
Abstract
Background
Chronic respiratory disease burden in Nepal is high, although data from the Terai (lowlands) is limited.
Methods
Through a community outreach programme in Mechinagar, 3398 adults (mean age 49.6 years, 59% female) were recruited to complete spirometry and questionnaires to determine prevalences of airflow obstruction, breathlessness (MRC dyspnoea score ≥3) and self-reported chronic lung disease. Multivariate logistic regression examined associated demographic and lifestyle factors.
Results
Prevalences of airflow obstruction (15%) and breathlessness (13%) exceeded self-reported chronic lung disease (8%). Age (odds ratio = 1.06, 95% confidence interval = 1.05-1.07), body mass index (BMI) per 1 kg/m2 (0.90, 0.88-0.93), physical inactivity (1.95, 1.07-3.84) and no formal education (1.46, 1.14-1.88) were associated with airflow obstruction. Smoking was only associated with airflow obstruction in females (1.90, 1.22-2.94) and adults ≥40 years (1.40, 1.05-1.86). Age (1.04, 1.03-1.05), airflow obstruction (2.43, 1.85-3.18), and male sex (0.63, 0.49-0.80) were associated with breathlessness. Only in females was breathlessness associated with BMI (1.08, 1.05-1.12) and mixed biomass use (2.65, 1.39-4.85). In men, labour/farming/agriculture work (3.30, 1.12-14.20) or unemployment (4.39, 1.43-19.30) was associated with breathlessness.
Conclusion
There is likely underdiagnosis of chronic lung disease in the Terai. Addressing smoking, educational disparities, physical inactivity and environmental pollutant exposure are public health priorities to improve respiratory health in the region.
Introduction
Chronic respiratory diseases contribute disproportionately to morbidity and mortality in lower-middle-income countries (LMICs). 1 Indeed, these countries account for 90% of chronic obstructive pulmonary disease (COPD) deaths. 2 Smoking, along with household, ambient and occupational pollutants, creates a milieu that at least partly explains the substantial burden of chronic respiratory diseases in LMICs. 3
Nepal, an LMIC in Southeast Asia with a population of ∼30 million, had the highest age-standardised mortality rate from chronic respiratory diseases in the Global Burden of Disease Study 2019. 3 COPD was also found to be the country’s second leading cause of death from non-communicable disease. 4 As in other LMICs, the burden of chronic respiratory disease in Nepal has been attributed to smoking as well as often unregulated household and ambient air pollution, although these exposures vary based on gender and geographical location. 5
In rural areas, the use of biomass fuels for cooking, often in poorly ventilated homes, may pose a significant risk factor for respiratory health that disproportionately affects women.6,7 Conversely, in urban areas, notable risks include ambient air pollution: driven by traffic, industrial activity and urbanisation – as well as occupational exposure to airborne pollutants.8,9 In 2019, the Nepal Health Research Council reported that 28% of men and 8% of women smoke, with even more exposed to passive smoking at home or in the workplace. 10 Poverty, inadequate access to healthcare and limited health literacy also contribute to the burden of chronic respiratory disease in Nepal. 5
Nepal’s diverse topography can be divided into the Himalayas, the middle hills, and the Terai (Lowlands), each with differing climates and health challenges. However, most published lung-health data from Nepal come from single-site studies in areas such as Pokhara and Bhaktapur (Himalayas and middle hills).11,12 These local snapshots cannot be extrapolated nationwide, and they leave the Terai – the country’s most industrialised and populated region 13 – largely uncharted. Given the limited literature on lung disease in Nepal despite its alarming prevalence and impact, 5 bridging this geographical evidence gap is essential to develop a country-wide picture of the burden of respiratory morbidity and prevention strategies to combat it.
This study aimed to assess respiratory health and identify associated risk factors as part of a community outreach programme in the Eastern Terai region of Nepal.
Methods
Study design
This was a community-based cross-sectional study as part of the Kidney, Hypertension, Diabetes and Cardiovascular diseases (KHDC) programme for prevention, early detection and management based in Eastern Nepal (Dharan and surrounding districts). The programme involves awareness sessions and door-to-door visits to encourage people living in the community to attend screening visits at public places near their homes and undergo various diagnostic tests. All households in the vicinity were informed about the screening opportunity through several channels, including community leads, to ensure that all those living in the area had an equal opportunity to attend. The programme has been running since 2003, but in 2019, a pulmonary component was added (KHDC-P), led by the B.P. Koirala Institute of Health Sciences (BPKIHS) in collaboration with the Geneva University Hospitals. This was conducted in Mechinagar municipality, the largest municipality in the Jhapa district, Koshi province of Nepal. Adults aged ≥20 years attending screening visits (integrated in the awareness sessions) were invited to participate in this study. Individuals were ineligible if they had lived in the screening district for <6 months, had a contraindication to pulmonary function testing, or were deemed unable to perform spirometry. During the study visit, participants completed questionnaires to determine sociodemographic factors, respiratory symptoms and self-reported prior diagnoses of chronic lung disease, and also completed a spirometry assessment to assess lung function.
Ethical approval
Ethical approval was provided by BPKIHS (Ref. No. 310/076/077-IRC). All participants provided written informed consent.
Sociodemographic factors
Age, sex, tobacco smoking (never, former, current), education (yes: at least primary level education, no: no formal education), physical activity (<30 min/day, 30-59 min/day, ≥60 min/day), house type (pucca: permanent construction, semi pucca: mixed permanent and non-permanent materials, Kachcha/tin/wood: non-permanent materials), work setting (labourer/farm/agriculture, office/business, services, house, none, other) were assessed by questionnaire. Cooking fuel (mixed biomass, clean fuel) was also assessed by questionnaire, but was only available for a subset of participants. Height and weight were measured (barefoot), and body mass index (BMI) was calculated from body mass (kg) divided by height squared (m2).
Respiratory outcomes
Oxygen saturations were recorded using a pulse oximeter. Spirometry was performed by trained clinicians using either NDD EasyOne Air or MIR portable handheld spirometers following ERS/ATS guidelines. 14 Both pieces of equipment were calibrated using a 3-L syringe following the manufacturer’s guidelines. All participants repeated the lung function test at least three times. The clinicians conducting spirometry were trained to the standard of the Spirometry 2019 update from ATS and ERS. 15 The training included aspects such as pre-spirometry assessment, conduct of spirometry, interpretation and calibration. All traces were checked for quality control by trained clinicians, and usable readings, as per ATS/ERS guidelines were included in the analysis.14,15 Forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio were measured. Predicted FEV1 was based on South Asian reference values. 16 Airflow obstruction was defined as FEV1/FVC<0.7. 17 Breathlessness was graded using the MRC Dyspnoea Scale (1-5), and scores ≥3 were classed as breathless. 18 Chronic bronchitis was defined as the presence of cough and phlegm production for at least 3 months, according to the chronic bronchitis questionnaire. 19 The COPD Assessment Test (CAT) was used to assess the impact of respiratory symptoms on participants’ lives. 20
Statistical analyses
Descriptive statistics for participant demographics and respiratory outcomes were presented as mean and standard deviation for continuous variables and number and percentage for categorical variables. To assess the association of the exposure variables and respiratory outcomes, logistic and linear regressions were used for binary and continuous outcome variables, respectively. The a priori confounders were age, sex and smoking status. For each exposure, univariate analysis was performed to determine the unadjusted odds ratio for logistic regression or the beta (β) coefficient for linear regression. Exposures that had statistically significant univariate associations were added to a multivariate model. Backward elimination was used to determine the final adjusted model, whereby the variable with the highest p-value was removed in a stepwise process until all variables included demonstrated a significant association. Confounders determined a priori were included in the adjusted model irrespective of their statistical significance. Sex-stratified analyses were also conducted using the same variables from the adjusted model, along with any additional variables that showed a significant interaction with sex in univariate analyses. Confounders/exposures included age, sex, smoking status, BMI, house type, recruitment site, education, physical activity, work setting and cooking fuel for all respiratory outcomes. Because of the large number of individuals with missing data for cooking fuel (due to its later addition), its associations with respiratory outcomes were analysed separately in a subset (n = 1386), and only a priori confounders were included in the adjusted model. The presence of airflow obstruction was treated as an additional exposure variable for breathlessness, a CAT score ≥10 and chronic bronchitis. Associations between smoking and work setting, as well as between airflow obstruction and breathlessness with self-reported prior diagnosis of chronic lung disease, were assessed using Chi-squared tests. Statistical significance was accepted at p < 0.05 (i.e., 95% confidence intervals not crossing 1.00). All statistical analyses were performed using
Results
Participant demographics as mean (SD) or N (%).

Not all percentages add up to 100 due to rounding.
Smoking prevalence by occupation
As shown in OLS Table 1, the work setting with the highest proportion of current smokers was in the services (26%), followed by labour, farming or agriculture (23%).
Respiratory outcomes
Respiratory outcomes as mean (SD) or N (%).

Not all percentages add up to 100 due to rounding.
For the subset with available cooking fuel data, respiratory outcomes are presented in OLS Table 2. The prevalence of respiratory outcomes was similar between this subset and the main sample.
Associations between self-reported chronic lung disease, airflow obstruction and breathlessness
A large proportion of those with airflow obstruction (70%) had no self-reported prior diagnosis of chronic lung disease (OLS Table 3). Similarly, a large proportion with breathlessness (67%) were also not previously diagnosed (OLS Table 4). Notably, many with airflow obstruction (70%) were not breathless (OLS Table 5).
Factors associated with airflow obstruction
Factors associated with airflow obstruction (FEV 1 /FVC <0.7).

Significant associations (p < 0.05) are highlighted in bold.
aAdjusted model includes recruitment site as a covariate.
bin variable column denotes a significant interaction effect with sex in unadjusted model.
Factors associated with breathlessness
Factors associated with breathlessness.
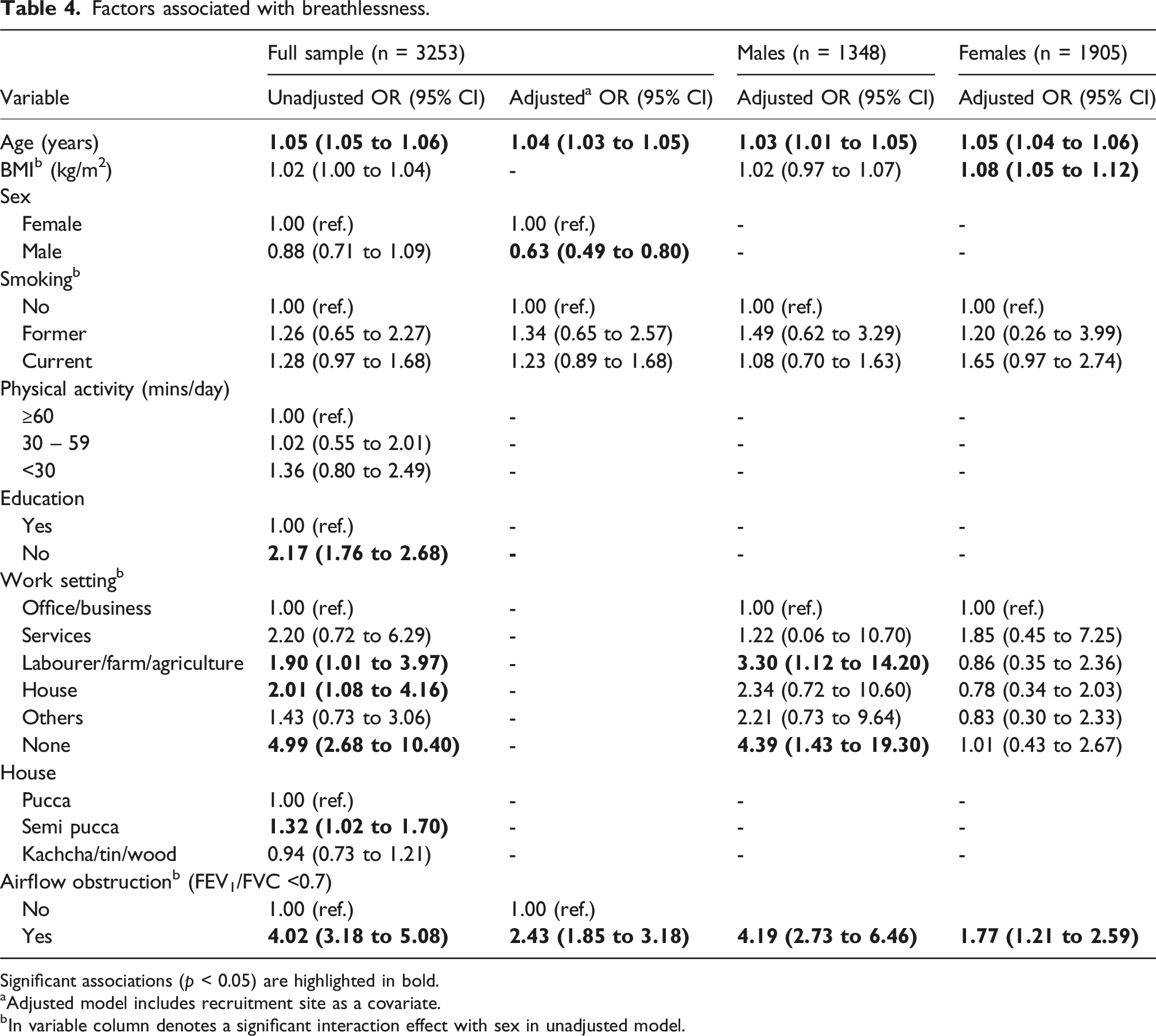
Significant associations (p < 0.05) are highlighted in bold.
aAdjusted model includes recruitment site as a covariate.
bIn variable column denotes a significant interaction effect with sex in unadjusted model.
Factors associated with a CAT score ≥10
Factors associated with a CAT score ≥10.
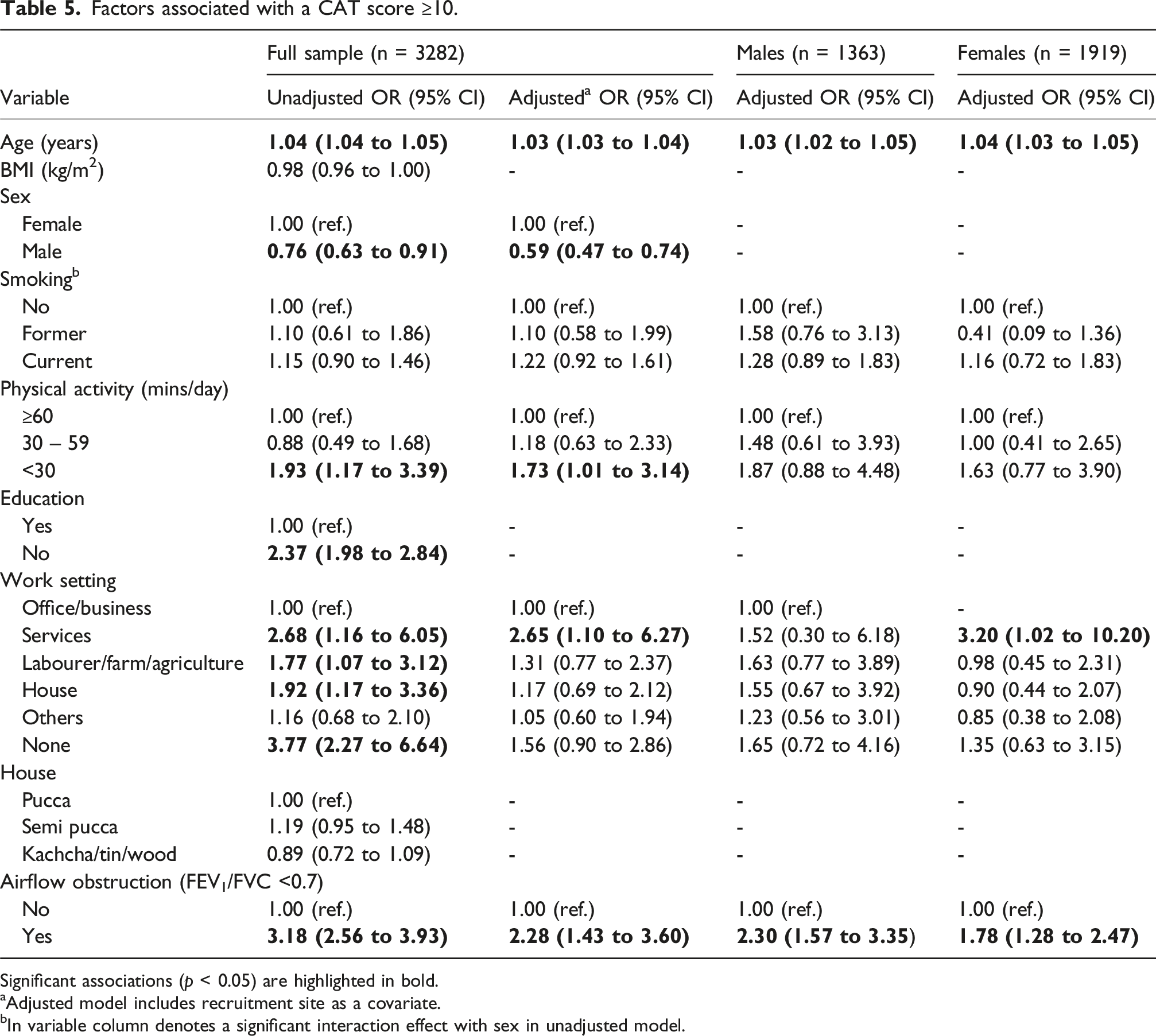
Significant associations (p < 0.05) are highlighted in bold.
aAdjusted model includes recruitment site as a covariate.
bIn variable column denotes a significant interaction effect with sex in unadjusted model.
Factors associated with chronic bronchitis
In the final adjusted model, age (OR = 1.04, 1.02 to 1.05) and airflow obstruction (2.35, 1.60 to 3.45) were associated with significantly higher odds of reporting chronic bronchitis, while males had significantly lower odds (0.66, 0.46 to 0.94) of reporting chronic bronchitis than females (OLS Table 6).
Factors associated with FEV1 % of predicted value
Age (β = −0.002, 95% CI = −0.002 to −0.001), male sex (−0.03, −0.04 to −0.01) and no education (−0.04, −0.07 to −0.004) were associated with a lower FEV1 % of predicted value, whereas BMI (0.003, 0.001 to 0.005) was associated with higher values (OLS Table 7).
Association of cooking fuel with respiratory outcomes
Of the 1386 individuals who had data for cooking fuel, 1279 (92%) used clean fuel and 107 (8%) used mixed biomass. Univariate analyses revealed that individuals who used mixed biomass were not at significantly higher odds of having airflow obstruction (1.04, 0.56 to 1.81) than those who used clean fuel sources (reference group). Individuals who used mixed biomass were at significantly higher odds of breathlessness (2.14, 1.29 to 3.43), and the odds remained significantly higher (2.17, 1.29 to 3.55) after additional adjustment for confounders defined a priori (age, sex, smoking status). Individuals who used mixed biomass were not at significantly higher odds of having a CAT score ≥10 (1.55, 0.94 to 2.47) or chronic bronchitis (1.60, 0.65 to 3.41). There was no significant association between cooking fuel type and FEV1 % of predicted (β for mixed biomass = −0.04, 95% CI = −0.08 to 0.01, p = 0.11).
There were no significant interaction effects between cooking fuel and sex on any respiratory outcomes. However, sex-stratified analyses showed that, compared to those using clean fuel, females using mixed biomass had significantly higher odds of breathlessness (2.65, 1.39 to 4.85), whereas the association in males was not significant (1.41, 0.53 to 3.35).
Discussion
This study assessed associations of potential risk factors with indicators of respiratory health in the Eastern Terai region of Nepal. Airflow obstruction and breathlessness were identified in a notable proportion of the community, including many of those who did not have a self-reported prior diagnosis of chronic lung disease. Several modifiable risk factors were identified, including smoking, which was associated with airflow obstruction in individuals over 40 years old.
The proportion with airflow obstruction is comparable to previous work; however, direct comparisons should be made with caution due to differences in methodologies, age group, and occupational and environmental exposures across regions.11,12,21 A large proportion of participants were breathless/had airflow obstruction without a prior diagnosis, suggesting underdiagnosis. Although this issue has been previously documented elsewhere in Nepal, 11 this study highlights that even in the Eastern Terai region (which generally has better geographical accessibility to public health facilities than the northern, mountainous areas) 22 underdiagnosis may still be a concern. As many with airflow obstruction were not breathless and showed only mild airflow obstruction (pre-bronchodilator), the impact of the airflow obstruction classification in the study population should be interpreted with caution. The prevalence of chronic bronchitis in the study population is also in line with previous research, published over 40 years ago. 21
As expected, smoking, a major risk factor for COPD, 23 was a significant predictor for airflow obstruction. Independent of age group, smoking was a risk factor for airflow obstruction in females but not males, in line with evidence that females are more susceptible to tobacco smoke. 24 Smoking prevalence varied by occupation, suggesting opportunities for smoking cessation initiatives in certain workplaces. A lack of education – an indicator of low socioeconomic status 25 – was associated with a greater odds of airflow obstruction, in line with previous findings. 11 Lower educational status is associated with risk factors such as smoking, exposure to air pollution, and limited access to healthcare, which may explain the association.26–28 Low physical activity was also associated with greater odds of airflow obstruction. Although reverse causation is possible, Bédard et al. provided causal evidence for a protective effect of physical activity on respiratory health in smokers. 29 Increased promotion of physical activity in Nepal may be warranted, especially for smokers and those exposed to air pollution.
The morbidity is depicted by both the large proportion with breathlessness and poor health status. Airflow obstruction was understandably a key risk factor for breathlessness. Sex-specific risk factors included a higher BMI in females, and in males, an occupation related to labour, farming or agriculture (likely due to pollutant exposure). The same occupational link may have been harder to detect in women because fewer of them worked in those roles, thereby reducing statistical power.
Sex was associated with several respiratory outcomes in this study. Females were more likely to report breathlessness and chronic bronchitis. Although the interaction between sex and cooking fuel was not statistically significant, sex-stratified analysis revealed a significant association between cooking fuel and breathlessness in females only, due to disproportionate exposure to biomass pollutants.6,7,30,31 The smaller sample for which cooking fuel data was collected may have led to reduced statistical power, thus explaining the lack of a significant interaction effect.
Addressing the burden of respiratory disease in Nepal requires a robust public health plan. Although there has been some progress in tobacco control through introducing advertising bans and other initiatives, policy analyses indicate weak implementation of tobacco control policies. 32 Greater taxation, stricter enforcement of bans, and improved access to cessation services are needed to strengthen tobacco control. 32 Public health efforts to accelerate the transition from using biomass to clean energy are also warranted, given its association with breathlessness in females in this study and its widespread use nationally. 33
This study has limitations. The cross-sectional assessment restricts the ability to establish causality. Although key confounders were adjusted for, residual confounding may still influence findings. For example, extrapulmonary causes of breathlessness, such as cardiovascular disease were not analysed. Other pulmonary causes, such as restrictive breathing patterns can also contribute to breathlessness. There is also a risk of selection bias, as certain individuals (e.g., those who are more health-conscious) may have been more likely to attend screening visits. Further, the total number of individuals invited for screening was not recorded, preventing a calculation of response rate and limiting our insight into the representativeness of the sample. The % predicted FEV1 values were calculated with equations for the wider South Asian population, not Nepal-specific norms, so slight misestimation is possible; nonetheless, these equations are the best reference currently available. 16 Only smoking status was adjusted for, and information on the extent of tobacco smoking would have enabled more robust adjustment for smoking-related confounding. Physical activity was assessed by self-report, which is susceptible to recall error and social desirability bias, and is more likely to capture deliberate rather than incidental activity. 34 Furthermore, performing postbronchodilator spirometry would have allowed for greater clinical diagnostic utility. Amongst the strengths, spirometry was conducted by trained personnel using strict quality assurance protocols and calibration, ensuring accurate assessment. By recruiting from a wide range of sites, the study’s sample is more geographically representative. Participants covered a broad range of occupations, although representation from office/business posts and the service-sector was limited, particularly amongst women.
In conclusion, this study reports considerable respiratory morbidity and likely underdiagnosis of lung disease in the Eastern Terai region of Nepal. It highlights potential public health priorities for the region, including improving physical activity, supporting smoking cessation, and reducing educational disparities and environmental pollutant exposure.
Supplemental material
Supplemental Material - Lung health in the Terai region of Nepal
Supplemental Material for Lung health in the Terai region of Nepal by Malik Hamrouni, Sanjib K Sharma, Om P Kurmi, Prajwal Gautam, Suman Lohani, Ujwal Gautam, Sigiriya A Perone,Olivia Heller, Ian P Hall, Tricia M McKeever, Charlotte E Bolton in Chronic Respiratory Disease
Footnotes
Acknowledgements
We thank the following for their assistance in the study’s conduct, oversight and management: Mamit Rai, BP Koirala, the Department of Internal Medicine, BPKIHS; KHDC-P research team; the Community Volunteers and Geneva University Hospitals.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for the pulmonary component was from Global Challenges Research Fund and NIHR Nottingham Biomedical Research Centre. The KHDC was supported by funding from Geneva University Hospitals.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IPH is in receipt of research funding from the Wellcome Trust and holds an NIHR Senior Investigator Award. He has undertaken advisory board work for GSK. All other authors declare no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.