
Abstract
Time until the subsequent exacerbation (PEx) in cystic fibrosis (CF) is a significant health outcome and one of the significant end points in clinical trials. Risk factors associated with shorter time until the next exacerbation (TUNE) have not been reported. This is a prospective study. TUNE was the number of days from the end of intravenous (IV) antibiotic treatment of a PEx until the day of start of IV antibiotics for the following PEx. Factors assessed were age, gender, site of treatment, CF-related diabetes (CFRD), allergic bronchopulmonary aspergillosis (ABPA) and infection with Pseudomonas aeruginosa (PA). In addition, we examined parameters obtained at day 14 of treatment including forced expiratory volume in the first second (FEV1), body mass index, CF respiratory symptom score, C-reactive protein (CRP) and serum cytokines. A total of 170 exacerbations in 58 adult CF patients (27 female), mean (SD) age 25.8 (6.7) years were analysed. When analysing individual variables, patients with lower FEV1, greater symptom score and higher CRP at the end of exacerbation were associated with shorter TUNE. Patients with ABPA and CFRD had a shorter TUNE than those without. When applying multiple regression analysis, factors associated with shorter TUNE were older age and lower day-14 FEV1 values. Shorter periods until the following PEx are expected in older CF patients and those with lower FEV1 at the end of course of treatment. When these risk factors are present, there may be a justification to take therapeutic steps to increase the time until the following PEx.
Introduction
Pulmonary exacerbations (PExs) in cystic fibrosis (CF) are important feature of the disease. 1,2 Frequent CF PExs influence the quality of life 3 and are associated with reduced lung function. 4
Most severe CF PExs are treated with 14-day course of antibiotics, 5 with the majority of CF patients experiencing symptomatic improvement and increase in lung function tests at the end of the course. But the duration of this improvement differ amongst patients.
Time until the next exacerbation (TUNE) is clinically important for patients. It has also been identified as a primary end point in clinical trials. 6,7 Factors associated with a shorter TUNE have not been previously assessed.
In a cross-sectional study involving CF patients from the South and Southwest of England, we previously demonstrated that lower forced expiratory volume in the first second (FEV1), chronic infection with Pseudomonas aeruginosa (PA) and CF-related diabetes (CFRD) were associated with frequent need for intravenous (IV) antibiotics for PExs. 8
Since then we conducted a 3-year longitudinal research programme on CF PExs in adult CF patients in our unit. This research allowed the evaluation of selected outcome measures in the management of PEx. 9 Comprehensive data including demographics, CF-related complications, and characteristics of CF PExs at the point of presentation and throughout the course of management were recorded. In addition, for patients who had more than one PEx, data on the precise number of days until the following exacerbations were available. This allowed the opportunity to investigate the risk factors associated with shorter TUNE.
Our hypothesis was that several factors would contribute to shorter TUNE. These included old age, poor lung function tests, CF-related complications and residual symptoms and clinical signs at the end of treatment. This article describes the testing of this hypothesis.
Patients and methods
The research programme was a prospective research with a 2-year recruitment period and a 1-year follow-up (last follow up in July 2010). This programme was approved by the Southmead Research Ethics Committee (Bristol, UK). The objective of the programme was to examine the value of intensive input of the CF team during home management of CF PExs in adult CF patients.
Patients’ selection
All CF patients treated and managed in our centre by the CF multidisciplinary team only were invited to take part. Those who signed an informed consent prior to being involved in the study were enrolled. The medical records were kept within a safe environment in the department and therefore complete data were available for most patients. Inclusion criteria were consenting adult CF patients who had at least one PEx in the year prior to the study and who received full care in our unit. Exclusion criteria were mild exacerbations requiring oral antibiotics, episodes in which IV antibiotics were initiated for reasons other than PExs, patients with chronic infection with Burkolderia cenocepacia, patients on a shared care treatment programme with neighbouring CF units and post-lung transplant patients. Approximately 25% of our patients needed extension of treatment beyond day 14. Patients who received more than 2 antibiotics for PExs or those who needed extending antibiotics beyond 14 days were also excluded from the analyses. This was to ensure comparability of intervention with antibiotics between patients.
Defining and management of PExs
A PEx was defined as ‘an event in the course of the disease in which there is an increase in symptoms beyond day-to-day fluctuations for the patient who required treatment with IV antibiotics’. This was adapted from that of acute exacerbation of chronic obstructive pulmonary disease (COPD) as previously defined. 10 All patients received a combination of two antibiotics: aminoglycoside usually tobramycin or amikacin and another antibiotic of the following: ceftazidime, aztreonam, piperacillin-tazobactam or meropenem.
Upon the decision to start treatment with IV antibiotics, patients underwent the following set of assessments: measurement of respiratory symptom score, spirometry and body mass index (BMI) measurement. Venous blood samples were collected for the measurement of C-reactive protein (CRP) and clotted blood was centrifuged and the sera stored at −70°C for future cytokine analysis. All assessments were repeated on day 14 of treatment.
TUNE was calculated as the number of days from day 14 of that PEx until the day of start of the next course of IV antibiotics. For the purpose of this analysis, if no PExs occurred during the follow-up period, TUNE was considered as 365 days.
Risk factors selected for analyses
Risk factors for shorter TUNE that were selected for assessment were based on the results of a previous study that examined factors associated with increased frequency of PExs. 8 These were age, gender, chronic infection with PA, CFRD and site of treatment (home or hospital). In addition, we included allergic bronchopulmonary aspergillosis (ABPA) based on our observations that this factor contributed to shorter time between PExs.
In order to account for the contribution of resolution of symptoms of PEx at the end of exacerbation treatment, a number of day-14 parameters were selected for analysis. These were FEV1, CF symptom score, BMI, CRP, serum interleukins (IL-6 and IL-8) and serum tumour necrosis factor-alpha (TNF-α). The choice of these cytokines was based on two publications by Kube et al. who reported increases in secreted IL, IL-8 and TNF-α in cell lines in response to PA. 11,12
Chronic infection of PA was defined as growth of these bacteria in the sputum in at least 50% of sputa collected within the previous 12 months. 13
ABPA was considered to be present if the patients fulfilled the following criteria: symptoms of asthma (wheeze and chest tightness), rise in immunoglobulin E (IgE) of at least double the upper limit of reference value (87 IU/100 ml in our laboratory) and raised specific IgE for aspergillus. 14
Diabetes in CF patients was regarded to be present if the patients met one or more of the criteria identified by the UK CF Trust guidelines. 15 These were (a) random plasma glucose level of more than 11.1 mmol/L on 2 occasions during disease stability away from pulmonary exacerbations; (b) impaired glucose tolerance test (120 min postglucose plasma levels of 7.9–11 mmol/L) with weight loss and deteriorating clinical condition; (c) patient with hyperglycaemia on regular daily glucose monitoring and weight loss or clinical deterioration or plasma glucose at 120 min of more than 11.1 mmol/L. All our patients with CFRD were on insulin and were managed in a multidisciplinary CF diabetes clinic.
Site of treatment (hospital or home) was decided upon as a consensus between patients and the CF team. Patients were considered to have been treated at home if they received over 80% of the treatment at home. If patients were treated in hospital or at both hospital and home the site of treatment was classified under other. As part of the research programme, all patients treated at home received two structured visits every week from CF nurses or CF physiotherapists throughout the course. At each visit, emphasis was made on regular physiotherapy, adherence to treatment and advice on physical rest and proper nutrition.
All spirometry measurements that were performed during the course of exacerbations were part of routine clinical assessment that all patients underwent. Spirometry was performed by qualified and experienced lung physiologists using daily calibrated lung function equipments according to the recommendations of the British Thoracic Society/Association of Respiratory Technicians and Physiologists guidelines. 16 The operators were unaware of the study.
The symptom score used in this study has been described and validated. The article is currently in press. 17 The score evaluated four symptoms: cough, sputum, breathlessness and fatigue. Each symptom was scored from 0 (no symptoms) to 4 (severe symptoms). The total symptom score was the summation of the individual scores of the four symptoms. The score was found to be sensitive to change and correlated with lung function tests. Symptom score was assessed at the start and at the end of the IV course of antibiotics.
Blood samples were taken at the start (day 1) and at day 14 of antibiotic treatment. These were sent for identification of CRP at the Biochemistry Laboratory at the Bristol Royal Infirmary. In our institution, CRP values of over 5 mg/100 ml were regarded to be raised and values exceeding 19 mg/100 ml were clinically significant.
Clotted blood samples were centrifuged and the sera were stored in a freezer at −70°C for cytokine analyses. Plasma levels of IL-6, IL-8 and TNF-α were determined using the microsphere-based multiplexing technique (Luminex 100 system, Luminex Corp., Austin, Texas, USA). Assays were performed according to the manufacturer’s protocol.
Statistical analysis
Statistical analyses for this research were done with the help of Biostatistics Units at University Hospitals Bristol NHS Trust. Two computer statistic packages were used: GP Stat and Prism 4.
Each exacerbation was regarded to be a separate entity. Analyses were done in steps. First, all data were examined for normality of distribution. Second, analyses of each factor that may have contributed to TUNE were made separately. Standard methods of comparisons and correlations were applied. It was clear that TUNE was not normally distributed (Figure 1) and therefore, nonparametric methods were used. For example, comparison of TUNE in patients with and without ABPA was made using Mann-Whitney U test. Similar method was used to compare TUNE in patients with and without PA or CFRD. Comparison of age in those with and without CF-related complications was made using two-tailed Student’s t test.

Histogram of time until the next exacerbation (TUNE) in pulmonary exacerbations (PExs) included in this study.
Correlation coefficients between TUNE, age, FEV1, CRP and log10 cytokine levels were identified using Spearman’s correlation test.
The third step was to apply forward stepwise multiple regression analysis for candidate variables. For this analysis, TUNE was the dependent variable.
Results
A total of 170 exacerbations in 58 adult CF patients were assessed. Accurate data on TUNE was available in 161 (94.7%) of all PExs. Table 1 shows patients’ demographic data for all patients and for patients as divided for those with long TUNE (over the median of 112 days) and short TUNE (below the median of 112 days). Figure 1 shows the distribution of TUNE in the exacerbations included in the analyses. TUNE was 1–6 months for the majority of patients. In 9.4% of all PExs, no subsequent PExs was encountered after 1 year of follow-up.
Patients’ demographic data in all patients, patients with long TUNE (TUNE above median days) and short TUNE (TUNE below the median days) a

Best: represent the greatest value of each measurement in the year of the study; FEV1: forced expiratory volume in the first second; % predicted: percentage of predicted of value for age, gender and height with Knutson’s correction; BMI: body mass index; ABPA: allergic bronchopulmonary aspergillosis; CFRD: CF-related diabetes; Pseudomonas aeruginosa: patients chronically infected with this bacteria (see text); site of treatment: ‘Other’ refers to treatment given in hospital or in mixed site (see text); TUNE: time until the next exacerbation.
aDifferences between all factors did not reach statistical significance.
Patients with CFRD, ABPA or PA were on the whole older than patients without either of these complications (Table 2).
Age in patients with and without CF-related adverse risk factors a
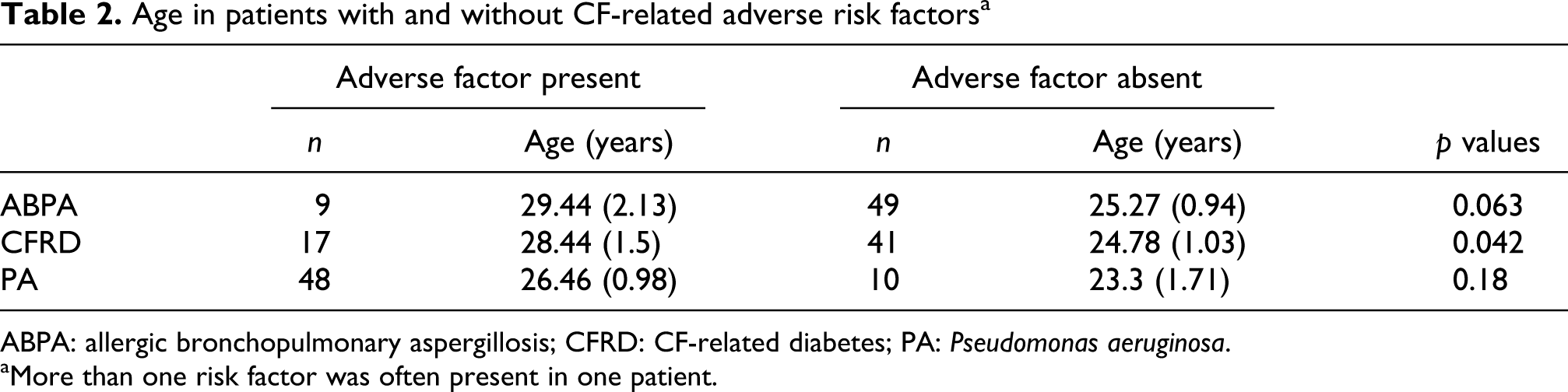
ABPA: allergic bronchopulmonary aspergillosis; CFRD: CF-related diabetes; PA: Pseudomonas aeruginosa.
aMore than one risk factor was often present in one patient.
Out of 135 measurements of day 14, CRP values of over 5 mg/100 ml (raised) and over 19 mg/100 ml (clinically significant) were measured in 56 (41.5%) and 34 (25.2 %) patients, respectively.
When using univariate analyses, patients with ABPA and CFRD had shorter TUNE compared to patients without (Table 3).
TUNE (days) in patients with and without CF-related adverse risk factors

CFRD: CF-related diabetes; PA: Pseudomonas aeruginosa; TUNE: time until the next exacerbation.
TUNE did not differ according to site of treatment; mean days (SD) 118.2 (103.6) for those who were treated at home for PExs compared to 122.1 (100.7) for those who were treated in hospital or had treatment in mixed site (others).
Assessment of symptom score, FEV1 and BMI at day 14 of treatment was made at a proportion of patients mainly due to lack of adherence to attending that visit or in some patients due to unwillingness to complete the symptom score. Similarly, blood samples were provided for CRP, IL-6, IL-8 and TNF-α in a proportion of patients. There was a significant correlation between TUNE and day-14 FEV1 but not BMI. A significant inverse correlation was found between TUNE and day-14 CF symptom score and CRP but not any of the other proinflammatory markers (Table 4).
Correlation coefficient values between TUNE and factors assessed at day 14 of intravenous treatment

BMI: body mass index; CF: cystic fibrosis; CRP: C-reactive protein; FEV1: forced expiratory volume in the first second; IL: interleukin; TNF-α: tumour necrosis factor-alpha; TUNE: time until the next exacerbation.
Multiple regression analysis was applied. TUNE was the dependent factor. Table 5 shows that, after applying multiple regression analysis, factors contributed to shorter TUNE were older age and lower day-14 FEV1 but not any of the other candidate factors.
Summary of multiple regression analysis a
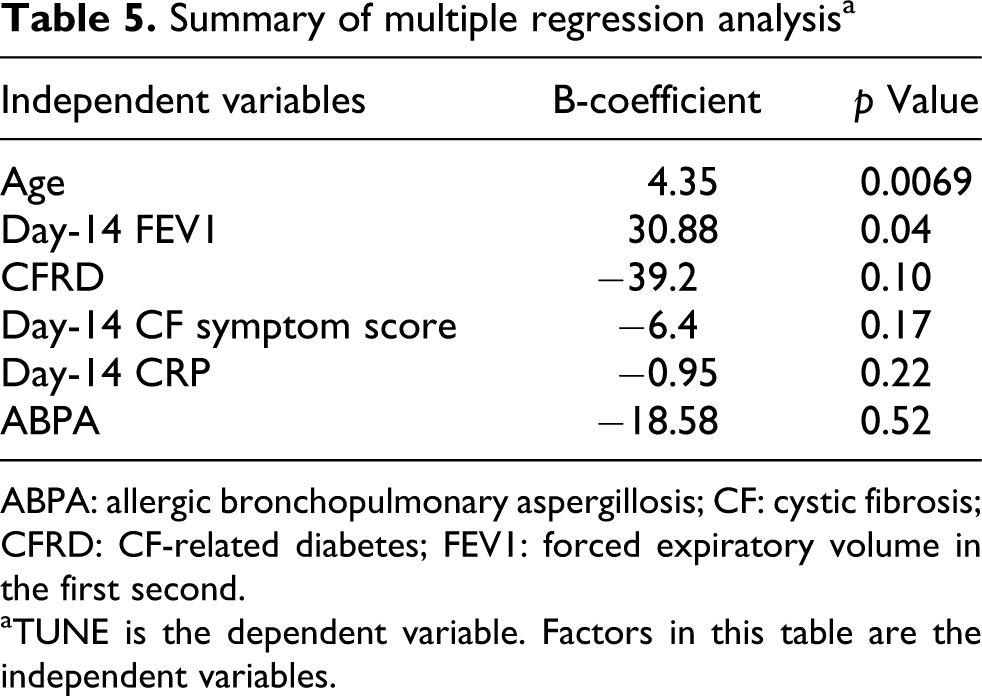
ABPA: allergic bronchopulmonary aspergillosis; CF: cystic fibrosis; CFRD: CF-related diabetes; FEV1: forced expiratory volume in the first second.
aTUNE is the dependent variable. Factors in this table are the independent variables.
Discussion
To our knowledge, this is the first study to prospectively investigate factors affecting TUNE in adult CF patients. The only parallel work was done in patients with COPD. 18,19
In the majority of cases subsequent PExs occurred within 6 months from the initial PEx, but in approximately 10% of all PExs no PEx occurred within 1 year.
During the assessment of TUNE, we did not take into account oral antibiotics given to mild PExs. Our reasons for excluding courses of oral antibiotics are that the indications are often looser than those for IV antibiotics and because we regarded exacerbations needing IV antibiotics to be a more robust defining factor for PExs. We are not clear that excluding oral antibiotics would have changed the outcome of this study, but we would understand a contrary argument.
In our study, we confined the analysis to PExs induced by PA as they constituted the majority of adult CF patients. We also ruled out PExs needing more aggressive treatment IV antibiotics for more than 14 days and PExs needing more than 2 antibiotics, as including these may play a role in TUNE.
Throughout the programme, we opted for an ‘action definition’ of PExs that was dependent on the decision to treat by clinicians upon patients’ presentations. In the planning stage, we were cognizant of other definitions, 20,21 but most of these were either orientated to paediatric and young adult CF patients or based on case scenarios rather than patient-based experience.
The key findings of this study suggest that older CF patients with poorer lung function tests are at increased risk for shorter TUNE. The implication of this analysis may merit consideration for altering patients’ management in high-risk patients and may need to be factored in clinical trials where TUNE is an outcome.
Reporting the comparisons and correlations of single risk factors with TUNE as well as multiple regression analysis yielded useful data. We found that the prevalence of CF-related complications outlined in Table 2 appeared to be greater in our study population than those reported for adult CF literature. This was because patients included in this study were those who presented with at least one PEx. CF-related complications were found to be more prevalent in older patients and TUNE was significantly shorter by average 34, 47 and 56 days in patients with PA, CFRD and ABPA, respectively (Table 3).
Given that old age (Table 2) and reduced day-14 FEV1 4 were common denominators in those with CF-related complications, multiple regression analysis found these two factors to independently influence TUNE. As other factors (ABPA, CFRD, day-14 symptom score and day-14 CRP) were likely to be affected by FEV1 and age, they were discounted per se as independent factors influencing TUNE.
Serum inflammatory markers (CRP) and proinflammatory markers (cytokines) at day 14 did not contribute to TUNE. This is in variance of the results of studies in COPD in which greater CRP and higher symptoms at the end of exacerbations were associated with a shorter time until the following exacerbation. 18
The reason for this difference may simply reflect the difference between two disease processes. The lungs in adult CF patients are probably on the whole inflamed to greater extent than those of COPD. This is manifested by more prominent systemic inflammation shown by high values of CRP at the end of PExs in CF patients. CRP values greater than 19 mg/L at the end of treatment was found in quarter of patients, which would suggest a residual lung (and systemic) disease in a significant number of patients. Also, whilst many COPD patients included in the studies referred to above would be expected to have low volume of bacterial load, the majority of CF patients included in our study were chronically infected with PA and with other CF bacteria at the time of their inclusion and would be expected to remain so at the end of IV treatment for PExs. A third reason would be in the fact that whilst our study showed correlation between CRP and TUNE (like the COPD study did), the COPD study did not use multiple regression analysis.
Based on previous studies, we elected to include only risk factors that we previously found to be associated with adverse outcome of PExs. 4,8 It could be argued that the study should include other factors such as genetic profile and pancreatic status. We also did not examine the contribution of chronic infection with other bacteria such as Staphylococcus aureus, Stenotrophomonas maltophelia and Burkholderia cepacia. At the time of this research, none of our patients grew Burkholdeia cenocepacia and only few had Burkholderia multivoran. In addition, perceived shortcomings of this study would be in not factoring control of diabetes by including blood level of glycosylated haemoglobin (HbA1c %).
Similarly, it could be suggested that we should include medications in the analyses. These were not included mainly because our practice in managing adult CF patients was policy based. For that, most of our patients would have been on azithromycin and all patients with CFRD are on insulin. Most patients with ABPA were on low dose of prednisolone and/or inhaled corticosteroids together with long-acting bronchodilators.
Whilst this argument is valid, the disadvantage of including all these factors in the analysis is that we would dilute risk factors reported previously and we would be doing too many analyses which may weaken the study.
This study had its limitations, some of these were already outlined in the discussion. The number of patients was relatively modest. Given the limited number of CF patients available in most adult CF units, our study, like other studies, 22,23 treated exacerbations as a separate entity. Cluster analyses would have been appropriate but of the relatively small number of patients. Larger studies may need to focus on the appropriateness of whether or not several PExs in one patient could feasibly be included in separate analyses. This is important in interventions used in a rare disease such as CF.
The findings of this study suggest that older CF patients with poorer lung function tests are at increased risk for shorter TUNE. The implication of this analysis may merit consideration for altering patients’ management in high-risk patients and for clinical trials. Adjustment for age and FEV1 in clinical trials of interventions in which TUNE is an end point of analysis may need to be made. For high-risk patients suggested alteration to management may need to be made. This may be done by close follow-up of patients following PExs, choosing a combination of more than two antibiotics or by adding adjuvant doses of oral corticosteroids when treating PExs. The latter is not unusual as many CF physicians in the UK reported using oral corticosteroids as an adjuvant to antibiotics during CF exacerbations 24 and a small prospective study suggested beneficial outcome from adding oral corticosteroids. 25
It would be understandable that CF clinicians might raise objections to these methods as a mean to extending TUNE. We would conclude that no evidence exist to the efficacy of each suggested method. Further we would advocate that all interventions would need to be weighed against its potential harm and would merit examination of their effectiveness.
Footnotes
This research was funded by an unrestricted grant from David Tellings Charitable Trustees – Bristol.