
Abstract
Background: Severe physical inactivity (SPI) in patients with COPD is associated with a poor prognosis. It is unknown whether there is a link between SPI and systemic inflammation, and if systemic inflammation in SPI changes following pulmonary rehabilitation (PR).
Methods: A prospective, observational study of patients referred for at least 7 weeks of PR comprising 2 h of exercise therapy and education twice weekly. At baseline and after PR, daily physical activity level (PAL) was measured with a validated activity monitor, SenseWear® as well as systemic inflammation: b-eosinophils, p-fibrinogen, p-CRP, s-IL-6 and s-CD 163. SPI was defined as PAL <1.4.
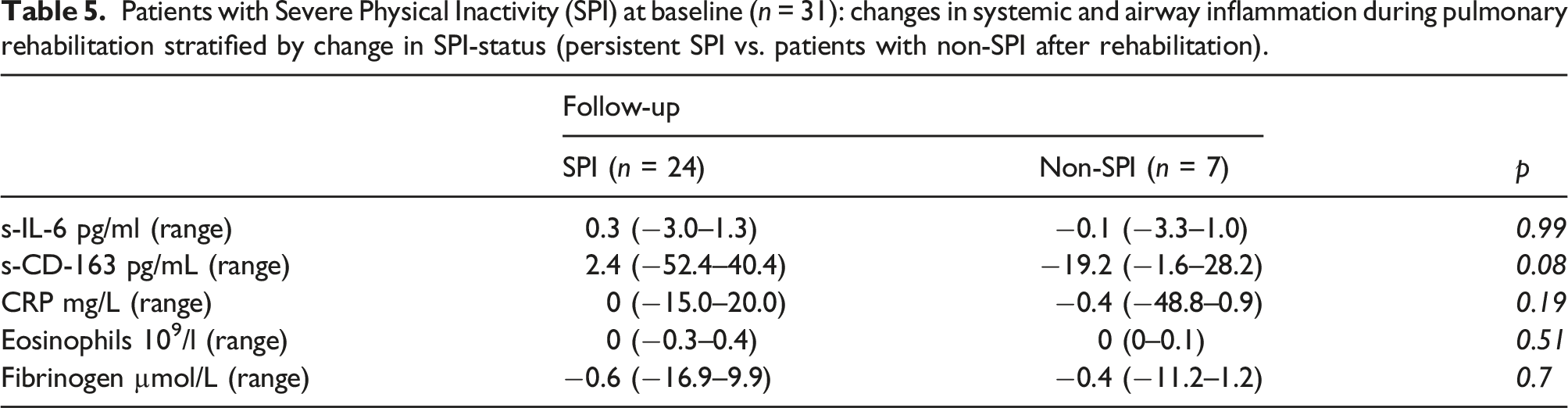
Results: At baseline, SPI was present in 31 of the 57 patients included, and 23% (7/31) improved to non-SPI after PR. We observed no differences between patients with SPI and non-SPI, except baseline plasma fibrinogen level was slightly yet significantly higher in patients with SPI (median 13.3 [6.2–23.6] vs 11.2 [6.5–16.7] µmol/l) but change in fibrinogen levels differed insignificantly between patients who improved to non-SPI at follow-up compared to patients with persistent SPI (−0.6 [−16.9–9.9] vs −0.4 [−11.2–1.2] µmol/l).
Conclusion: SPI in COPD appears not to be associated with a distinct inflammatory profile compared to less sedentary COPD patients attending pulmonary rehabilitation. Currently biomarkers have no role in the detection of SPI in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with sedentary lifestyle especially in advanced stages. A minority of patients with COPD are severely physical inactive (SPI), defined as a total daily energy expenditure/resting energy expenditure ratio <1.4. 1 SPI is inversely correlated to disease severity, measured as lung function decline, frequency of hospitalization and mortality in patients with COPD.2–4 In our previous paper, investigating the change in activity during pulmonary rehabilitation, we demonstrated, that patients with SPI does not improve as much from pulmonary rehabilitation as the general COPD population, 5 but the explanation for this remains unknown. Current evidence supports an association between reduced lung function and systemic inflammation as well as a possible link with comorbidities such as cardiovascular disorders, skeletal muscle dysfunction, diabetes, and osteoporosis.6,7 At stable condition, COPD is associated with elevated levels of systemic inflammatory markers such as leukocytes, eosinophils, CRP, IL-6, fibrinogen, and TNF-α.6,8–12 Lifestyle factors such as smoking, poor nutrition, low physical activity level (PAL) and obesity are known to increase systemic and/or local inflammation in COPD.10,13,14 The association between physical inactivity and systemic inflammation is of particular interest as it is present not only in COPD, but across a range of chronic conditions.15,16 As exercise therapy and other types of physical activities are known to be anti-inflammatory, 17 physical inactivity is a highly relevant treatment target. This is further substantiated by the fact that exercise therapy, typically as part of pulmonary rehabilitation (PR), improves health-related quality of life and exercise capacity in patients with COPD.18,19 As it is unknown, we aimed at investigating the relationship between the activity level and systemic inflammation and whether PR can reduce systemic inflammation in patients with SPI.
In this exploratory study, we hypothesized that patients with SPI would have increased systemic inflammation and that measurable improvements in PAL after PR – especially changing from SPI to non-SPI – would lead to a significant reduction in systemic inflammation.
Methods
Design
Previously, clinical data and study design has been published. 5 Briefly, this was a prospective, observational cohort study conducted in 2013–2014 at four PR units in Region Zealand, Denmark. The reporting adheres to the STROBE guidelines. 20
The study was approved by the Danish National Ethical Committee, and complied with the Declaration of Helsinki. Written and oral informed consent was obtained from all participants.
The study was registered at ClinicalTrials.gov (NCT01700296).
Participants
Patients referred for PR were included if they fulfilled the following eligibility criteria:physician-diagnosed COPD based on symptoms and spirometry; no exacerbations in the past 4 weeks prior to inclusion, ability to give informed consent, no life-threatening comorbidity (e.g. malignancy or severe heart failure), and no history of asthma.
Patient and public involvement
Patients gave informed written and verbal consent before study initiation. Patients were not involved in the design of the study. All patients who requested information on study results were provided with these after publication.”
Rehabilitation
The reporting of the PR adheres to the TIDieR guidelines. 21 PR was conducted according to Danish national guidelines as a multidisciplinary, non-pharmacological intervention using supervised exercise therapy and patient education. 22 Patients attended either one of three municipal rehabilitation centers or a hospital-based PR. The content of the PR was comparable but as this was an observational study, the duration of PR varied between sites from seven to 12 weeks. The PR consisted of two-hour sessions twice weekly: 1 hour of exercise therapy, equally distributed between endurance and strength training under supervision of a physiotherapist, and 1 hour of patient education by an assigned nurse or other relevant professionals e.g. dietitian.
Initially, 30 min of strength training was performed using weight training machines for the following muscles: pectoralis major, deltoid, biceps brachii, triceps and quadriceps. Patients performed 3 × 12 repetitions at 50–80% of one repetition maximum (1-RM). The 1-RM test was repeated halfway to re-establish the workload. Subsequently, 30 min of individually adjusted endurance training was performed at moderate intensity to level 14–15 on the Borg scale of perceived exertion. The endurance training included either cycling on an ergometer or walking on a treadmill. Education included disease-, nutritional- and pharmacological education in addition to smoking cessation assistance.
Outcomes
The patients were examined twice: at first day of PR (before the first rehabilitation session (baseline), and in the week after completing PR (follow-up).
Primary endpoint: Between-groups differences in change of inflammatory markers between patients with SPI at baseline who at follow-up still have SPI versus those improving to non-SPI.
Secondary endpoints
Baseline differences in inflammatory markers between patients with SPI versus non-SPI.
Protocol deviations
The current study deviates from our original protocol (clinicaltrials.gov number NCT01700296). Firstly, the Ethics Committee disapproved inclusion of a control group not attending the physician-requested PR. Secondly, we chose to examine the short-term outcomes as long-term systemic inflammation is affected by many non-COPD related factors, such as rhinitis, cardiovascular diseases, chronic liver disease etc., which we could not control or adjust for. Due to the short-term outcome the incidence of exacerbations (AECOPD) became unnecessary. As there was no control group, we decided to do an observational study with the primary outcomes physical activity (measured by the Sensewear) and systemic inflammation changes.
Basic measurements
Group characteristics (n = 57).

Objective measurement of physical activity including Severe Physical Inactivity
PAL was measured with an activity monitor (SenseWear© Armband, Bodymedia, Pittsburgh, PA) continuously worn for 7 days after each study visit. SenseWear© has previously been validated for use in COPD. 1 The activity monitor is worn on the back of the upper right arm at the level of the triceps. It assesses accelerations in two planes using a bi-axial accelerometer, and measures and stores skin temperature, near body temperature, heat flux, and galvanic skin resistance. Output from the SenseWear© includes total energy expenditure, daily time in sedentary-, light-, moderate- and hard activity as well as number of steps. SenseWear© is a wellvalidated multisensor in COPD.23–27 This activity monitor is worn on the back of the upper right arm at the level of the triceps and assesses accelerations in two planes using a bi-axial accelerometer. It measures and stores near body temperature, heat flux, skin temperature, and galvanic skin resistance. Weight and height data are entered for each patient. The SenseWear © collects data on average daily steps, average daily consumption of minutes in mild, moderate and hard activity, calorie consumption, average daily activity, average daily hours of sleep. SenseWear © measures the Physical Activity Level (PAL) which is the Total Energy Expenditure (TEE) divided with the Resting Metabolic Rate (RMR). Known as Severe Physical Inactivity (SPI): PAL <1.4.1,28
Activity is measured in Metabolic Equivalent of Task, MET, a unit of energy expenditure (kcal/kg/h).
In the current study, PAL was calculated as total daily energy expenditure divided by resting energy expenditure in kcal measured by the activity monitor. Based on a previous study, cut-off values for PAL were defined as PAL ≥1.70: active person, 1.40–1.69: sedentary person; and <1.40: SPI.29,30 Data from patients with ≥2 days of ≥90% wearing time were included.
Laboratory analyses
Leukocytes and eosinophils were measured in blood and CRP, IL-6, fibrinogen, and TNF-α in serum. We also measured serum CD163 as overexpression on lung alveolar macrophages may be involved in COPD pathogenesis. 31
Serum and plasma samples: 5 mL samples of both serum and plasma were collected in sterile tubes and centrifuged. The supernatant was stored at −800 C for later analysis of inflammatory markers IL-6, and CD 163. All biomarkers were measured at The Respiratory Research Unit, Bispebjerg University Hospital, using commercial ELISA kits (Human IL-6 and sCD163 Quantikine high sensitivity ELISA; R&D Systems, Minneapolis, MN, USA).
Blood samples: CRP (Dimension Vista, Siemens Healthcare Headquarters GmbH, Erlangen, Germany), eosinophils (Sysmex XE-5000, Sysmex Corporation, Kobe, Japan), and fibrinogen (STAGO, Triolab AS, Brøndby, Denmark) were measured at every visit. All blood samples were analysed at Naestved Hospital, Department of Clinical Biochemistry immediately after each PR-visit (Figure 1). Flowchart.
Sample size calculation
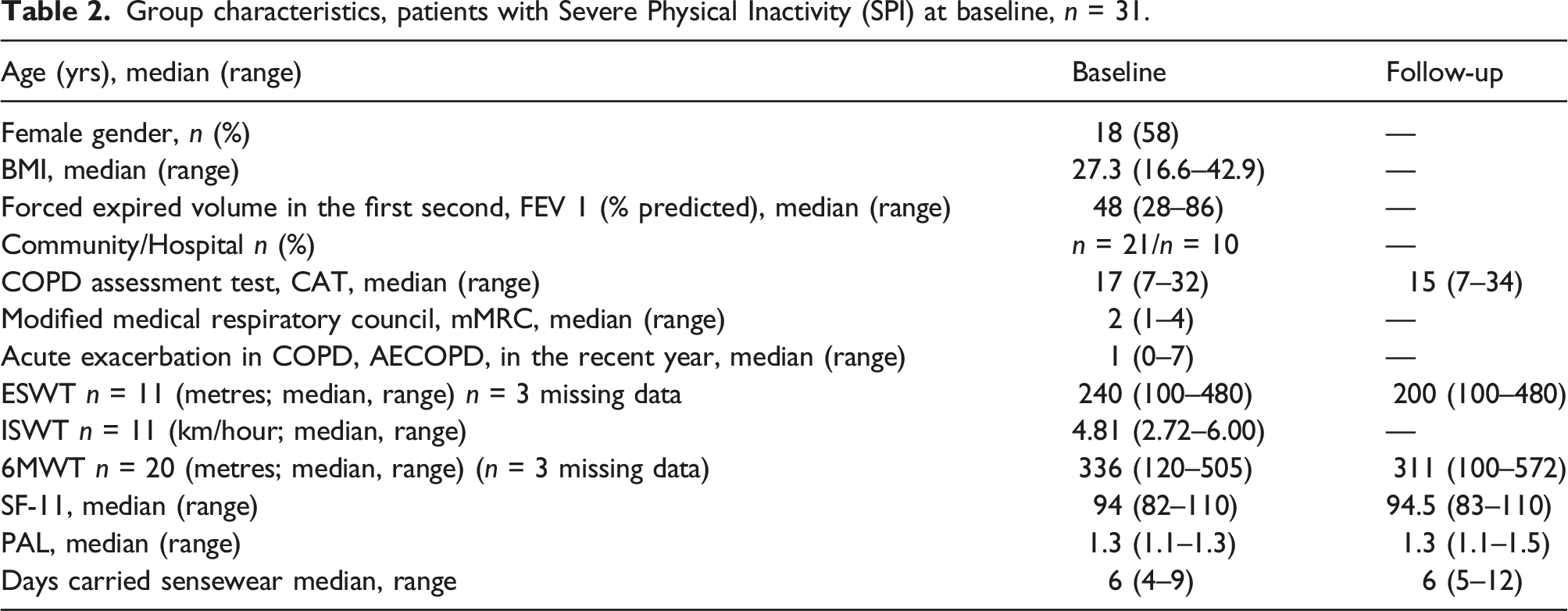
Group characteristics, patients with Severe Physical Inactivity (SPI) at baseline, n = 31.
Statistics
As data were not normally distributed, we used non-parametric statistics. Continuous data were presented as median (range), and categorical data as numbers (%). Differences were assessed using Wilcoxon signed-rank test (continuous data) resp. Chi2-test (categorical data). Kruskal-Wallis test for trend was performed for coherence between PAL tertiles and inflammation, and Spearman’s rho was used for correlation analyses. Statistical significance was defined as p < 0.05 and all analyses were performed using professional statistical software (STATA 14.1; StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
Results
Patients
In total, 31 patients out of the 57 patients were classified as SPI at baseline. After PR, seven of these patients (23%) became non-SPI, as they increased their daily level of objectively measured physical activity (PAL) to ≥1.4. A demographic table, previously published, has been added to provide context for the study results. 5 None of the study participants were treated with oral corticosteroids or antibiotics within 4 weeks prior to baseline or follow-up visits. Complete data sets of SenseWear© and inflammatory markers were available in 66–76% of patients: IL-6 68% (n = 40), CD-163 66% (n = 39), and fibrinogen, eosinophils and CRP 76% (n = 45).
All data presented are original data without imputation. All analyses were run with and without imputation, but no results changed from significant to insignificant or vice versa.
Inflammatory markers at baseline
Systemic and airway inflammation at baseline stratified by patients with Severe Physical Inactivity (SPI) (n = 31) or non-SPI (n = 20).


(a) Association between PAL and CD 163 from baseline to follow-up. (b) Association between PAL and IL-6 from baseline to follow-up.
In total, 20 (39%) were current smokers (median pack-years: 41), and 30 (59%) used daily-inhaled corticosteroids (ICS). We observed no association between ICS use, current smoking and level of inflammatory markers (data not shown).
Changes in inflammatory markers after PR
Physical Activity Level tertiles and inflammatory markers at baseline.

*chi2 >0.05 for trend.
Discussion
Patients with Severe Physical Inactivity (SPI) at baseline (n = 31): changes in systemic and airway inflammation during pulmonary rehabilitation stratified by change in SPI-status (persistent SPI vs. patients with non-SPI after rehabilitation).
In contemporary COPD management, inflammatory biomarkers play a limited role. Blood-eosinophil count guides the decision of inhaled corticosteroid in patients with frequent exacerbations
32
but no inflammatory biomarker has to date proven clinically relevant and valid concerning everyday COPD diagnosis, prognosis or disease management.32,33 COPD is a heterogeneous disease entity, which is managed clinically by addressing COPD phenotypes, eg. frequent exacerbators, eosinophil predominant, smokers, chronic bronchitis, emphysema, asthma-COPD overlap and more COPD.34–37 The role and composition of local and systemic inflammation differs between COPD phenotypes, so the phrase “enhanced chronic inflammatory response” in the 2016 GOLD definition of COPD has later been removed.
32
Our study is the first to investigate the inflammatory profile of patients with SPI in COPD. We found low and inert levels of inflammatory markers with little change during PR, even in patients with a significant improvement in daily physical activity level. A similar inert pattern has been reported in a study of PR for patients with COPD and cachexia.36,37 COPD-related sarcopenia and especially sarcopenic obesity is associated with short walking distance and increased systemic inflammation.37–40 We did not include data on body composition, hand-grip strength, leg circumference, timed up-and-go test, or other measures related to muscle strength but sarcopenia is a known risk-factor for physical inactivity in COPD.38,41 Studies investigating changes in systemic inflammation during PR in patients with COPD-related sarcopenia are therefore needed.
The literature on changes in systemic inflammation during PR is contradictory: some studies report no changes,39,42–44 whereas others show reduction in eg. IL-8, 45 IL-6, 46 and CRP 46 supporting that exercise is an efficient and inflammation lowering activity.15,16
However, systemic inflammation may derive from comorbid or transient causes such as asthma and infections. 32 We excluded recent exacerbations or asthma to avoid “contamination” of inflammation due to non-COPD causes or transient fluctuations. This may result in a relatively “low-inflammation” cohort of COPD patients as frequent exacerbators were unlikely to pass exclusion criteria but on the other hand increased the internal validity of the study.
An obvious short-coming is the small sample size and risk of a type II error, yet a statistically significant reduction in IL-8 during PR was demonstrated in an even smaller sample size. 45 Furthermore, inflammatory markers may vary over time but we included only two measurements, 12 and changes in physical activity may be to discrete to elicit a detectable inflammatory change.13,19,40 Yet this is the first study to explore systemic inflammation in COPD patients with SPI, and it suggests that SPI is not associated with a distinct pro-inflammatory profile, and that improved physical activity level in SPI was not associated with a reduction in systemic inflammation. Currently, biomarkers seems to have no role in the diagnosis or monitoring of SPI. Improving physical activity in this very sedentary cohort was possible for 23%. Future studies should identify methods to improve the outcome of PR in this susceptible subgroup accounting for needs and preferences of the individual.
Footnotes
Author’s Note
The study was registered at ClinicalTrials.gov (NCT01700296), ![]() . Registered in November 2012.
. Registered in November 2012.
Acknowledgements
We want to thank Palle Lyngsie Pedersen and the dep. of Clinical Biochemistry on Naestved hospital for help with analyzing the blood samples.
Authors contribution
MT has as a part of her PhD contributed substantially in all aspects of the work.
UBT has as a main supervisor of the PhD project also contributed substantially in all aspects, except data collection.
AL has made substantially contributions in the interpretations of data as well as having substantially revised the manuscript.
STS has made substantially contributions in the interpretations of data as well as having substantially revised the manuscript.
JL has made substantially contributions in acquisition and analysis of the laboratory samples.
All authors have read and approved the manuscript
Ethics approval and consent to participate
The study was approved by the Danish National Ethical Committee, and complied with the Declaration of Helsinki. Written and oral informed consent was obtained from all participants.
Availability of data and materials
Data from the current study is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Skou is associate editor of the Journal of Orthopaedic & Sports Physical Therapy, has received grants from The Lundbeck Foundation, personal fees from Munksgaard, all of which are outside the submitted work. He is co-founder of Good Life with Osteoarthritis in Denmark (GLA:D®), a not-for profit initiative hosted at University of Southern Denmark aimed at implementing clinical guidelines for osteoarthritis in clinical practice. Anders Løkke has, during the last 5 years, on one or more occasions served in an advisory board, as a speaker, as principal investigator and/or participated in education activities arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Orion Pharma, Pfizer and Teva. Additionally, Anders Løkke has received unrestricted research grants from Boehringer Ingelheim, Chiesi and Pfizer - all of which are outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was, as a part of a PhD project, supported by Naestved, Slagelse and Ringsted Hospitals’ Research Fund, and a 1-year scholarship from University of Southern Denmark. Financial contributions to equipment and laboratory testing from Moeller Foundation, Meyer scholarship the local Health Research Unit at Naestved Hospital (grant No N/A). Dr. Skou is currently funded by a grant from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement No 801790) and a program grant from Region Zealand (Exercise First).