
Abstract
Background
Individuals with early-stage non-small cell lung cancer (NSCLC) often show reduced exercise capacity and physical activity (PA) after surgery, with or without (neo-)adjuvant therapy. However, understanding of peoples’ lived-lives following lung cancer diagnosis and surgery remains unknown.
Objective
This study aimed to deeper understand how lung cancer diagnosis and surgery shape individuals’ daily lives within one to three months post-surgery.
Methods
Adults (18+) with stage I–IIIA NSCLC were recruited one to three months after surgery or (neo-)adjuvant therapy including radio-/chemo-/immunotherapy. A rapid ethnographic approach was used. Participants were observed at home during three two-hour visits, with a semi-structured interview during the last visit. Field notes and transcripts were thematically analyzed in Atlas.ti using a hybrid approach. Initial themes were deductively guided by the 14-domain TDF and inductively refined. Final themes were mapped onto the COM-B model.
Results
16 individuals (69% female; 69±7 years; 3820±2207 steps/day; 6±8 min/day moderate-to-vigorous PA; 44% received (neo-)adjuvant therapy) participated in home observations (86h total, range 4-6h) and a semi-structured interview during the last visit (383min total, range 16-44min). Four key themes were identified; 1) Physical consequences affecting daily life; 2) Emotional and social coping; 3) Motivation and barriers influencing PA and rehabilitation; 4) Gaps in education and guidance.
Conclusion
Lung cancer surgery (with or without (neo-)adjuvant therapy) causes physical, emotional, and social challenges that impair daily life. PA and engagement to rehabilitation is often limited by symptoms and contextual barriers. Tailored rehabilitation addressing individuals’ living conditions, physical, and emotional needs are considered crucial for recovery.
Keywords
Introduction
Lung cancer is the most commonly diagnosed cancer in men and the third most commonly diagnosed cancer in women worldwide. 1 Non-small cell lung cancer (NSCLC) is the most common subtype of lung cancer, accounting for approximately 85% of all cases. 2 Thirty-five percent of NSCLC individuals are diagnosed with early-stage (stage I-IIIa) NSCLC. 3 The preferred treatment option for early-stage NSCLC is lung resection, with or without (neo-)adjuvant chemo- and/or immunotherapy. 4 Impaired exercise capacity and physical activity (PA) are common in individuals following lung surgery for NSCLC and may negatively impact health-related quality of life (HRQoL), reflecting the influence of both disease- and surgery-related factors.5,6 7 Both are therefore considered important treatable traits for non-pharmacological interventions. 8
Individuals after surgery for NSCLC are potentially excellent candidates for rehabilitation programs. To date, moderate-to high-certainty evidence shows that structured exercise training programs combining aerobic and resistance exercises improve exercise capacity, quadriceps muscle force, HRQoL, and symptoms of dyspnea in individuals with NSCLC following lung surgery. 8 Interventions focusing on behavior change, as successfully applied in individuals with chronic obstructive pulmonary disease (COPD), could also provide valuable benefits to improve low levels of PA, alongside exercise training, in people with lung cancer. 9 Cancer survivors are recommended to engage in at least 150 minutes of moderate PA per week and return to normal daily activity as soon as possible following diagnosis and treatment. 10
Despite evidence supporting the role of rehabilitation, it remains grossly underutilized. 11 In individuals with chronic respiratory disease, barriers to perform exercise training or PA include travel issues, suboptimal scheduling, and other commitments (e.g., caring for others, work responsibilities, and social commitments), as well as cost, illness, and the impact of comorbidities. 12 Previous research in individuals with breast, prostate, or head and neck cancer has revealed similar barriers, along with cancer-specific symptoms and issues, such as fatigue, breathing difficulties, and pain, that can hinder the initiation and/or maintenance of exercise training or PA after treatment.13–15
However, many of these findings are based on interviews and may not fully capture the complexity of people’s daily lives, hiding deeper concerns that are not easily expressed. 16 As a result, current insights may only offer a limited view, making it difficult to design effective, person-centered solutions. To gain a deeper understanding of individuals’ lived experiences within a limited timeframe, this study employed a rapid ethnographic approach that allowed consideration of the clinical and contextual aspects of postoperative recovery. By spending time in people’s everyday environments, this approach allows us to observe what shapes their behaviours, routines, and decisions about PA and rehabilitation.
An in-depth insight into the impact of lung cancer diagnosis and treatment on peoples’ lived-lives is crucial to inform strategies that improve engagement in exercise, PA, and rehabilitation. 17 Therefore, this study aimed to explore how lung cancer diagnosis and surgery shape individuals’ daily lives within one to three months post-surgery, with or without (neo-)adjuvant therapy.
Methods
Study design
A rapid, flexible, and pragmatic ethnographic approach was used, informed by the Theoretical Domains Model (TDM). 18 A rapid ethnographic approach gathers rich, contextual insights over a short time frame (e.g., days to weeks), while still using core ethnographic methods like observations, interviews, and engagement in natural settings. 16 Three home observations (two hours each, one week apart) with informal conversations were completed and during the last visit, a recorded semi-structured interview (15–45 min) was conducted to explore key themes in more depth. Participants were specifically asked to describe perceived changes in physical function, symptoms, and activity levels compared with their pre-surgery status, to help differentiate limitations related to lung surgery from those associated with pre-existing conditions. Topics were predefined, according to the TDM, but adapted based on individual observations and conversations. To ensure consistency in data collection and reporting, all assessments and observations were conducted by the same investigator across all participants. This study was conducted and reported in accordance with the Standards for Reporting Qualitative Research (SRQR) (Supplement S1). 19 The study was approved by the ethics committees of Ziekenhuis Oost-Limburg and Hasselt University (NO. Z-2023064; B3712023000005) on 18/10/2023.
Participants
Adults (18+) with stage I–IIIA NSCLC were included one to three months after surgery or after (neo-)adjuvant therapy including radio-/chemo-/immunotherapy. Exclusion criteria were progressive/recurrent lung cancer, other malignancies (<2 years), performing structured exercise, non-independent living, psychiatric/cognitive disorders, or inability to understand Dutch. Individuals were recruited during post-treatment consultations and provided written informed consent. This study employed a purposive sample of sixteen individuals, with variation in sex, age, educational level, employment status, rehabilitation status (accepted/declined), and (neo-)adjuvant therapy (yes/no), to ensure the inclusion of diverse perspectives. 16
Data collection
Individual characteristics, the lived experiences of individuals, objectively measured physical activity, and patient-reported outcome measures were assessed (Supplement S2).
Data analysis
Individual characteristics, objectively measured physical activity and PROMs were analysed using IBM SPSS statistics version 28 (IBM Corp., Armonk, NY, USA). All data is presented as means ± standard deviation (SD), median [Q1; Q3] or percentages.
During observations, informal conversations arose naturally and were documented in field notes. Reflexive notes were kept during and after the observations to document researcher thoughts, assumptions, and evolving interpretations. A structured template was used to capture contextual details, reflections, and emerging insights. Semi-structured interviews were audio-recorded, transcribed using TurboScribe, and cross-checked. Field notes and interview transcripts were independently coded and analyzed in Atlas. ti by two researchers (SH, AJLM), and discrepancies were resolved through discussion. Quotes were translated by one researcher (SH).
The analysis process was regularly discussed within the research team for peer debriefing. A hybrid thematic analysis combined deductive guidance from the 14-domain TDF, 20 with inductive refinement as data collection progressed. Analysis began after initial observations and interviews, with field notes and transcripts analysed simultaneously to ensure a comprehensive understanding of the context and participant perspectives. Final themes were mapped onto the COM-B model. 21 Participants were invited to review their interview transcripts for accuracy (member checking).
Results
A total of 28 individuals with NSCLC who had surgery were screened, of whom nineteen individuals met the eligibility criteria and were contacted. Sixteen individuals agreed to participate and signed the informed consent, while three declined due to a lack of interest. Recruitment occurred between December 2023 and June 2024, with all participants completing three home observations and a recorded semi-structured interview (Figure 1). Consort diagram.
Individual characteristics
Demographic characteristics of individuals.

Note. Data are expressed as mean ± SD. Abbreviations: ID: Identification; F: Female; M: Male; BMI: Body Mass Index (kg/m2); Mean steps/day: Mean steps per day; MVPA: Moderate-to-Vigorous Physical Activity (min/day); RAL: Robot-Assisted Lobectomy; uVATS: uniportal Video-Assisted Thoracoscopic Surgery; Uni: Uniportal; LUL: Left Upper Lobe; RUL: Right Upper Lobe; RML: Right Middle Lobe; RLL: Right Lower Lobe; CLBP: Chronic Low Back Pain; COPD: Chronic Obstructive Pulmonary Disease. During the first observation, sex, age, self-reported height, and weight, smoking status, pack years, highest level of education, and employment were recorded. Cancer type, cancer stage (TNM 8th edition), medical treatment, days since medical treatment, and comorbidities were retrieved from the medical record. Post-operative rehabilitation uptake was assessed through self-reported data.
Lived experiences of individuals
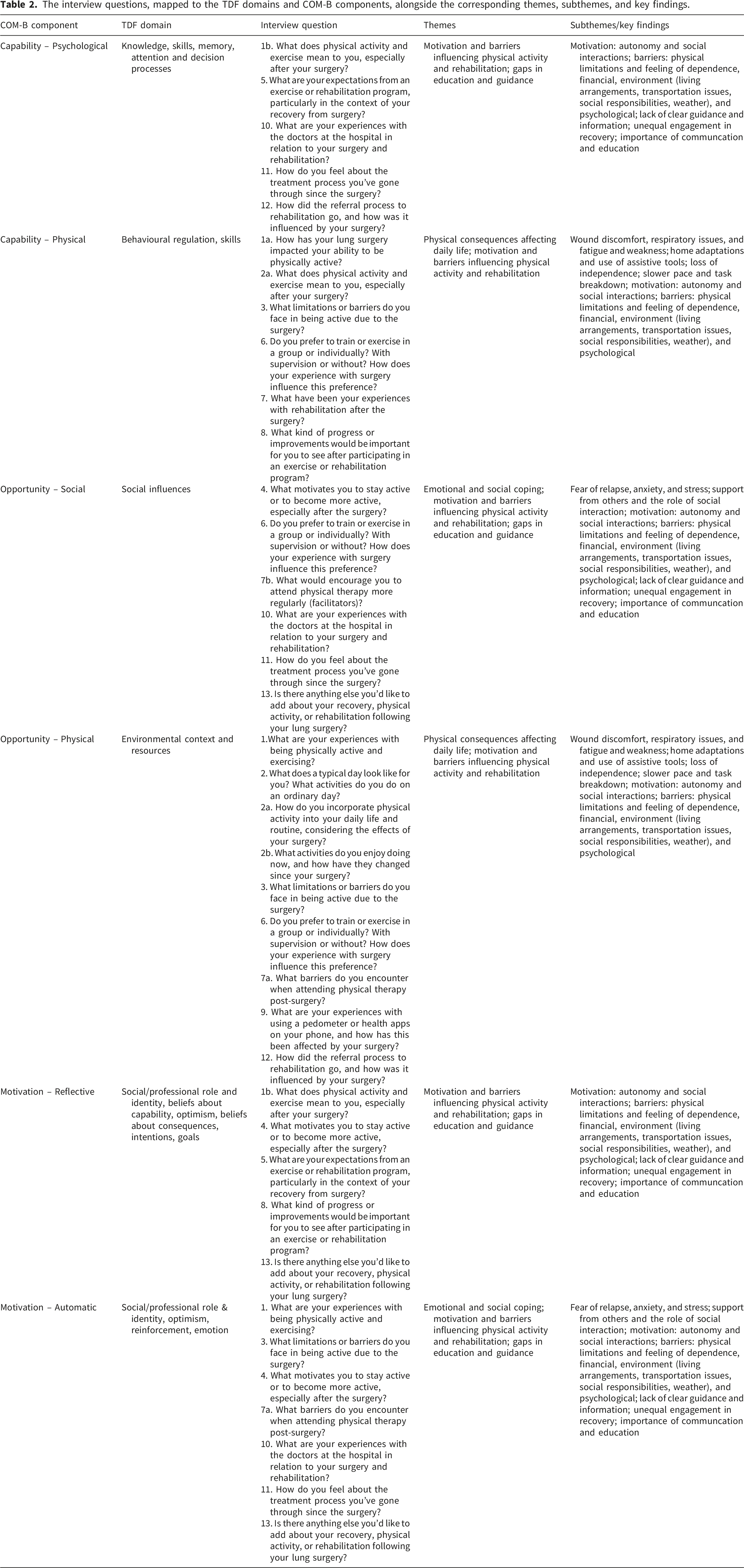
Four key themes emerged; 1) Physical consequences affecting daily life; 2) Emotional and social coping; 3) Motivation and barriers influencing PA and rehabilitation; 4) Gaps in education and guidance (Figure 2). The interview questions, mapped to TDF and COM-B, with themes, subthemes, and key findings, are further detailed in Table 2. Detailed observations and quotes can be found in Table 3. Representation of the four key themes identified through observations and semi-structured interviews. The interview questions, mapped to the TDF domains and COM-B components, alongside the corresponding themes, subthemes, and key findings. Overview of observations and individual quotes by theme and subtheme.

Physical consequences affecting daily life
Individuals described a range of physical consequences such as wound discomfort (pain, soreness, pulling sensation), respiratory complaints (shortness of breath, coughing), fatigue, and weakness that interfered with daily activities. One woman (P07) avoided walking outside since surgery, as cold air caused wound pain. This was also seen during the observations, as another participant (P03) struggled to reach a glass of water on a nearby table, and one woman (P01) limited cooking to twice a week because it required too much energy.
Many participants reported in interviews adapting their daily routines, such as pacing activities throughout the day or taking frequent rest breaks, or modifying their home environments, for example by rearranging furniture to minimize effort or using assistive devices to facilitate mobility and household tasks, in order to reduce discomfort. For instance, a small chair was used to reach cupboards, but post-surgery pain prevented one woman (P06) from using it, forcing her to stop storing essentials, such as tins of beans, within easy reach. She consequently shopped more often, which was difficult due to pain. Another participant (P10) moved his bed to the living room as stairs were unmanageable, while one woman (P01) avoided stairs by getting ready in her living room, keeping deodorant, perfume, and a mirror there, which restricted its social use.
Despite such adjustments, physical limitations hindered daily activities and exercise, increasing reliance on family or caregivers. Participants commonly reported avoiding stair climbing, window cleaning, reaching overhead, and lifting heavy objects like groceries. When tasks were performed independently, they were often observed to be broken into smaller steps, such as taking one plate at a time from the cupboard or leaving dishes on counters to put away later (P02). These prolonged efforts reduced energy for health-promoting behaviors, leading to more sedentary lifestyles.
Although some participants described improvements in symptoms and functional abilities across the three visits, observations showed that others maintained or increased adaptations, underscoring variability in recovery trajectories.
Emotional and social coping
Participants frequently expressed during interviews their reliance on loved ones for emotional comfort and practical support during recovery. Emotional responses such as fear, anxiety, and stress, often related to uncertainty about relapse, were commonly articulated and were also seen during observations. For example, one participant (P10) became emotional several times when discussing the future, seeking comfort from his wife, who provided reassurance through gentle words.
Observations further illustrated how social support functioned in daily life. One participant (P01), living on the first floor, remotely opened the door for visitors, unable to manage the stairs. Her downstairs mailbox was observed to be overflowing. She explained that she was waiting for her neighbour to collect the mail for her. While such support eased physical limitations, having others around also created responsibilities. In another home (P14), a crowded calendar filled with social visits, and household tasks suggested that social obligations restricted availability for PA and rehabilitation. This contrast illustrates how social ties could both enable and constrain recovery, depending on the nature of support and expectations.
While some individuals reported feelings of loneliness and insufficient support, others described finding strength and comfort through these social connections, highlighting the wide range of social experiences during recovery.
Motivation and barriers influencing physical activity and rehabilitation
During observations, many individuals showed strong motivation to regain autonomy. For example, one participant (P04) attempted to complete household tasks independently; when his wife offered to unload the dishwasher, he became visibly frustrated and declined assistance. This behavior aligned with interview statements expressing a desire to remain independent. While social interaction often encouraged activity, participants described how dependence on others or limited support could also act as barriers. One participant (P03) expressed a wish to gradually resume household tasks herself, pointing out areas she felt were inadequately cleaned by her husband or daughter, concerns that reflected her need for control and autonomy.
Participants reported several environmental and financial barriers to PA. Those living in social housing (P01, P02, P09, P13, P15, P16) described limited space and resources for rehabilitation, which was confirmed during observations of small or cluttered living environments. Environmental constraints such as stairs, transportation difficulties, and weather conditions were frequently mentioned. For example, one participant (P15) living in a small apartment struggled with stairs and limited space, which constrained indoor PA. In another case (P05), taking the bus to rehabilitation was possible, but she felt unsafe and unsure about the fare, often arriving exhausted. Another individual (P02) mentioned that environmental factors, such as bad weather, discouraged outdoor walking. Psychological challenges post-surgery, including fear of illness, particularly lung-related conditions like bronchitis (P01), also limited engagement.
Although several participants stated they felt confident exercising independently at home, observations revealed little evidence of structured or guided home-based rehabilitation. Exercise equipment was rarely observed, and limited space or unsuitable surroundings posed additional challenges. Although some mentioned wearables like step counters or smartwatches as motivational tools, only a few were actually seen using them. Participants noted that the recovery journey was often longer and more difficult than anticipated, highlighting the interplay of personal motivation, environmental factors, social support, and psychological barriers.
Gaps in education and guidance
Participants frequently reported insufficient guidance from healthcare professionals regarding safe activity, rehabilitation options, and recovery expectations. Observations reinforced these concerns, revealing environmental and safety risks such as loose rugs, narrow hallways, and cluttered spaces that increased fall risk. One participant (P11) described a misstep at a doorstep during the first week after surgery due to dizziness and weakness. These concerns, combined with a mismatch between perceived and actual ability, highlights the need for professional support in creating a safe recovery environment. However, many individuals reported receiving insufficient information about available services, which contributed to feelings of frustration and uncertainty. For instance, it was observed that one participant (P04) was unsure how to perform exercises safely or how to access local rehabilitation programs, resulting in avoidance of activity and waiting passively for her partner. She depended heavily on external support and showed less personal initiative.
Given the emotional burden of a cancer diagnosis, participants consistently emphasized during interviews that support from family and friends remained vital, with individuals often feeling more comfortable sharing concerns with loved ones.
Objectively measured physical activity
People wore the PA monitor for 5 ± 2 days, with an average wearing time of 827 ± 100 minutes/day. Nearly all participants (94%) fell below the recommended 7500 steps/day, averaging 3820 ± 2207 steps/day. Average sedentary time was 601 ± 105 minutes/day and time spent in light physical activity (LPA) averaged 220 ± 80 minutes/day. Engagement in moderate-to-vigorous physical activity (MVPA) was minimal, averaging 6 ± 8 minutes/day.
Patient-reported outcome measures
Patient-reported outcome measures.

Note. Data are expressed as median [Q1; Q3]). + Indicates reference values. * Indicates normative values.
Abbreviations; PA: Physical Activity; ESES: Exercise Self-Efficacy Scale; LASA: Longitudinal Aging Study Amsterdam – Lifestyle for Vital Ageing Scale; SRQ-E: Self-Regulation Questionnaire - Exercise; TAMPA: Tampa Scale for Kinesiophobia;.DASS-21: Depression, Anxiety, and Stress Scale - 21 items; MFI-20: Multidimensional Fatigue Inventory – 20 itemsy; mMRC: Modified Medical Research Council Dyspnea Scale; SF-36: Short Form-36; EORTC QLQ C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GH: General Health; SS: Symptom Severity; FS: Functional Status; EORTC-LC13: European Organization for Research and Treatment of Cancer Lung Cancer 13-item module; EQ-5D: EuroQol-5D.
Discussion
This ethnographic study uncovered complex, context-specific barriers and facilitators influencing PA and exercise after lung cancer surgery. Beyond known physical symptoms, environmental constraints, such as small living spaces, safety hazards, and limited access to rehabilitation resources, emerged as critical factors limiting activity engagement. Social support and individual motivation were important facilitators but often insufficient without tailored healthcare guidance. Importantly, the findings highlight that generic exercise recommendations may not align with individuals’ lived realities, emphasizing the need for personalized, context-aware rehabilitation plans that integrate individuals’ home environments and social circumstances to improve adherence and recovery outcomes after lung surgery for NSCLC.
The physical burden of lung cancer surgery is compounded by psychosocial challenges such as fear, anxiety, and uncertainty about relapse. Similar psychological distress has been documented across various cancer populations, where fear of disease progression or relapse can severely affect mental well-being.30,31 Additionally, individuals with NSCLC who had surgery report lower health-related QoL compared to healthy adults, with scores comparable to or slightly better than those with advanced COPD or pulmonary fibrosis. 32 This underscores the critical need for rehabilitation and ongoing support, which have proven benefits in improving quality of life in chronic respiratory diseases. 33
Although most participants initiated post-operative rehabilitation, this care was primarily delivered in community-based primary care settings rather than within specialized oncology rehabilitation programs. The limited number of attended sessions, combined with variability in program content and disease-specific expertise, may help explain why individuals continued to report uncertainty regarding safe exercise performance and self-management. Participants described several potential reasons for limited engagement, including a low perceived usefulness of supervised sessions, the belief that exercises could be performed independently at home, and variable access to physiotherapists with specific expertise in post–lung surgery care. These findings align with previous qualitative research indicating that individuals may perceive structured rehabilitation as insufficiently beneficial and prefer more flexible, self-managed exercise options. 34 Overall, these findings suggest that initiation of rehabilitation alone does not necessarily translate into sufficient perceived competence or knowledge, highlighting the need for more structured, tailored, and sustained guidance following lung surgery. In other populations, preference-based or home-based models, particularly in prostate cancer, often improve adherence compared with standard RCT formats, 35 while in other chronic conditions, structured, team-based programs combining exercise, education, and support can achieve excellent adherence (77%). 36 Additionally, the adoption of wearable activity trackers is limited by unfamiliarity, poor understanding of PA metrics, and lack of confidence-building strategies. Addressing these barriers requires integrated interventions, including home-based programs and PA tele-coaching.9,37,38
Despite nearly all individuals (94%) falling below the recommended 7500 steps/day, 39 they recognize the importance of PA (8/108,10) and show motivation to be physically active (8/105,8). However, confidence in engaging in PA is often low, as individuals are afraid of causing damage to the surgical wound or hindering their recovery. Exercise self-efficacy in this study aligns with previous findings where people with higher self-efficacy were more physically active, while those with lower self-efficacy had a higher risk of not achieving the recommended 7500 steps/day. 38
Notably, some participants felt fully recovered despite ongoing limitations, highlighting the need for education to prevent underestimation of rehabilitation needs. Reassurance that symptoms like pain or breathlessness rarely indicate relapse, and that exercise is safe, is crucial. However, many participants (7 out of 16) had only primary education. This lower educational attainment is often associated with reduced health literacy. Limited health literacy could affect individuals’ understanding of postoperative care instructions, rehabilitation options, and recommendations for PA, potentially influencing their experiences and engagement with rehabilitation. Therefore, tailored education, incorporating simplified and visual educational materials, social support, and practical strategies, preferably delivered face-to-face by specialized professionals and reinforced through repeated explanations using teach-back techniques, may enhance individual engagement in rehabilitation.40,41 However, current rehabilitation models may not suit all individuals: home-based programs can be impractical in small spaces, and centre-based care may be inaccessible. Addressing these challenges may require flexible delivery models, such as transport support or delivering rehabilitation in local community settings.
Strengths and limitations
A major strength of this study was its detailed qualitative approach, combining in-home observations with semi-structured interviews to capture lived experiences. The TDF provided a structured framework for analyzing behavioral influences on PA and rehabilitation. Home visits also offered unique insights into their recovery environment and eliminated the need for travel, including a more diverse sample, and reducing selection bias. Integrating informal observations with detailed field notes helped mitigate recall and social desirability bias. Finally, conducting observations at multiple times and days allowed a comprehensive understanding of daily routines.
Limitations include potential observer effects, as participants may have altered behavior or environment. Several participants also had multiple comorbidities that may have influenced physical function, PA and recovery. A high comorbidity burden is commonly reported in individuals undergoing lung cancer surgery, 42 reflecting the clinical complexity of this population. While participants were prompted to focus on lung surgery–specific changes, the influence of pre-existing conditions cannot be fully excluded. Observations during home visits and structured assessments were interpreted in relation to each participant’s baseline functioning to minimize misattribution. Further, focusing on early post-surgical recovery may not capture longer-term challenges. Continuing to wear PA monitors after interviews may have influenced activity, though inactivity remained common. Despite purposive sampling, diversity in gender, employment, and educational level was limited due to recruitment constraints. As a result, our findings predominantly reflect the experiences of individuals with similar sociodemographic characteristics and may underrepresent perspectives related to different work demands, socioeconomic contexts, or access to rehabilitation and support services.
Future recommendations
Interventions for lung cancer survivors should address their specific physical, social and emotional challenges related to exercise and PA. Providing the right knowledge and tools can improve engagement, adherence to rehabilitation, and long-term recovery.43–45 Although education about rehabilitation is crucial, it is often underused due to gaps in clinical pathways, inconsistent delivery, and a lack of focus. Referrals to specialized rehabilitation are sometimes unclear, causing delays or missed care. Practical strategies to overcome barriers to rehabilitation and PA could include home-based adaptations to facilitate exercise, tele-coaching to provide remote guidance and support, transport assistance for attending sessions, and individualized guidance from healthcare professionals to ensure exercises are safe and appropriate for each individual. Implementing such strategies may enhance adherence, engagement, and overall recovery outcomes.
Conclusion
Lung cancer surgery (with or without (neo-)adjuvant therapy) causes physical, emotional, and social challenges that impair daily life and engagement in PA and rehabilitation. Despite motivation, PA and engagement to rehabilitation is often limited by symptoms and contextual barriers. Tailored, integrated rehabilitation addressing individuals’ living conditions and their physical and emotional needs are crucial for recovery.
Supplemental material
Supplemental material - The lived experiences of individuals with early stage non-small cell lung cancer following lung surgery: A rapid ethnographic approach
Supplemental material for The lived experiences of individuals with early stage non-small cell lung cancer following lung surgery: A rapid ethnographic approach by Sarah Haesevoets, Anouk J. L. Muijsenberg, Dries Cops, Samantha L. Harrison, Maarten Criel, David Ruttens, Marc Daenen, Martijn A. Spruit, Heleen Demeyer, Chris Burtin in Chronic Respiratory Disease.
Supplemental material
Supplemental material - The lived experiences of individuals with early stage non-small cell lung cancer following lung surgery: A rapid ethnographic approach
Supplemental material for The lived experiences of individuals with early stage non-small cell lung cancer following lung surgery: A rapid ethnographic approach by Sarah Haesevoets, Anouk J. L. Muijsenberg, Dries Cops, Samantha L. Harrison, Maarten Criel, David Ruttens, Marc Daenen, Martijn A. Spruit, Heleen Demeyer, Chris Burtin in Chronic Respiratory Disease.
Footnotes
ORCID iDs
Ethical considerations
The study was approved by the Institutional Ethics Committee of Hospital East-Limburg and Hasselt University (NO. Z-2023064; B3712023000005, dd. 18 October 2023).
Consent to participate
All participants gave written informed consent before data collection began.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by a grant of Bijzonder Onderzoeks Fonds (BOF21KP15).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.