
Abstract
Objectives
To determine whether a remote behaviour change service (Active Steps), delivered by a UK charity, can increase physical activity over a 12-month period in adults with lung disease.
Methods
Active Steps (n=166) consisted of 1:1 telephone health coaching for 12 months alongside printed (e.g. activity diary and chart, information and goal setting booklet) and digital behaviour change strategies (e.g. exercise videos, motivational newsletters, pedometer). A concurrent control group was recruited (n=80) for comparison. Self-reported physical activity (Short Active Lives Survey) and self-reported health (EQ-VAS) were collected at baseline, 3, 6, and 12 months. Logistic regression models (adjusted for confounders) were used to analyse the odds of becoming physically active or average changes in physical activity time and EQ-VAS.
Results
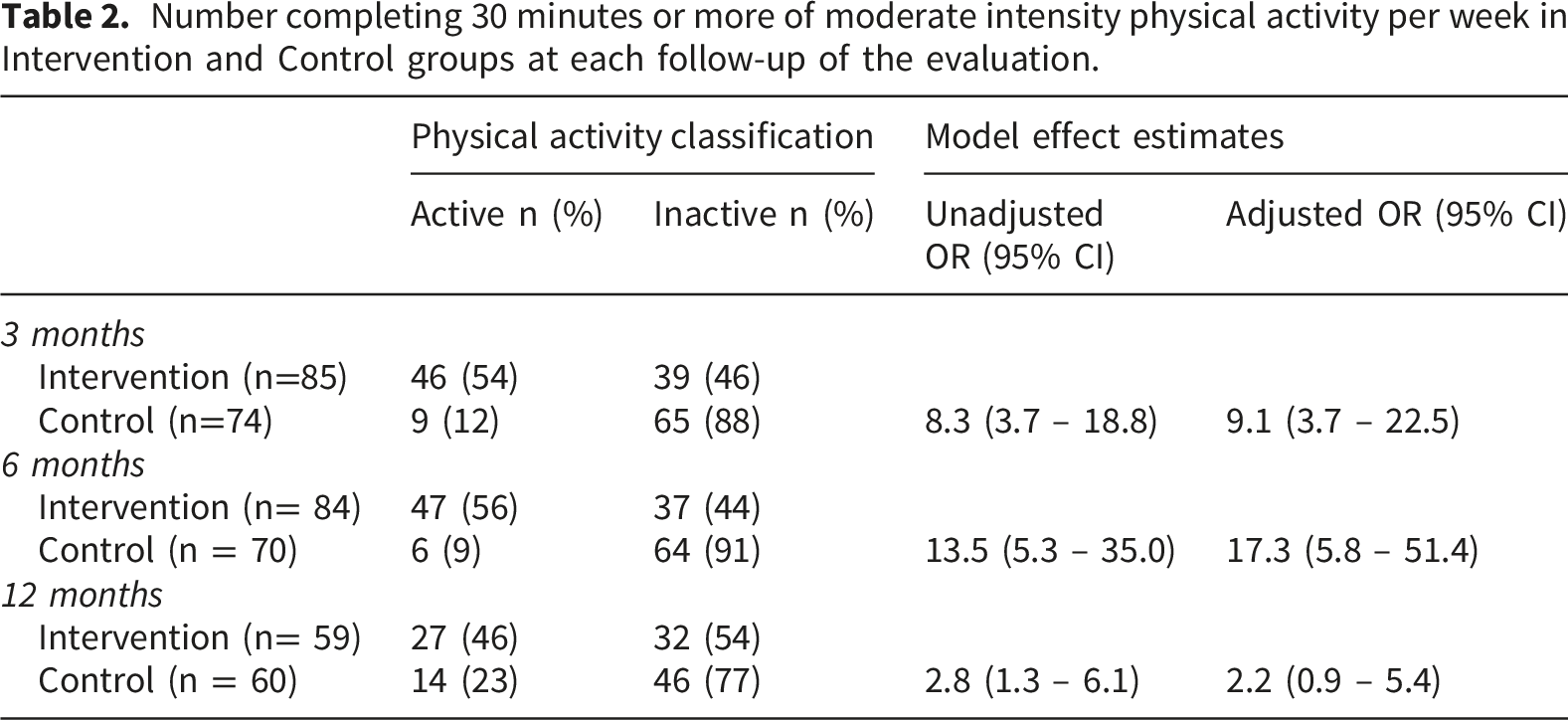
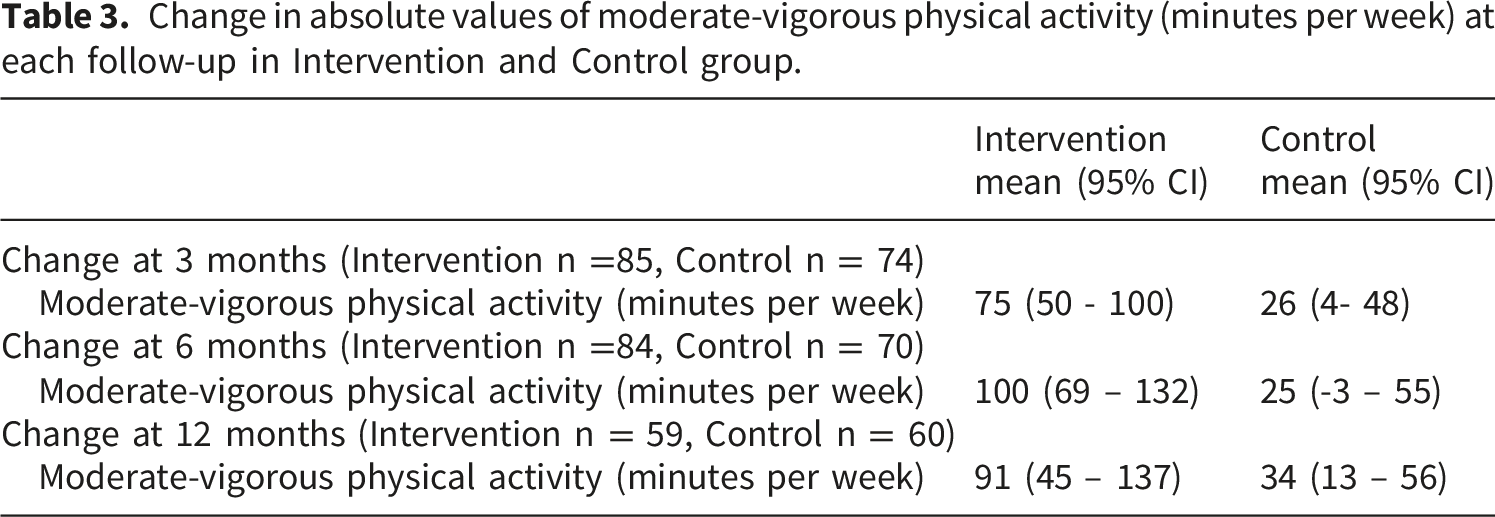
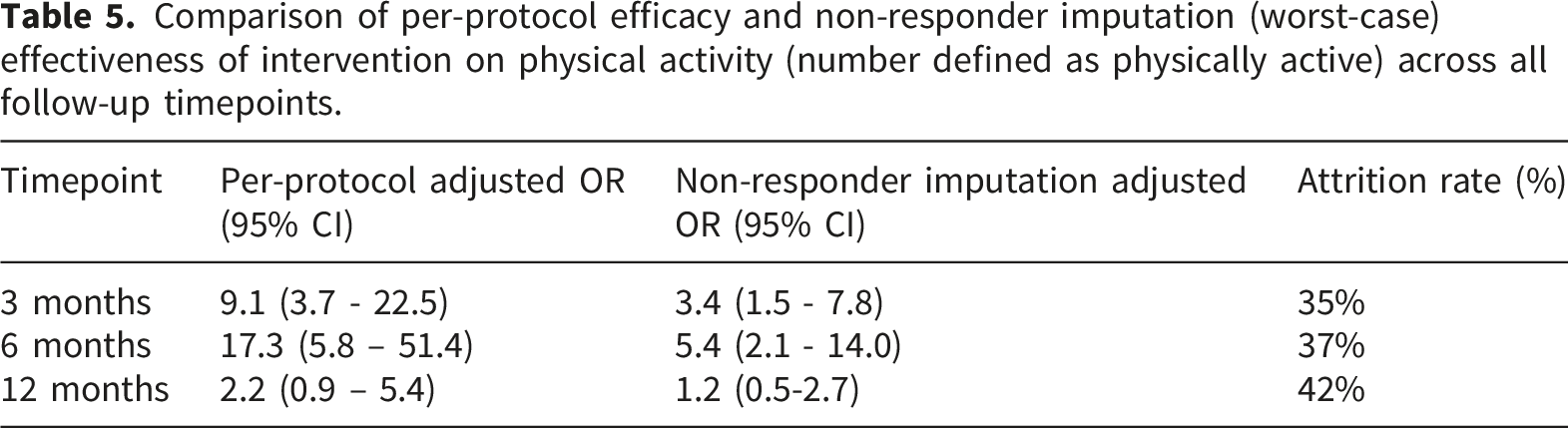
Primary outcome: The number of participants defined as physically active at 12 months was greater with Active Steps (46%) compared to controls (23%) which was statistically significant in an unadjusted (odds ratio (OR) [95% confidence intervals (CI)]:2.8 [1.3-6.1], p=0.011) but not adjusted model (OR: 2.2 [0.9-5.4], p=0.097). Secondary outcomes: Compared to controls, Active Steps increased the number of participants physically active at 3 and 6 months, increased the weekly minutes of moderate-vigorous physical activity and improved self-reported health (EQ-VAS) across all timepoints.
Discussion
Our findings suggest that charity-led remote behaviour change support is effective in the short-to-medium-term in adults with lung disease, but high participant attrition necessitates caution in interpreting sustained effect estimates at 12 months. Further long-term evaluations are needed to address adherence and sustainability of such services.
Background
Adults diagnosed with chronic lung disease such as asthma, bronchiectasis, chronic obstructive pulmonary disease (COPD), and interstitial lung disease have reduced levels of daily physical activity when compared to healthy counterparts of a similar age, with many not meeting the recommended physical activity guidelines.1–5
Increasing physical activity in people with chronic lung disease is associated with improved symptoms, physical function and quality of life whereas inactivity is associated with adverse clinical outcomes, including increased hospitalisation and all-cause mortality.6–8 Structured physical activity programmes, such as pulmonary rehabilitation are one of the key treatments for chronic lung disease. A six-to-eight week course of pulmonary rehabilitation is known to have well-established benefits including clinically important improvements in exercise capacity, quality of life and respiratory symptoms such as dyspneoa. 9 However, there are barriers preventing people with chronic lung disease attending pulmonary rehabilitation including accessibility, under-referral and long waiting times. 10 Even when a pulmonary rehabilitation program is completed, this does not always translate to changes in long-term daily physical activity for people with chronic lung disease. 11
More strategies are needed to increase physical activity across a wider range of settings for people with chronic lung disease including catering for when structured physical activity programmes cannot be accessed or before starting such programmes. Asthma + Lung UK (formerly British Lung Foundation) received funding to develop, deliver and test a new remote health coaching behaviour change service called Active Steps. The co-design and development of this service have been previously reported. 12 The primary aim of this study was to determine whether the remote behaviour change service could increase physical activity in adults with lung disease who are physically inactive. The secondary aim was to assess the impact of the behaviour change service on self-reported health and disease-specific quality of life.
Methods
Design
This was a non-randomised controlled study conducted between February 2019 and October 2021.
Participants
Eligibility criteria
The target population were physically inactive adults living with a chronic lung disease (asthma, bronchiectasis, COPD, interstitial lung disease, lung cancer, mesothelioma). Physical inactivity was defined - in accordance with public health services in England13,14 - as undertaking less than 30 minutes in total of moderate-vigorous intensity physical activity per week. People unable or unwilling to provide their consent for the study were excluded.
Interventions
Active Steps delivery model.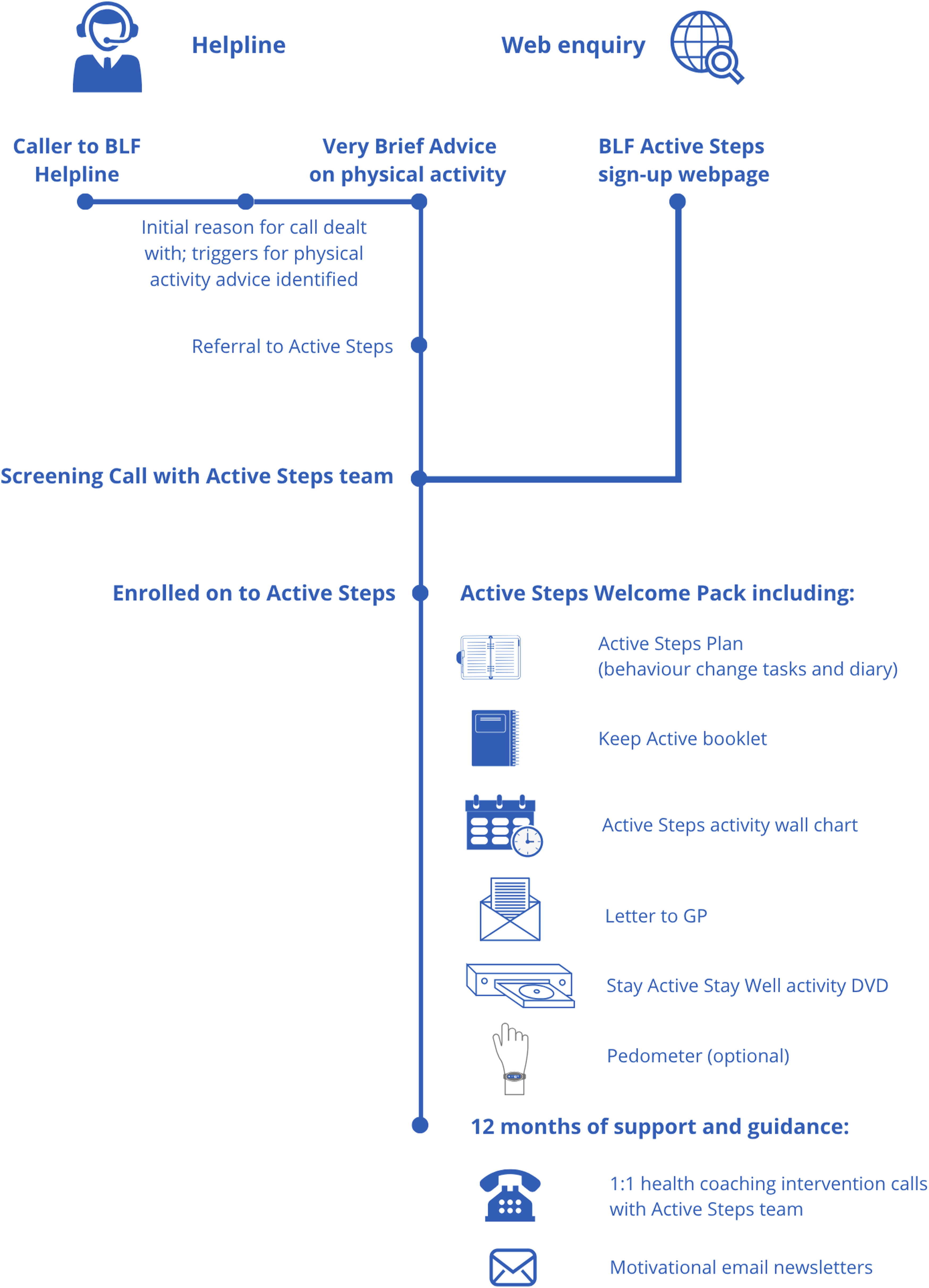
Outcomes
Primary
The primary outcome was a between-group comparison of the number of participants completing 30 minutes or more of moderate-to-vigorous physical activity per week at 12 months. Physical activity was measured by the Short Active Lives Survey (SALS). The Active Steps service was funded as part of a larger programme by Sport England to impact on physical activity measured by SALS. Since January 2018 SALS has been Sport England’s recommended physical activity measurement tool for its funded projects. SALS is a self-reported tool to measure adult physical activity levels. SALS consists of three questions, each containing three sub-questions, which establish activity levels in relation to walking, cycling and sport/fitness activities. The tool asks the number of days the activity was undertaken, the duration, and whether the effort was enough to raise their breathing rate. SALS has previously been validated against other recognised self-reported and device-based measures of physical activity. 16
Secondary
Between-group comparisons of the number of participants completing 30 minutes or more of moderate-to-vigorous physical activity per week at 3 and 6 months were secondary outcomes. Between-group changes in total self-reported moderate-to-vigorous physical activity were also assessed by SALS at 3, 6 and 12 months. Between-group changes in self-reported health at 3, 6 and 12 months were measured using the visual analogue scale (EQ VAS) and descriptive system of the EQ-5D-5L quesstionnaire. 17 The intervention participants completed a short-form chronic respiratory disease questionnaire (CRQ)18–20 as a measure of respiratory-specific quality of life at baseline, 3 months, 6 months and 12 months.
Recruitment
Data collection and follow-up
The British Lung Foundation collected baseline, 3, 6 and 12-month data for intervention participants over the telephone with data entry to purpose-built web-based surveys (Qualtrics, Utah, United States). Data were collected by a member of the Active Steps team who was not involved in delivering intervention calls to the specific participant, with data submitted directly to an independent research team. In September 2019, data collection procedures were expanded to include the option of intervention participants being emailed a link to the web-based surveys to self-complete, if staff were unable to schedule a telephone follow-up. Baseline and outcome data for the control group were collected at baseline, 3, 6 and 12 months by the research team using the same web-based surveys (Qualtrics) as the Active Steps service users.
Sample size
This was a non-randomised study where a concurrent control group was sought during the same study period as a group receiving a new service implemented by a national charity. The evaluation was designed to detect an absolute difference of 10% in the proportion of participants being physically active at 12 months. Based on 80% statistical power and a 5% level of significance, 58 participants per group were required. British Lung Foundation had originally estimated capacity to enrol 200 participants into Active Steps over the service period. However, we conservatively estimated that at least 80 participants would be recruited for both the intervention and control groups in the study period. This would allow for a 25% dropout rate over the 12-month follow-up period.
Data analysis
All analyses were performed using SPSS v27 (IBM Armonk, New York). The primary approach for analysis was a “per protocol” analysis. This referred to the analysis of only those participants who strictly adhered to the project (protocol) including receipt of the intervention for 12 months and/or provided data at follow-up.
The primary outcome was assessed using binary logistic regression. Given the study design, we first identified potential confounders for the outcome of physical activity. A directed acyclic graph (DAG) 21 was constructed (Supplementary Material, Figure S1) to identify the minimal sufficient set of potential confounders for adjusting the effect of the intervention on physical activity. Based on prior literature,22,23 baseline differences in demographic or clinical factors between groups in the study, and inspection of the DAG, we identified age, gender, breathlessness severity, diagnosis of diabetes, heart condition or mental health condition, and social deprivation as potential confounders of the effect of the intervention on physical activity.
Binary regression models with and without adjustment for these potential confounders were used to estimate the effect (interpreted as an odds ratio) of the intervention on number of participants completing 30 minutes or more of moderate-vigorous physical activity per week at 3, 6 and 12 months. Changes from baseline at 3, 6 or 12 months in the secondary outcomes of total minutes of physical activity and self-reported health (EQ-VAS) were assessed using logistic regression with or without adjustment for the potential confounders. The potential confounders for the outcome of self-reported health (EQ-VAS) were considered similar to that of physical activity. Analysis of the effect of intervention on self-reported health (EQ-VAS) was performed with or without adjustment for the potential confounders. Descriptive statistics of the health profiles from the EQ-5D questionnaire were reported in accordance with published methods (see supplementary material). 24 Changes from baseline to 12 months in CRQ domain scores were assessed using paired t-tests. The short to medium changes (at 3 and 6 months) in CRQ domain scores were assessed using one-way repeated measures analysis of variance followed by post-hoc paired t-tests.
Given the primary focus of the intervention was to increase the number of people physically active at 12 months, we also undertook a sensitivity analysis using non-responder imputation. All participants lost to follow-up at 12 months were classified as inactive to provide a “worst-case” conservative estimate alongside the per-protocol analysis. Baseline characteristics of participants who completed the 12-month follow-up or were lost to follow-up were compared within both groups. The DAG informed confounders used in the primary analysis were also applied in the non-responder imputation. To support interpretation of results across the study duration, non-responder imputation was also conducted with physical activity at 3 months and 6 months.
Results
Completeness of follow-up
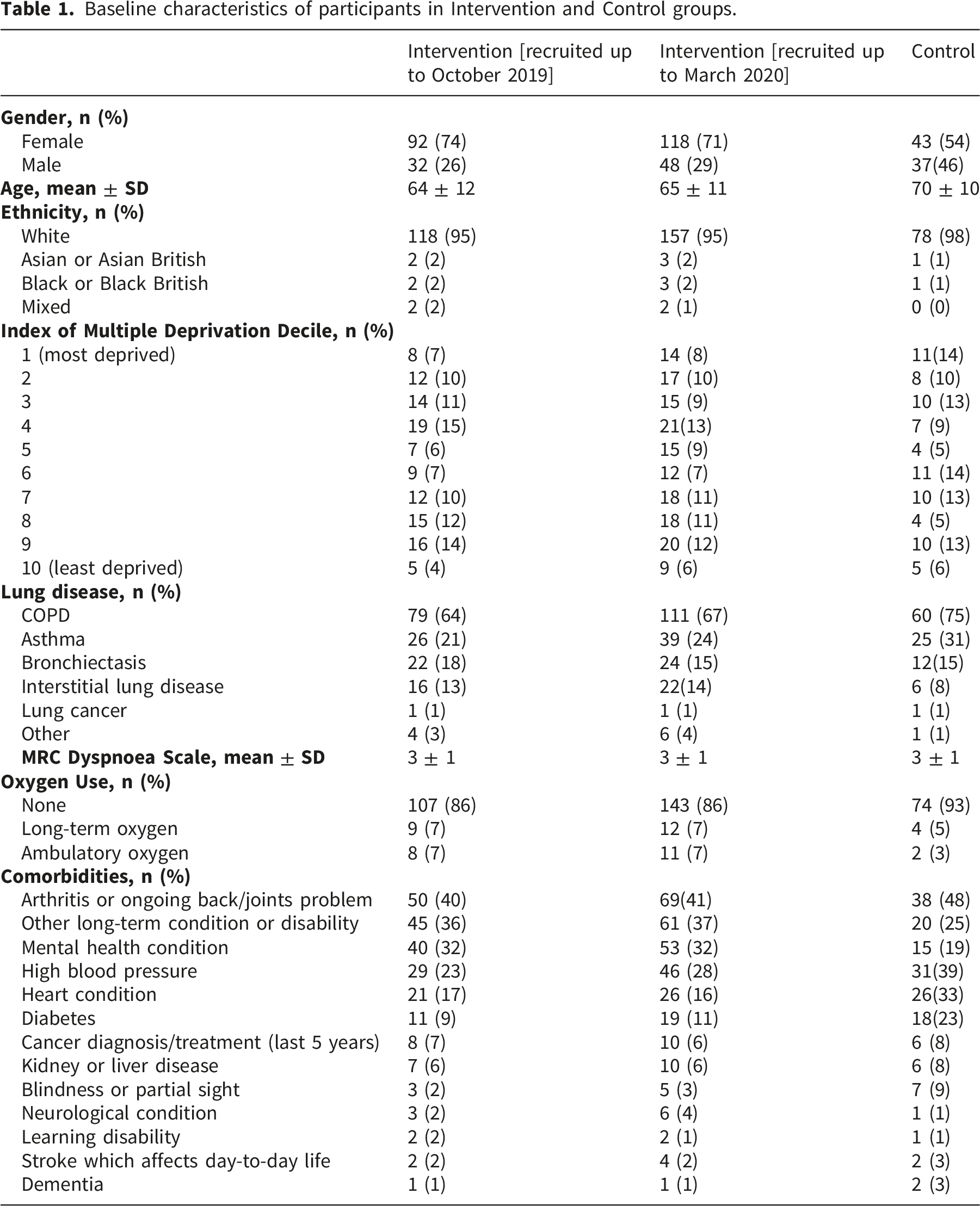
Baseline characteristics of participants in Intervention and Control groups.
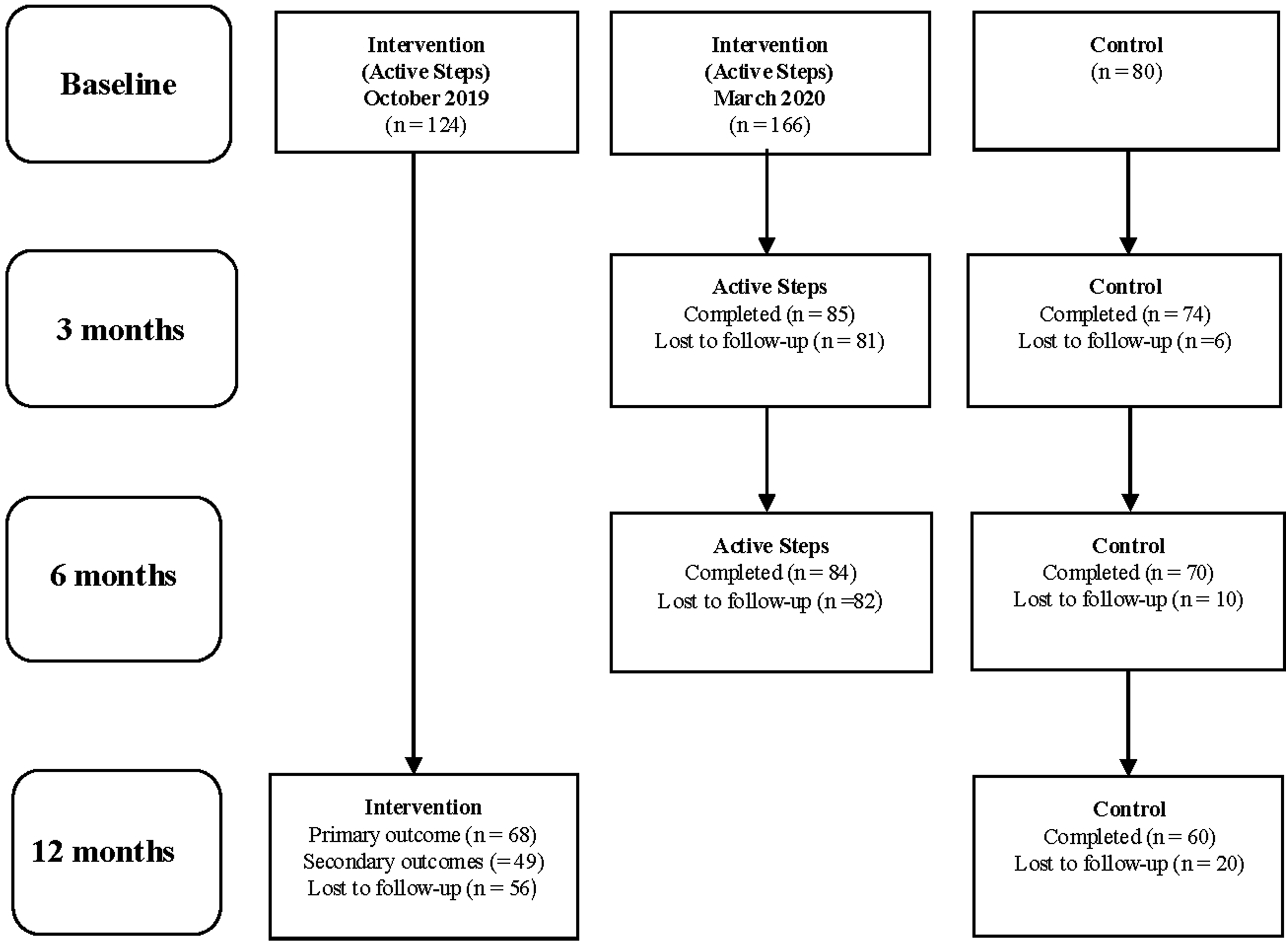
Completeness of follow up of Intervention and Control participants.
Primary outcome
Number completing 30 minutes or more of moderate intensity physical activity per week in Intervention and Control groups at each follow-up of the evaluation.
Secondary outcomes
Change in absolute values of moderate-vigorous physical activity (minutes per week) at each follow-up in Intervention and Control group.
Changes in EQ-VAS at each follow-up in Intervention and Control group.

CRQ: At 12 months, the mean ratings (95% CI) improved by 0.5 (0.2-1.0, p=0.008), 0.6 (0.2–1.0. p=0.005), 0.8 (0.4–1.2, p<0.001) and 0.5 (0.1–1.0, p=0.026) for dyspnoea, fatigue, emotional function and mastery domains respectively, all of which were statistically significant and of a magnitude considered to be clinically meaningful. Repeated measures ANOVA revealed a main effect of time on dyspnoea (p< 0.001), fatigue (p< 0.001), emotional function (p<0.001) and mastery (p=0.006) at 3 and 6 months. At 3 months, the mean ratings (95%CI) improved by 0.5 (0.1–0.8, p=0.014), 0.6 (0.6, 0.2–0.9, p=0.002), 0.7 (0.2–1.2, p=0.005) and 0.6 (0.1–1.0, p=0.007) for dyspnoea, fatigue, emotional function and mastery domains respectively, all of which were statistically significant and of a magnitude considered to be clinically meaningful. At 6 months, the mean ratings (95%CI) improved by 0.8 (0.8, 0.3–1.2, p<0.001), 0.6 (0.3–1.0, p<0.001), 0.9 (0.6–1.3, p<0.001) and 0.4, (0.1–1.9, p=0.147) for dyspnoea, fatigue, emotional function and mastery domains respectively, all of which were statistically significant and of a magnitude considered to be clinically meaningful except for the mastery domain.
Sensitivity analyses
Comparison of per-protocol efficacy and non-responder imputation (worst-case) effectiveness of intervention on physical activity (number defined as physically active) across all follow-up timepoints.
Discussion
Summary of main findings
Per protocol analysis of adults who engaged with a remote behaviour change service (Active Steps) were twice as likely to be physically active at 12 months than a control group. However, this intervention effect was attenuated (to 1.2 times) in a conservative sensitivity analysis assuming all participants lost to follow-up remained inactive, reflecting the impact of high participant attrition on statistical power and certainty of the long-term effects of the service. Conversely, per protocol analysis revealed Active Steps service users were 9 times and 17 times more likely to be physically active at 3 months and 6 months. Sensitivity analysis confirmed these short-to-medium term changes were robust (3 and 5 times more likely to be physically active at 3 and 6 months) even under worst-case assumptions. Changes in physical activity in the per-protocol analysis were accompanied by clinically meaningful improvements in self-reported health and disease-specific quality of life.
Existing literature
Systematic reviews of remote coaching interventions delivered through internet and telephone have shown potential to support behaviour change and promote physical activity in people with chronic lung disease, 25 but they are not readily available in the UK. Similar to randomised controlled trials,26–28 which have assessed the effects of health-coaching interventions, we observed benefits in the short-term and long term. The current study targeted the intervention at adults who were defined as physically inactive, with this at the time being the UK Chief Medical Officers/Sport England definition of less than 30 minutes of moderate-vigorous physical activity per week.13,14,29 The current study indicates the potential for health coaching interventions to support the most physically inactive people in lung disease populations. Although the absolute between group differences in weekly physical activity were ∼ 60 minutes or less, such changes with the intervention were accompanied with clinically meaningful improvements in self-reported health and quality of life. Health coaching interventions, with a focus on physical activity behaviours have been shown in randomised controlled trials to increase quality of life in COPD 30 but less evidence is available for other chronic lung diseases.
Strengths and limitations of the study
To our knowledge, this study is the first to report the analysis of a service delivered remotely by a UK charity to modify physical activity in inactive adults with lung disease. We acknowledge that our outcome measures were all self-reported, which may be prone to recall and social desirability bias. However, outcomes were selected based on physical activity measures (SALS) used at population level in England 14 and tools (EQ5D, CRQ) that are frequently used to assess the health impact of behaviour change interventions in people living with lung disease.31,32 Methods were also undertaken to limit risk of bias through keeping data collection and intervention delivery in the service as independent as possible and the data submitted immediately to the research team via a web-based system upon collection. The specific nature of the study design (i.e. lack of randomisation) does not eliminate the greater risk of bias with observational studies. For example, participants in the intervention and control groups relied on different recruitment sources albeit the use of a control group allowed for better scrutiny of longitudinal changes in physical activity and health status compared to other possible designs of service implementation in the ‘real world’ (e.g. single arm before-and-after study designs). It is worthy to note that usual care in the control group was not strictly controlled, where some participants had unexpected increases in physical activity. The CRQ was only assessed within Active Steps participants, hence we cannot be certain that the clinically meaningful improvements in CRQ domains at all timepoints were due to the intervention alone.
The eligibility criteria for this study were designed to be as broad as possible to replicate those likely to seek support from the British Lung Foundation. Although the behaviour service engaged with people with a range of lung diseases from various socioeconomic backgrounds, the service largely recruited females. Baseline imbalances between the two study groups were also observed in other characteristics such as age, mental health, heart disease and diabetes. The analyses on physical activity and self-reported health were performed with adjustments for these baseline imbalances. While these adjustments helped to reduce the risk of confounding bias it impacted statistical power in the per protocol analysis, as seen with the shift away from statistically significant effects in the primary outcome between the unadjusted and adjusted model. The current study, both in intervention delivery and data collection also met the difficult conditions of the COVID-19 pandemic. Although the study was aided by remote service delivery and data collection, the impact of COVID-19 on the charity’s services and delivery (including financial position and staffing) meant the total number of participants enrolled in the service over the study period was less than expected and those recruited between late 2019 and March 2020 were unable to be followed-up for the full 12-month period.
A key limitation of this study was the participant attrition rate, particularly important when interpreting true effectiveness of the intervention in the ‘real world’. The primary approach to this study was a per protocol analysis to evaluate the efficacy of the service, in those who remain engaged throughout the 12-month follow-up. To support collection of the primary outcome, the British Lung Foundation sent a letter to all service users prior to the follow-up at 12 months to encourage completion. Service users were given the option of only providing data for the primary outcome. This was partly successful in having service users who had withdrawn from the service come forward to provide data at 12 months. To address the loss of data in the analysis, we employed a non-responder imputation as a conservative sensitivity analysis, where all participants lost to follow-up were classified as physically inactive. It is worthy to note that his approach is recognised in the literature to be overly conservative, particularly in behavioural interventions where missingness may not strictly equate to treatment failure. 33 As this sensitivity analysis is considered to give the most conservative estimate of minimum treatment effect, it may underestimate the true clinical benefit. 34 Our comparison of participants who completed the 12-month follow-up to those who were lost to follow-up demonstrated a higher proportion of males in the control group were lost to follow-up at 12 months than completed (65% vs. 35%), but gender was not a significant predictor of activity in the final adjusted models. Hence, while attrition was high, it was largely non-systematic and unlikely to have introduced significant selection bias on our physical outcomes. The possibility of survivor bias, however, cannot be entirely excluded.
Implications for future research and practice
The current study had relatively specific target populations and outcomes. The primary objective of this study dichotomised physical activity outcomes into active or inactive. Active Steps was a component of the ‘Movement for All’ programme, a strategic partnership between multiple health and social care charities in the UK and Sport England. This initiative (including the ‘We Are Undefeatable’ campaign) was designed to support adults with chronic disease to become physically active and rooted in UK national policies stating unquestionable health benefit or greatest return on public investment would be achieved by supporting the most inactive members of the community. 14 29 Hence, the current study targeted reduction of the number of people who would be defined as being physically inactive in the UK (completing less than 30 minutes of moderate-vigorous activity per week). Therefore, the success of the intervention in the current study may not be generalisable to all countries, which may use different definitions for physical inactivity. Challenges in the long-term follow-up of populations with lung disease, including those assessing physical activity, are common. 35 The interpretation of the long-term effects on physical activity in the present study was sensitive to participant attrition. The uncertainty of the effect at 12 month is likely attributable to a combination of a significant loss of statistical power and a decline in the intensity of behaviour change over time. The true effect of the behaviour change support provided in this study likely sits somewhere between our per protocol analysis and conservative sensitivity analysis. This highlights a dual challenge for any future remote behaviour change services; the potential need for additional strategies (between 6 and 12 months) to maintain long-term behaviour, and refined retention strategies to maintain the sample size necessary for long-term evaluation. This study demonstrates that charity-led remote support can be an effective strategy to initiate change in physical activity behaviour in adults with lung disease with robust effectiveness sustained for at least six months. Future services will need to focus on identifying and supporting participants at high risk of disengagement to bridge the gap between initial adoption and long-term maintenance.
Conclusions
Active Steps was an effective charity-led remote service to initiate changes in physical activity behaviour in the short-to-medium-term in adults with lung disease, but high participant attrition necessitates caution in interpreting longer term effects at 12 months. Changes in physical activity in people who engaged with the service coincided with clinically meaningful improvements in self-reported health and respiratory specific quality of life.
Supplemental material
Supplemental material - Remote behaviour change service for inactive adults with lung disease: A non-randomised controlled study
Supplemental material for Remote behaviour change service for inactive adults with lung disease: A non-randomised controlled study by Jones AW, Robinson H, Saunders M, Brewster A, Ridyard C, Smith M, Peel J, Shopland J, Wilson C, Dean A, Hinchliffe M, Siriwardena AN, Law G in Chronic Respiratory Disease
Footnotes
Acknowledgements
We would like to thank and acknowledge: all of the participants who took part in this study; Susan Frizzell, British Lung Foundation Active Steps and data teams for supporting data collection; Lincolnshire Community Health Services NHS Trust, Lindum Medical Practice, Nettleham Medical Practice, Spilsby Surgery, Glebe Practice and National Institute for Health Research Clinical Research Network East Midlands for supporting recruitment of the control group.
Funding
The delivery of the behaviour change service and an independent evaluation was funded by Sport England and the British Lung Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.