacy theory. 10 The aims of SM programmes are to teach skills needed to perform a specific medical regimen, guide health behavioural change and provide emotional support for the patients to control their disease and function better. 11
Review 8 of SM education for COPD patients (with 14 included studies) by Effing et al., reported an overall study completion rate of 86%, with dropout rates ranging from 0 to 30%. However, an overall study participation rate was not reported. The review acknowledged immense heterogeneity between the studies in intervention, follow-up periods, outcome measures and COPD populations. Patients were identified from a variety of different sources. Some studies did not report how patients were identified or invited or the number of patients approached the proportion who were eligible. A key issue in advancing health behaviour research is conducting representative recruitment and having well thought-out retention plans. 12 Non-participation by COPD patients in SM studies is an issue. There is a lack of information about the characteristics of ‘refusers’. 13
There is limited published research on patients’ reasons for attendance or non-attendance at ‘generic’ SM programmes for chronic conditions. 14 –16 Existing studies of patients attending generic SM programmes have tended to involve more females and younger, healthier, less disabled patients than the population of people diagnosed with COPD. 17 Moreover, little is known about participation in generic or COPD-specific SM programmes from the perspective of patients with COPD.
Better understanding of factors that influence participation in these programmes is essential for their delivery. This study explores the reasons for participation of patients with COPD and lay tutors in a COPD-specific SM programme piloted as part of the Better Living with Long term Airways disease (BELLA) study.
Summary of the BELLA pilot trial
The BELLA disease study was a pilot randomised controlled trial and feasibility study of a COPD-specific SM programme 18 for patients with moderate-to-severe disease according to the Global initiative for Chronic Obstructive Lung Disease (GOLD) Criteria. 19
The COPD-specific SM programme was developed by the UK Expert Patient Programme (EPP) Community Interest Company (EPP CIC). 20 The programme was based on the EPP, which is underpinned by the self-efficacy theory of behavioural change, a major component of Bandura’s sociocognitive theory with inclusion of COPD-specific elements (Table 1). The programme addresses five core SM skills: defining the problem, decision making, finding and using resources, forming partnerships with health care providers and taking action. 9 The COPD-specific elements of the programme involved a 3-h session once a week for 7 weeks. In week 4, a local respiratory physician held a session on COPD medications. At the final session, participants were encouraged to join an ongoing local support group, ‘Breathe Easy.’ Six courses were delivered in a local community centre by pairs of lay tutors, at least one of whom had COPD (April–September 2008). All lay tutors were trained, and subsequently accredited, by London EPP CIC to deliver the Expert Patient Programme and the BELLA version of the programme. Similarly, the tutors were trained as effectors of behavioural change. Participants in our study were given upto three different programme dates, if they did not attend the earlier programme. Participants that missed programme sessions because of illness were given the opportunity to attend those sessions to make up the missed programme. Attendance of five or more sessions of seven sessions was our predefinition of the programme ‘completer’. So we labelled participants who attended five or more sessions as ‘high attenders’ and participants with an attendance of less than five sessions were labelled ‘poor attenders’.
COPD elements of the COPD-specific self-management programme
COPD elements of the COPD-specific self-management programme
COPD: chronic obstructive pulmonary disease.
Methods
Participants
The patients for the trial were systematically recruited from primary care disease registers of 10 participating general practitioners and a community respiratory clinic in an east London district identified by the British Lung Foundation as having a particularly high prevalence of COPD 21 and where the generic EPP was not available. Study inclusion criteria were the diagnosis of COPD, age over 35 years, a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) <0.7, either symptomatic COPD defined as an acute exacerbation leading to unscheduled health care attendance within the past year or postbronchodilator FEV1 <80% predicted (moderate COPD, GOLD criteria). Patients with life threatening comorbidity, major psychological illness, inability to give informed consent, who had previously participated in any other SM programme or who were not fluent in English were excluded.
All study participants were informed at recruitment that they might be invited to participate in a qualitative interview later on. According to our study protocol, 15 patient interviews were to be conducted. Individuals were approached on the basis of their fit for the sampling frame and separate written informed consent was sought for their participation in the qualitative study.
A purposive sampling strategy was adopted to ensure that this study obtained full range of views typical of the wider population from participants having significant relation with the research topic. 22 A sampling frame was used to identify 26 potential programme participants (over the duration of the delivery of the six programmes) for the interviews to maximise the variation by number of sessions attended, gender, age, disease severity and treatment with long-term oxygen therapy.
Interviews
A pilot interview was conducted with a patient advisor member of the main study steering group. Individual semistructured face-to-face interviews (Table 2) explored participants’ motivations for attending or not completing the course. Tutors’ were asked about their perceptions on why patients might not participate or complete the course and to comment on the characteristics of high attenders versus poor attenders. Both the groups were asked on how they thought participation might be improved. Interviews ranged from 30 to 60 min in duration, were audio-recorded, anonymised, transcribed, and imported into Nvivo8 software for organisation and facilitation of data analysis.
Interview schedule
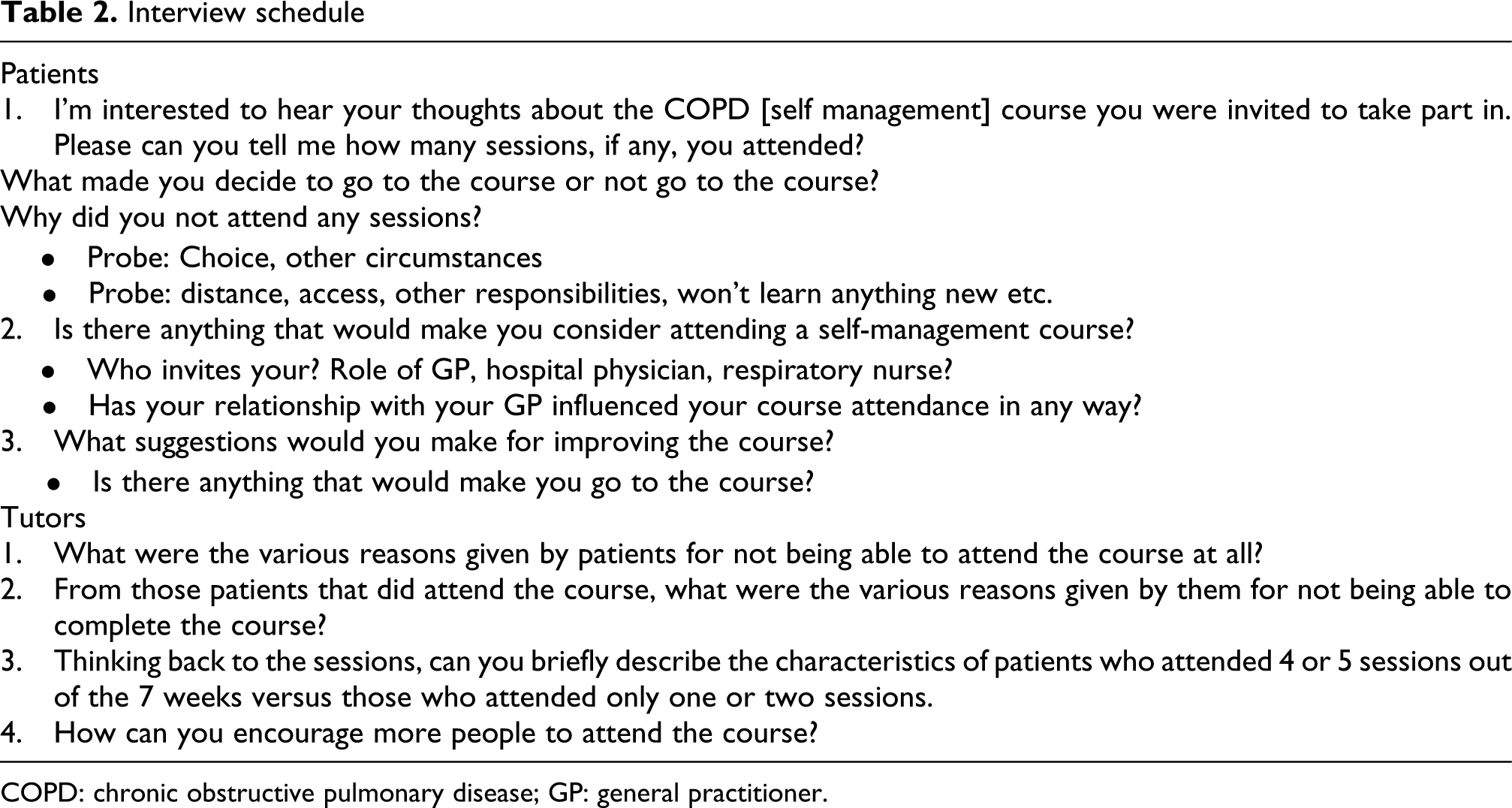
COPD: chronic obstructive pulmonary disease; GP: general practitioner.
Analysis
A ‘thematic framework’ approach was used for data analysis. 23,24 This approach is inductive and grounded but also deductive as it is also used to answer set aims and objectives. The interviewer read all of the transcripts several times to become familiar with the data set, to search for meanings and find patterns in the emerging concepts and themes and to develop a coding scheme. Two other researchers, including one expert in qualitative research, followed a similar process on five transcripts. The three researchers discussed the emerging coding scheme to check for a consistent pattern and any contradictory information. The data from all the transcripts were then charted under emerging themes and concepts giving a detailed account of views and experiences of the participants. A constant reference was made to the study questions when grouping the data under the emerging themes including issues that were raised by the participants. Finally, explanations for the findings were formulated and refined in discussions between the researchers and the study steering group.
Ethical considerations
The study was approved by the Local Research Ethics Committee: The Joint UCL/UCLH Committees on the Ethics of Human Research, Committee Alpha (07/H0715/110). All participants gave written informed consent before conducting the interview.
Results
A total of 116 participants were randomised to 2:1, after baseline data collection, to the offer of the SM programme or usual care. Of the study participants, 46% were male, mean age was 69.5 years and approximately one-third lived alone. Mean FEV1 percentage predicted was 54%, 78% had unscheduled COPD care in the previous 12 months, 17% were using oxygen, 28% were still smoking (self-reported) and only 15% had completed a PR course. At baseline, 32% described their current health as poor or very poor, 48% as fair and 19% as good or very good.
At 6 months follow-up, the results of the trial and feasibility study showed that the programme has a potential to improve health-related quality of life, exercise levels and self-rated health of patients in the intervention group in comparison with the control group. 18 Of the 78 intervention participants who were offered the programme, 64 (82%) agreed to be registered on the course. Amongst those registered participants, 27 (42%) did not attend any sessions, 20 (31%) attended less than five sessions and 31 (48%) attended at least five of the seven sessions (our predetermined definition of a course ‘completer’). A parallel qualitative study enabled us to examine reasons for participation and nonparticipation in the SM programme.
Of the 26 participants, 16 invited for the interview agreed to take part. Amongst those characterised as ‘poor attenders’ at the programme, three refused and one cancelled several appointments. Amongst ‘high attenders,’ one refused and five were late in replying. Interviews took place in the participant’s home or at the respiratory clinic, depending on their preference. Data saturation was achieved from the patient interviewees as no new themes were emerging as the interviews progressed. The four lay tutors responsible for the set-up and delivery of the programme were also interviewed at their home or workplace.
Patient characteristics are presented in Table 3. Of the 16 interviewees, 7 were male, 13 were diagnosed within last 10 years and 8 had severe COPD. Mean age of the interviewees was 70 years, seven lived alone, five were still smoking and four were on long-term oxygen therapy. The findings are discussed in terms of themes and subthemes linked to the aims of the study and presented under Patients’ and Tutors’ views with ‘quotes’ in the boxes.
Characteristics of the 16 programme interviewees
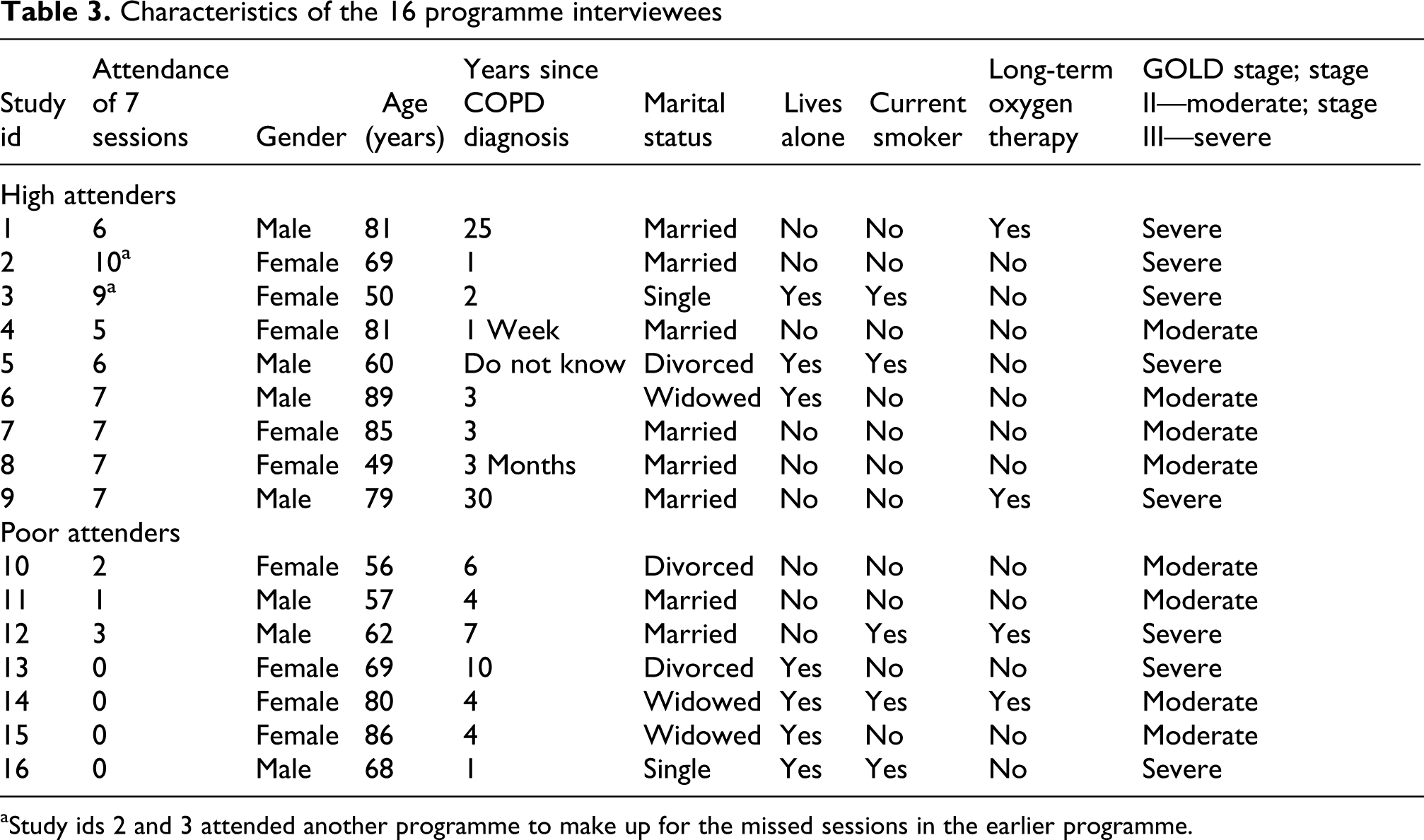
aStudy ids 2 and 3 attended another programme to make up for the missed sessions in the earlier programme.
Reasons for poor attendance
Patients’ view
Not unwell/did not identify self as a ‘person with COPD’
Although everyone in our study had moderate-to-severe COPD, three of the seven participants in the poor attendance category and two of whom were in employment did not consider themselves sufficiently affected by the disease to make attendance worthwhile. These participants were able to continue with most of their routine activities and did not require any further help with their condition (Box 1).
Not ill enough/didn’t identify as a ‘person with COPD’
“…basically after 10 to 15 minutes I realized no I don’t belong here [at the course], ’cos the people there [at the course] are worse than me…these people couldn’t even walk up and down the street without having a…breather so I’m not like that…”(ID 11, Male, 57 yrs, 1 session)
Physical and Psychological limitations
“Well the main reason was I live in this corner…and sometimes if I have a good day I can make it and another time I’m fighting for breath halfway through and then I don’t attempt it…My friend when she comes up to take me, she takes me down in the wheelchair and I get in the car and when we come home she brings me back in the wheelchair….I don’t feel I can intrude on her other time as she works full time (ID 15, Female, 86 yrs, no sessions)
“I didn’t [want] to sit through too much because I tend to get a bit depressed and agitated and what have you…I don’t like getting in with a lot of people…”(ID 12, Male, 62 yrs, 3 sessions)
Other obligations
“…Wednesday morning is my hair dressing day, the hair dresser comes here (home) and we pay her here, then I get my hair done, I cant wash it (hair) myself I can’t reach properly with these arms” (ID 14, Female, 80 yrs, no sessions)
B) Tutors’ view
Blaming others for their condition
“…I’ve found with all of the courses, you would get a drop-off earlier on, and that’s mainly because some of them [patients] thought that they could come along… and blame us for their condition…they think we’re the GP, we’re going to tell them what to do,…and everything is going to be all right, you know?…” (Tutor1)
Fear of making a change
“…[the low attendees]didn’t really want to get things back because they were frightened of what they were going to get back. Because they actually were like in a blanket, and all the services were doing everything for them. So what we were saying is to throw that blanket off…And there’s the panic…they [patients] don’t want to step out of that box.” (Tutor1)
Lack of support
“And a couple of people, I can remember just listening to their partners in the background [when I was on the phone inviting them]– although I don’t know if it was their partners – and just thinking, well, they’re not motivating them! Like (next bit in a slightly negative tone) “Oh, it’s that bird from that research!” (Tutor3)
Guilt about smoking
“…Well, there was someone who came and I don’t think he stayed, and he was a smoker, but the group was quite judgmental about smoking to my surprise…” (Tutor3)
Programme organisational issues
“…I did notice with the first session…it’s quite scripted and driven, which is good…but… people wanted to open up about why they were there, and I don’t think they [patients] got enough opportunity to do that…” (Tutor4)
Physical and psychological limitations
Conversely, three interviewees were so disabled by their COPD and/or comorbidity, including two who were effectively housebound, that they were reliant on their family or friends to take them out of the house. They did not want to intrude anymore on their family or friends’ time.
Two participants experienced low moods and felt uncomfortable being in a group of people that they did not know and dropped out (Box 1).
Other obligations
The course competed with other issues in people’s lives including family obligations, a regular shopping date or even a regular hair dressing appointment.
Other explanations for poor attendance included transport difficulties (despite funds being available to ease this; Box 1).
Tutors’ views
Tutors’ also mentioned all the things that patients listed. However, they also gave some strikingly different explanations including the following.
Blaming others for their condition. According to one tutor some patients preferred to blame others for their condition rather than accepting and learning how to manage it (Box 1).
Fear of making a change. The same tutor felt that some participants were so used to getting help from others that they were frightened to make a change to their lives (Box 1).
Lack of support. Two tutors believed lack of support from family or those around the patient, might have prevented attendance (Box 1).
Guilt about smoking. The programme was specifically designed not to exclude smokers but one tutor felt that guilt about smoking was a reason for poor attendance (Box 1).
Programme organisational issues. Finally, one tutor noted that the programme was rather curriculum-centred and that this may have excluded people from expressing themselves early on so that some lost interest (Box 1).
Reasons for high attendance
Patients’ and tutors’ views
Wanted to learn about SM
Four of the nine high attenders wanted to learn more about their condition, having accepted that help from conventional health services had reached its limits (Box 2).
A) Patients’ and tutors’ views
Wanted to learn about self-management
“…because I didn’t like the way I was going…I thought well the doctors don’t seem to be doing much although I’ve got the inhalers and I thought I wondered if there was anything I could do differently…”(ID 7, Female, 85 yrs, attended 7 sessions)
Socialising and wanting to meet others with the same illness
“…from the social side of it as well ’cos when you’re stuck in doors like 24/7 virtually and just to be able to get out and meet other people that are in the same predicament…it’s not so embarrassing…”(ID 5, Male, 60 yrs, 6 sessions)
“…I thought it was such a great relief to see these people [tutors], you know, talking about their illnesses as well, and they knew what you were going through! And that made me come back…” (ID 8, Female, 49 yrs, 7 sessions)
Altruism
“I tried to help, really. In myself, I’m all right…I said I’d go…because I’m interested…if it can help other people, and I think it probably did…” (ID 6, Male, 89 yrs, 7sessions)
Socialising and wanting to meet others with the same illness
Three participants felt that attending the course would be a great opportunity to get out of the house and meet people with the same condition. For some, it was the only place they could socialise. For one participant having programme tutors who themselves had COPD was also an incentive to attend (Box 2).
Altruism
Helping others was a motive for attendance for two participants (Box 2).
Tutors’ similarly believed that good attenders were not happy about having COPD but had accepted it and wanted to learn to live with it.
Steps to improve programme participation
Patients’ view
Groups of similar COPD severity
Two participants, one high and one low attender, suggested having a programme for groups of patients with similar COPD severity where people could relate to each other easily. This might motivate or encourage participation (Box 3).
Duration of the course
One of the three interviewees who were in employment, felt that chopping the length and duration of the course might make a difference to attendance (Box 3).
A) Patients’ view
Groups of similar COPD severity
“…a separate one [group]…if there was more people who was mild as me as I am then it would encourage me to go more [to the course]…you should…have more of a course to stop smoking…I mean that’s the main thing isn’t it?” (ID 11, Male, 57 yrs, 1 session)
Duration of the course
“… I think three hours is a bit too long…actually for a session. Maybe in bite-sized chunks,…of one and a half hours,… over a period of time,… maybe a week or so; something like that, rather than the once a week ….for those people who aren’t working,…I was working, so I think it suited to me to come each week, you know, and do the three hours…” (ID 8, Female, 49 yrs, 7 sessions)
B) Tutors’ views
Programme organisation
“I think we should have had a rule that we invited people like the day after or two days after (recruitment)…or it might have been even really good to have done it that day (when researcher did recruitment)…I don’t know if that would have made any difference. But I also think part of it was, with quite a few people (course participants), that I’d built up quite a good relationship on the telephone with them…” (Tutor3).
“…I think the practicalities of people actually coming on the course have got to be thought through as well…there should be something in place to give these people the access they need. So if they’ve got special needs, then we should be trying to meet those…like that lady…in a wheelchair” (Tutor4)
“…What I found is if this course goes on, then,…what you’d say to them then is, “I realise that, you know, you’re not ready to go on the course now, but there will be one in January or July, whenever.” It gives them another option, gives them time to think and I always say to people, “I’ll leave you on the list and they’ll contact you for the next course. It’d be really great to see you and I’ve been chatting to you on the phone, it’s been lovely to meet you. Really, so if you just come along to the first one and introduce yourself…And that’s how I get them there…” (Tutor1).
Tutors’ views
Programme organisation
The tutors felt that improving certain organisational aspects may help improve programme uptake. Examples given included the following: inviting patients within a day or two of the programme being offered to them, the individual inviting the patient to the programme should aim to develop a rapport with patients’ to help increase the chances of them remembering about the programme amidst their day-to-day living. One tutor stressed the importance of planning for participants’ ‘special needs’, e.g. wheelchair access. Another suggestion was that the programme should be flexible with several joining dates to allow participants to consider it and not feel pressured (Box 3).
Discussion
Summary of main findings
This study sheds light on why some patients with moderate-to-severe COPD were reluctant or unable to attend a COPD-specific SM programme, whilst others were motivated to attend from a sufficient sample size of 16 patient interviews and 4 interviews with programme tutors. Tutors and participants were in agreement with the following reasons for high attendance: a desire to learn more about their condition, socialising and meeting others with the same illness and altruism. Tutors agreed with some patient explanations, such as physical limitations, competing priorities and patients not recognising themselves as having COPD, for poor attendance. Some patients felt uncomfortable being in a group and going to an unfamiliar environment. Tutors also gave different explanations, such as fear of making changes, unwillingness to take responsibility for SM, lack of support from family or smoking, for poor attendance. These are the explanations that are somewhat stigmatising and would require a considerable degree of self-critical insight for patients to have expressed. The attitudes of other course participants to smoking may have played a part. Particular features of the course, such as lay tutors having the same condition as the participants – a favourable feature, whilst poor access and heavy reliance on scripted programme content may have been unfavourable, may also have influenced programme attendance. Patients felt that altering the length and duration of the programme to accommodate people’s routines might encourage attendance. Having separate groups with similar COPD severities might promote programme participation. Tutors’ suggestions were to have a flexible programme with several joining dates, time between the offer of the programme to invite should be a few days and planning for patients’ special needs.
Comparisons with existing literature
Our findings support many of the findings about attendance in studies of generic SM programmes. 14 –16 Altruism was found a common reason for attendance in a UK generic EPP study 14 and a recent Australian COPD CDSM trial. 25 Wanting to see benefit for themselves was also a reason for participation in Willis et al.’s study. 25 Social isolation was a reason for attendance in a generic SM programme study. 15 Feelings of social isolation can lead to people becoming resigned to their situation; patients then find it difficult to express themselves and relate to others. 26 In addition, our study showed that the patients wanted to attend to meet others with the same illness. Patients with COPD prefer engagement related to activities that allow social integration, role and independence. 26
The reasons found for poor attendance in our study were similar to Abraham and Gardener’s 15 generic SM programme study that included access and logistic issues. Another study of a programme for COPD patients 27 reported similar access issues. Reasons for nonparticipation also matched a US CDSMP study, 16 which were fatigue, depression, mobility and transport problems, lack of family or social support and discomfort in group settings. Two studies 28,29 have reported that the attendance is affected by patients’ negative perceptions of their illness. In our study, negative beliefs about their illness, such as not accepting one’s condition but blaming others for their illness or not believing that a change in health behaviour will make a difference, 28,30 could be exacerbated by depression and anxiety, states which are widely associated with COPD, 31,32 or by experiencing negative social interactions. 33 Lack of support from family may predispose patients to lose interest in learning skills and carrying out tasks. 34 In addition, our findings that some poor attenders felt relatively unaffected by their COPD supports findings reported elsewhere. 35
In comparison with the generic SM programme studies, our patients were older and had much lower self-reported health status. We also experienced more male participation in comparison with other studies, perhaps due to targeting a condition associated with smoking, the presence of a male lay tutor, or recruiting through primary care registers rather than volunteers.
Implications for future research and clinical practice
Our findings suggest that there are valid reasons to continue delivering COPD-specific SM programmes to people with moderate-to-severe COPD and to people who are motivated and committed to learning about SM. Getting patients more involved in their care, including developing partnerships with health professionals and reducing the disease burden, is a recommendation of national and health policy guidelines 36 and delivering group-based SM programmes is one way to achieve this. However, this type of SM intervention may not be suitable for all the patients with moderate-to-severe COPD because patients might not have accepted their condition or are housebound or suffer from emotional or functional limitations or have competing priorities. The negative perception of patients towards themselves and their illness requires better understanding. 37 Roles of social support and patient support networks should be recognized so that more time could be spent on people who have negative social interactions or those who live in social isolation. 33 One way to tackle this problem could be for clinicians to undergo training in conducting psychosocial needs assessment using the ‘Patient Report Informing Self-Management Support’ form 38 or information needs assessment. 39 Greater awareness of the importance of SM education should be promoted amongst clinicians 40 with the provision of clear referral procedures to these programmes. 41 Alternatives may need to be developed in collaboration with this patient group, 42 for example, delivering the programme in a primary care setting to reduce patients’ anxiety levels. 43 Other examples could be provision of SM education including remote disease monitoring by a registered respiratory therapist, 44 face-to-face education followed by monthly phone calls by case managers 45 or a patient-centred model using a health mentoring approach (grounded in behavioural psychology theory and includes motivational interviewing, goal setting, action planning and problem-solving skills and SM support theory and practice) delivered by phone or face-to-face. 46
Simple refinements to the COPD SM programme that we evaluated could improve attendance. First, patients can be offered several joining dates; participants in our study were invited upto three times to join a missed programme or were allowed to make up for the missed sessions by attending another programme. In practice, this is similarly seen in PR programmes, where patients are offered the opportunity to attend another programme to make up for missed sessions or a whole missed programme. Second, inviting patients within a few days of being approached for the programme is desirable; patients should be sent reminders between being registered and start of the programme to avoid patients feeling forgotten or to help them not to forget about the programme amidst their routine activities. Third, consideration needs to be given to the accessibility of programme venues, such as wheelchair access and lift availability. Perhaps also greater awareness by practitioners of the programme content and its benefits so that they could encourage and recommend programmes to patients 27,34,35,47 in addition to allowing patient recruitment from primary care may help to improve programme attendance. Educational initiatives are a good idea, but unless they are accompanied by a change in the way health professionals respond to patients, they are unlikely to have a sustained impact. 48
Strengths and limitations of the study
This study is believed to be the first to specifically explore views on participation in a group-based COPD-specific SM programme from the perspectives of COPD patients and lay tutors. This study attempted to overcome the problems of other studies 14 –16 that have relied only on the perception of patients. Tutors were able to deliver insight into poor attendance that patients were perhaps reluctant to voice, and this is the first time that a qualitative study has reported the perspective of lay tutors on this topic. Additionally, the study involves a proportion of participants with severe levels of COPD, reflecting the realities of this disease in a way that other studies of less severely disabled patients may not. 14 –16 Poor attendees were more reluctant to be interviewed, a difficulty commonly experienced with nonparticipants in studies. Being the first study of its kind, we must be cautious in generalising from this study to other COPD patient groups.
Footnotes
Funding
This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit Program [Grant reference number PB-PG-0906-11172]. The views expressed are those of the authors and not necessarily the NHS, the NIHR or the UK Department of Health.
Acknowledgements
The authors thank all the course participants and the lay course tutors, participating GP practice staff and the community respiratory clinic, UK Expert Patient Program Community Interest Company for their collaboration with the study and our steering group committee.
Conflict of interest
The views expressed in the article are those of the authors and not necessarily those of the NHS, the NIHR or the UK Department of Health.