
Abstract
Introduction
Effective management of pulmonary exacerbations (PEx) in cystic fibrosis (CF) is essential to minimise lung damage and reduce morbidity and mortality. Spirometry, the standard tool for lung function assessment in adult people with CF (pwCF), has limitations. Forced Oscillometry Technique (FOT) is an effort-independent method that assesses small airways disease and has been validated in other respiratory conditions. This study evaluated the feasibility and acceptability of implementing FOT during treatment for PEx in adult pwCF.
Methods
Twelve adult pwCF underwent FOT and spirometry at the start and end of PEx treatment, and at clinically convenient intervals. FOT was also measured before and after physiotherapy-directed airway clearance. A questionnaire assessed patient satisfaction with FOT.
Results
All patients had spirometry below baseline at PEx onset and small airways dysfunction on FOT. Treatment was associated with improvements in median FEV1pp (5.1%, p = 0.050) and X5 (0.2 cm H2O/L/s, p = 0.023), with a significant association between FEV1pp and X5 (p = 0.004). There was no significant FOT change after airway clearance. Patients rated FOT more favourably than spirometry.
Discussion
FOT is feasible, well-tolerated, and may complement spirometry in assessing adult pwCF during PEx. Further studies are warranted.
Introduction
Cystic fibrosis (CF) is a genetically inherited, life-limiting disease, characterised by chronic pulmonary infection and inflammation. Pulmonary exacerbations (PEx) of CF associated bronchiectasis are associated with progressive lung damage, increased patient morbidity and mortality, and decreased quality of life. 1 Whilst prevention, early detection, and treatment are crucial in minimising progressive loss of function in lung tissue and improving patient survival, there are no universally agreed methods of monitoring clinical response to treatment nor guiding treatment modalities and therapy duration. 2 This uncertainty is further complicated by the advent of cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapies, which have improved clinical outcomes and also challenged the current definitions and management of PEx. 3 Monitoring of lung function is the mainstay of disease assessment with spirometry, particularly Forced Expiratory Volume in 1 s (FEV1), currently the gold standard method in both acute and chronic care outpatient settings. 4 FEV1 is used as an objective marker to assist clinical decision-making during treatment for a PEx. However, it has been noted that FEV1 lacks sensitivity to detect changes in the small airways, which represent the site where CF lung disease and exacerbations begin.2,5 Furthermore, forced expiratory manoeuvres are unpopular in people with CF (pwCF) when unwell as they often stimulate coughing, especially in the early phase of a PEx. 6 Alternate methods to objectively assess pulmonary function in response to therapeutic interventions during PEx, including efficacy of airway clearance techniques (ACTs) are needed, but none have been integrated into routine clinical practice to date. 7
The Forced Oscillometry Technique (FOT) offers a user friendly, effort-independent method, which assesses small airway disease and has been validated in other fields of respiratory medicine. 8 This method assesses lung resistance and reactance as a measure of large and small airways disease and has been demonstrated to reflect anatomical and biochemical changes in the diseased CF lung.9,10 Whilst not integrated into routine medical practice, oscillometry has been demonstrated to reflect clinically relevant changes in paediatric patients with CF in the community and during treatment of a PEx.11–14 In adult pwCF, oscillometry has been sparsely studied but has potential as a promising technique for advancing the understanding and assessment of lung disease. 8 To our knowledge, there has been limited research into the utility of FOT during the treatment of PEx in adult pwCF, particularly in the era of CFTR modulator therapies. 15 This pilot study aimed to assess the feasibility of the practical implementation of FOT measurements in adult pwCF over the course of treatment for a PEx, and pre and post the delivery of physiotherapy supervised ACTs during a PEx. We also assessed the acceptability of FOT measurement in pwCF, to further evaluate its potential utility as a routine measurement that could be deployed in this clinical scenario.
Materials and methods
Study design
We conducted a prospective, single-centre study between September 2023 and January 2024. Consecutive adult pwCF treated for a PEx by the Adult Cystic Fibrosis Centre at The Prince Charles Hospital were evaluated for inclusion. This study was approved by the Metro North Health Human Research Ethics Committee (Project ID: 95639). All individuals in the study provided written informed consent prior to participating.
Participants
All patients aged 18 years or older, with a confirmed diagnosis of CF and able to perform lung function tests were considered eligible for our study. 16 PEx was defined by the Fuchs criteria, and all participants were deemed to require intravenous antibiotic (IVAB) treatment by the attending medical team. 17 Patients were excluded if they were unable to perform standard lung function testing, were considered to have severe underlying CF or were experiencing complications of PEx which would limit involvement in the study.
Data sources/measurements
Clinical management of PEx was guided by the treating medical team. Data on patient characteristics, treatment type and duration, clinical progress, and routine spirometry and laboratory measurements were obtained from the medical record.
Lung function tests
To assess conventional changes in lung function over the PEx treatment course, spirometry was assessed within 48 h of admission and prior to discharge. Spirometry measurements (raw values, % predicted, z-scores) were performed by trained staff per ATS/ERS guidelines or on home devices in instances where pwCF would perform spirometry without supervision but are familiar with correct technique.18,19 Forced Oscillometry Technique was performed by trained staff and measured within both 48 h of admission and prior to discharge. Measurements were performed on a TremoFlo C-100 Airwave Oscillometry System, and analysed by the TremoFlo Airwave Oscillometry Software, according to the 2020 European Respiratory Society guidelines. 20 To assess the effectiveness of physiotherapy supervised airway clearance, FOT was performed immediately pre- and post-physiotherapy at intervals of 48–96 h during the admission. For pwCF who were managed with IV ABx in the community, our usual standard of care was to admit the subject for at least 48 h for re-education and then discharge home to complete a week of home-based therapy before clinic review. In this setting, spirometry and FOT was performed on admission and again at completion of therapy. FOT parameters measured in this study included resistance at 5 Hz (R5), difference between R5 and resistance at 20 Hz (R5-20), reactance at 5 Hz (X5), resonant frequency (Fres) and total area of reactance (AX). Oscillometry results were considered in their raw values, z-score and in reference to published fixed cut-off values for small airways disease.21–23
Satisfaction surveys
To assess feasibility of FOT assessments in the PEx setting, pwCF completed a satisfaction survey adapted from the validated ‘Feeling of Satisfaction with Inhaler’ (FSI-10) questionnaire. 24 This adapted tool consisted of 10 items rated on a 7-point Likert scale, assessing factors such as ease of use, comfort, and perceived usefulness. In addition, participants rated their overall satisfaction with each testing modality. The survey was not validated but provided exploratory insight into patient experience with the FOT measurement compared to spirometry.
Statistical methods
Continuous variables were summarised as mean ± standard deviation (SD) or median and interquartile range (IQR) as appropriate. Categorical parameters are presented as frequency and percentages. Within-patient change in spirometry and FOT measures from admission to discharge and pre- and post-airway clearance were tested using Wilcoxon signed-rank test. Distributions and associations of interest were inspected and explored using histograms, boxplots, and scatter plots. Changes in FOT measures over the PEx treatment course were assessed using linear mixed effects models fitted with fixed effects for time and ACT (pre/post) and patient-level random intercepts. Standard errors were corrected for the small sample using the Kenward-Roger correction. Associations between FEV1 (percent predicted) and FOT measures were assessed using linear regression models with cluster-robust standard errors. Normality of residuals was assessed using inverse normal quantile plots. Statistical analysis was performed using IBM SPSS V.30.0 (SPSS, Chicago, IL) and Stata version 18 (StataCorp, College Station, TX).
Results
Participants and descriptive data
Baseline patient characteristics (n = 12).

CFTR: Cystic Fibrosis Transmembrane Conductance Regulator; FEV1: forced expiratory volume in 1 s; BMI: Body Mass Index; CFRD: Cystic Fibrosis-related Diabetes; CFLD: Cystic Fibrosis-related Liver Disease.
Treatment for PEx occurred in the inpatient setting for 10 (83%) patients and predominantly in the outpatient setting for 2 (17%) patients. Median length of IVAB treatment was 13 (11–14) days. All patients received at least two Pseudomonas aeruginosa targeting IVABs with 10 (83%) patients receiving tobramycin, five (42%) piperacillin-tazobactam, four (33%) meropenem, four (33%) ceftazidime, and two (17%) aztreonam. Interestingly, seven (58%) patients had concomitant viral infections as the precipitant to the PEx.
Lung function by spirometry and oscillometry measures (n = 12).

FEV1: forced expiratory volume in 1 s; R5: respiratory resistance at 5 Hz; R5–20: difference in respiratory resistance at 5 and 20 Hz; X5: respiratory reactance at 5 Hz; AX: respiratory reactance area; Fres: resonant frequency.
aBaseline defined as routine lung function performed immediately prior to PEx.
As FOT is not routinely utilised in our centre, no prior oscillometry data were available for our cohort. However, on admission the majority of our cohort had evidence of small airways disease, based on previously published cut-off values (Table 2).
Admission versus discharge lung function measures
Lung function measures over the study period.

Within-patient change in respiratory function measures from admission to discharge and pre- and post-airway clearance tested using Wilcoxon’s signed-rank test with values presented as median (IQR). FEV1: forced expiratory volume in 1 s; R5: respiratory resistance at 5 Hz; R5–20: difference in respiratory resistance at 5 and 20 Hz; X5: respiratory reactance at 5 Hz; AX: respiratory reactance area; Fres: resonant frequency.
aMedian change calculated from individual differences.
Pre- versus post-physiotherapy supervised ACTs
Median oscillometry measures prior to and following physiotherapy supervised ACTs were conducted for 11 patients and are presented in Table 3. Median time between paired measures was 4 (3, 4) days. There was no evidence for a significant reduction in airway resistance, reactance or resonant frequency following physiotherapy supervised ACTs.
Association over time and between measures
Regression modelling exploring change in measures over admission and effects of physiotherapy supervised ACT.

aEffect estimates derived from random intercept mixed effects model (n = 40 observations on 12 patients).
Results of linear regression analyses exploring the associations between FOT measures and FEV1 (percent predicted).

a95% confidence intervals derived using cluster-robust standard errors. (n = 40 observations on 12 patients).
Patient satisfaction
Patient satisfaction assessment of FOT as a method of measurement. a
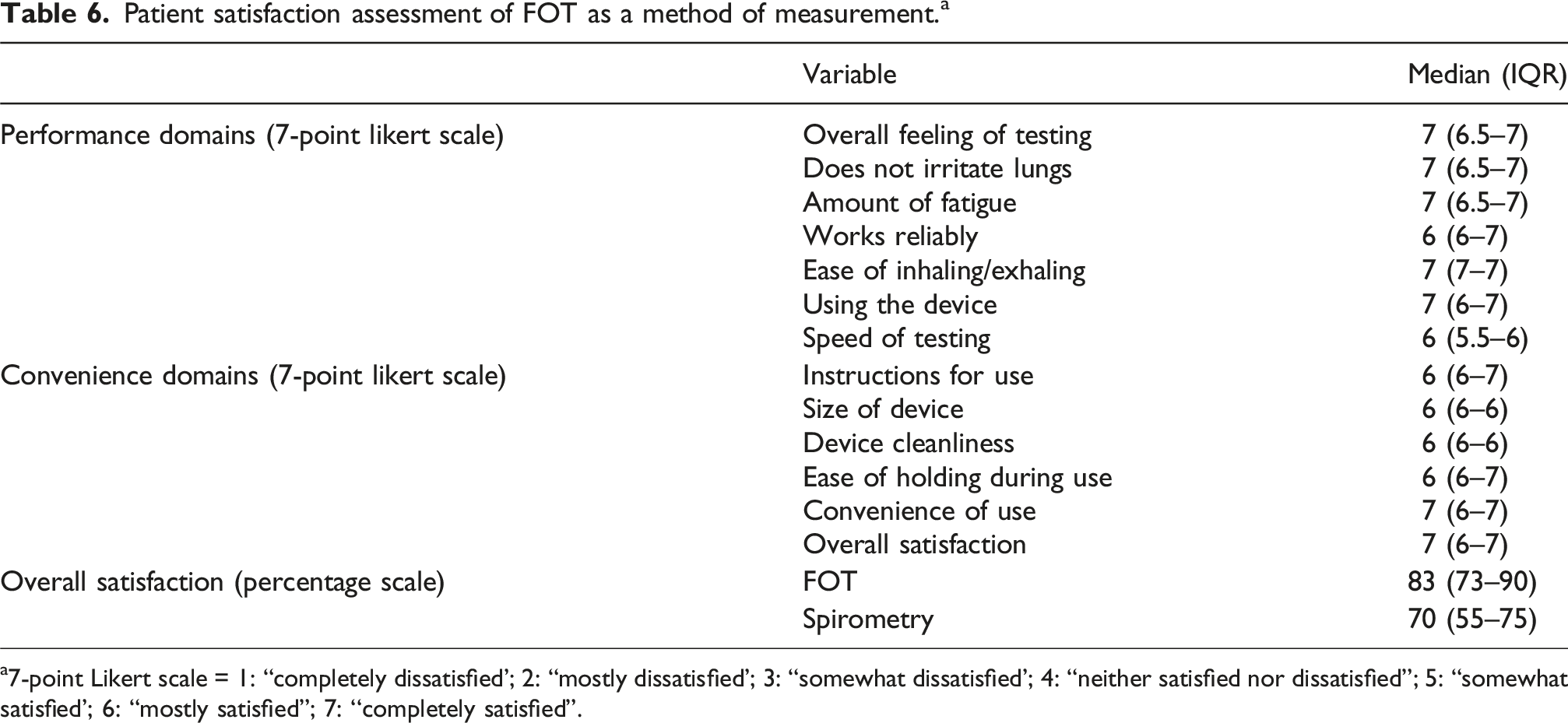
a7-point Likert scale = 1: “completely dissatisfied'; 2: “mostly dissatisfied'; 3: “somewhat dissatisfied'; 4: “neither satisfied nor dissatisfied”; 5: “somewhat satisfied'; 6: “mostly satisfied”; 7: ‘‘completely satisfied”.
Discussion
Whilst spirometry is currently the gold standard tool for respiratory measurements in adult pwCF, it is not without limitation. 26 Oscillometry offers a complementary measure of respiratory pathophysiology in CF and non-CF diseases of the airway, but FOT’s role in the assessment and management of adults with CF remains to be confirmed. 8
Our pilot study was conducted on a heterogenous cohort of pwCF undergoing IVAB treatment for a PEx. At the initiation of treatment, FEV1 was reduced from baseline values when well in all patients and improved overall with treatment. However, at completion of treatment, FEV1 had not returned to baseline in the majority of patients, which could be related to the high prevalence of respiratory viruses in our cohort and increased airway inflammatory response as a consequence. Oscillometry measures demonstrated evidence of small airways disease in the majority of patients on admission and these changes had not normalised by the end of IVAB. Persistent abnormalities in respiratory reactance were the most notable across the cohort, which implies persistent small airways disease. None of the oscillometry measures changed significantly after physiotherapy supervised airway clearance techniques. For measures of lung function across the course of PEx treatment, there was a significant improvement in FEV1 percent-predicted and X5, and a trend towards improvement in R5-20. Improvement in these oscillometry measures suggest an improvement in small airways disease with PEx treatment. This was further confirmed with regression modelling, which demonstrated a statistically significant correlation between FEV1 percent predicted and X5 over the treatment course. There was also a potential association between FEV1 and oscillometry measures of AX, and Fres, but this needs to be confirmed in a larger study.
Patient satisfaction with FOT as a method for airway function assessment was extremely high across all assessed domains in our study. In comparison to spirometry, patients generally expressed a preference for FOT, which scored higher in an overall satisfaction measure. In addition, our research team found FOT measurements to be operator and user friendly, easy to deliver and overall well tolerated by all patients.
Studies of oscillometry in pwCF are limited, with sparse analysis in an adult population. 8 Oscillometry has been shown to correlate with spirometry in older children with CF and to worsen during PEx before returning towards baseline following effective treatment.27,28 In adult pwCF oscillometry measures demonstrate an increased total and peripheral resistance and more negative reactance in comparison to healthy controls.9,10 Oscillometry findings in our cohort are comparable to that described in existing studies in adult pwCF, providing validation of our findings.9,10,15,29 Whilst retrospective analysis has suggested that oscillometry may have a role in the early identification of PEx our study is the first to demonstrate a potential role in monitoring improvement with treatment for PEx. 15
High quality objective measures of AWC in pwCF are lacking. 7 There is some suggestion that oscillometry measures of resistance and reactance improve with autogenic drainage in both children and adult pwCF.29,30 As a direct measure of the physiological benefit of ACTs there is conflicting evidence in paediatric subjects with a suggestion that coughing and diaphragmatic breathing exercises may increase measures of resistance.31–33 However, our study did not demonstrate any significant change in oscillometry with physiotherapy supervised ACTs which may reflect the small study numbers, variations of ACTs used amongst subjects, timing of FOT measurement or patient associated factors not accounted for in our study. In addition, ACTs primarily target proximal mucous plugging in proximal airways and clearance of occlusive plugs may result in the ventilation of previously obstructed airways, thus revealing underlying small airway pathology.20,34 Furthermore, mucus plugging itself is strongly associated with small airway dysfunction and effective clearance may unmask these abnormalities, with an apparent worsening of FOT parameters post-ACTs.35,36 This could add nuance to the use of FOT as a measure of ACT and could perhaps represent a useful marker of treatment effectiveness in the hands of experienced physiotherapists.
Our results are exploratory and subject to study limitations. Firstly, the small sample size limits statistical analysis, confidence, and generalisability. However, as discussed above, our findings are in line with similar studies suggesting our cohort is representative, adding confidence to our results and suggesting feasibility for further research. Secondly, as our hospital does not routinely utilise oscillometry measures in clinical practice there were no baseline measures for our study subjects, limiting assessment of oscillometry findings to that occurring over the course of PEx treatment. Thirdly, we did not assess oscillometry in the context of different ACT methods and chose to allow patients to employ their usual techniques, thus potentially limiting the opportunity to demonstrate the utility of oscillometry, as the patients’ techniques may have in fact been ineffective, thus compromising our assessments. Fourthly, as has been noted within the literature, a sizable portion of our cohort were identified to have viral co-infections. 37 There are conflicting reports that the decline in lung function in pwCF suffering a PEx with viral co-infection may be of lesser magnitude than with bacterial associated PEx, but that the decrement in FEV1 may persist for a prolonged period after the acute viral illness.38–40 Finally, no complementary clinical and biochemical measures of response to PEx treatment, nor clinical outcome measures were assessed as part of this study.
The diagnosis of PEx is difficult in pwCF and similarly, determining the efficacy of treatment in hospitalised patients is also challenging. There are limited tools to guide early detection of PEx, initiation or duration of antibiotic therapy, or inpatient versus outpatient therapy. 3 Such conundrums have become more pertinent in the era of CFTR modulator therapy where PEx are less likely to meet historical definitions, yet may continue to result in progressive lung injury and functional decline in the longer term. 41 There is developing evidence that oscillometry measures may be more sensitive than spirometry in the early identification of exacerbation in asthma and chronic obstructive pulmonary disease. 8 FOT monitoring during a PEx in pwCF may provide clinically relevant information to guide duration of therapy. A decline in measures could indicate a worsening of small airway disease, as an early marker of disease deterioration, prompting an escalation of therapy. Evidence of persistent small airway disease may guide decisions on adjunct therapy such as bronchodilators, corticosteroids or antibiotics. In stable pwCF a noted change from baseline could inform early escalation or initiation of therapy.20,34–36
Our study demonstrates the feasibility for oscillometry measures to monitor treatment in adult pwCF admitted with PEx, but further prospective research is required before reliable integration of oscillometry can occur in the clinical setting. Whilst there are correlates between oscillometry and spirometry measures, larger studies are required in adult populations to further assess oscillometry measures in the early detection of PEx and treatment response. To better evaluate small airway changes with ACTs in adult pwCF, oscillometry should be assessed in comparison to emerging measures such as multiple breath washout, biomarkers of airway inflammation and advanced imaging techniques of lung ventilation including volumetric CT and functional MRI.
Conclusion
Our pilot study confirms that oscillometry is a well-tolerated tool that could be used to assess small airway function in adult pwCF undergoing IVAB treatment for PEx. Oscillometry could thus provide valuable additional information, beyond currently utilised objective measurements such as spirometry, about pulmonary pathophysiology in adult pwCF. Further research is needed in adequately powered studies to determine whether oscillometry is superior to spirometry in guiding therapeutic decision making in the management of PEx in adult pwCF. This pilot study also highlights the need for studies of oscillometry as an objective measure sensitive to small airway disease that could be used to optimise and personalise management in the era of ETI therapy where physical symptoms are less prominent, but sub-clinical airway injury may still be occurring.
Footnotes
Author note
Dr James Nolan, corresponding author, has moved to a new institution since completing the research.
Acknowledgments
This research was supported by a Novice Investigator grant awarded by The Prince Charles Hospital Foundation.
Ethical considerations
This study was approved by the Metro North Health Human Research Ethics Committee (Project ID 95,639) on 13/07/2023.
Consent to participate
All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: This work was supported by The Common Good Foundation Novice Investigator Grant (NI2023-23).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.