
Abstract
Background
Frailty is common among patients referred to pulmonary rehabilitation (PR) programs. While it is considered an independent predictor of program non-completion, people with frailty respond positively to PR. Clinicians’ perspectives on assessing and managing frailty in PR has not been established. This study aimed to identify clinicians’ current practices, perceptions, and opinions on assessing and managing frailty in people who attend PR in Australia and New Zealand.
Methods
An international online survey targeting healthcare professionals in Australia and New Zealand involved in PR programs using a combination of multiple-response closed-ended and open-ended questions. This survey study was reported in accordance with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS).
Results
Of 103 responses, 89 healthcare professionals completed the survey (92.6% completion rate). Nineteen percent routinely assessed frailty, mostly using Short Physical Performance Battery (SPPB). Respondents reported the main considerations for choice of frailty assessment tools were ease of use and cost. The most common frailty indicators identified by respondents included falls history, low body weight, slow or aided gait, and muscle weakness. Seventy-nine percent believed PR to be appropriate to manage frailty in this population, while 94% desired additional resources in future guidelines. Suggestions to improve PR to better manage frailty included reshaping rehabilitation program content, and providing specific patient education. Future desired research priorities included improvements to frailty assessment tools, frailty-specific guidelines and workforce training.
Conclusion
This study explores PR practices among clinicians in Australia and New Zealand, showing variability in frailty assessment and management. It provides a foundation for evaluating key aspects of PR models that can be tailored to these clients’ needs and limitations.
Introduction
Pulmonary rehabilitation (PR) is an essential non-pharmacological treatment for a range of chronic lung diseases. It is a multi-component and multidisciplinary therapeutic intervention that reduces symptoms, enhances function, and improves the quality of life of people with chronic lung diseases.1,2 As such, PR is recommended in international clinical practice guidelines, 3 including in Australia and New Zealand. 1
Frailty is a syndrome characterised by diminished reserves and heightened susceptibility to stressors.4,5 One of the most common models for conceptualising frailty describes it through five main clinical characteristics: unintentional weight loss, fatigue, muscle weakness, decreased gait speed, and reduced physical activity. 5 The presence of frailty has been shown to be associated with adverse health outcomes for older adults, such as falls, acute care hospitalisations, disability and death.4,5 The global prevalence of frailty among patients with chronic lung disease ranges from 20% to 58%.6–9 Data from Australia and New Zealand are limited. However, one previous study attempted to measure how frailty affects long-term survival after intensive care unit (ICU) admission for Chronic Obstructive Pulmonary Disease (COPD) exacerbation, finding a frailty prevalence of 54%. 10 Frailty has gained increased recognition as a “treatable trait” 11 of importance in the management of people with chronic lung diseases.12,13 This has led to understandable inquiry regarding the suitability of PR programs to address the limitations and needs of people with chronic lung disease and coexisting frailty.
An emerging body of research examining the prevalence of frailty specifically within the PR context suggests it is potentially detectable in 25–58% of patients.12,13 Although limited data exists from robust clinical trials regarding the impact of PR on people with chronic lung disease and coexisting frailty, various cohort studies have shown frailty instruments demonstrate responsiveness to PR14–19 suggesting probable benefits. Despite this, gaps in knowledge remain regarding the role of PR in managing frailty as well as an understanding of current practices that clinicians use for assessing and managing frailty within PR. This is important to understand as the healthcare professionals responsible for delivering PR (e.g. physiotherapists, exercise physiologists, nurses, occupational therapists, dietitians and medical clinicians),1–3 may differ in their understanding and/or perspectives on how to ideally manage coexisting frailty in this context. Understanding the needs and perspectives of these healthcare professionals and the potential barriers and facilitators impacting upon service delivery are critical first steps towards improve clinical care for this important patient group.
Objective
This study examined clinicians’ practices and views on assessing and managing frailty during PR in Australia and New Zealand.
Methods
Study design and survey development
This study was a cross-sectional electronic survey conducted between June to September 2021. Ethics approval was obtained from the Monash University Human Research Ethics Committee (reference 27053). Consent for anonymous participation was obtained within the survey following review of the explanatory statement. The survey involved 32 questions covering four areas: (1) demographic details of participants and PR programs; (2) the significance of assessing and managing frailty in these programs; (3) clinicians’ confidence in assessing and managing frailty during PR; and (4) specialised training in frailty management undertaken. Questions about the future of frailty assessment and management in PR were also included. To ensure the study’s brevity, most questions were designed using 5-point Likert scales (e.g., ‘much less effective,’ ‘somewhat less effective,’ ‘neutral/about the same,’ ‘somewhat more effective,’ and ‘much more effective’), multiple-response questions, or yes/no/unsure options. Open-ended questions were also included to allow for more in-depth responses. The survey was pilot-tested with five clinically-based allied health professionals to evaluate face validity. This resulted in minor wording adjustments for clarity and suggestions to reduce total survey length, which were accommodated. A blank copy of the final instrument is included in the Supplemental S-1. The survey was constructed in a university-hosted secure Qualtrics account, accessible only to the project team. Default settings were applied without imposing additional restrictions on IP addresses (e.g. to prevent survey re-entry or unintended multiple completions by individuals). Reporting of findings followed the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) checklist. 20 Supplemental S-2: Completed CROSS Checklist.
Settings and participants
Healthcare professionals working in PR who were involved in the coordination or delivery of PR in the last 24 months were eligible to participate. The research team contacted participants via email, social media outlets and advertisements in peak respiratory bodies across Australia and New Zealand (retained on message boards throughout the study period). Participants were encouraged to circulate the survey link among interested colleagues (i.e., snowball sampling). The survey was expected to take fifteen to 20 min. No formal power calculation was conducted to determine a target sample size due to the exploratory and broad nature of the survey and the lack of suitable data upon which to formulate such decisions. Due to the snowballing nature of recruitment, no follow-up action was able to be conducted at the individual participant level, and response rates were not able to be calculated.
Data analysis
Survey data were analysed using Stata 14 SE. Categorical data were expressed in terms of frequencies and percentages, illustrated in appropriate graphs or tables. Responses from five-point Likert scales were dichotomised into two categories: (‘much more effective/somewhat more effective’ and ‘about the same/somewhat less effective/much less effective’) permitting comparisons via Chi-square test. No attempts were made to manage or impute missing data apart from conducting a complete analysis of available data per item (e.g. relative to the denominator per question). No sensitivity analyses were conducted or attempts made to adjust variable data or account for any confounders.
Open-ended responses were synthesised using a simplified process of content analysis. 21 Briefly, this involved familiarisation of the dataset through repeated readings, coding of recurring ideas and concepts, collation of data under preliminary themes, and refinement to determine final theme descriptors. Themes were initially identified and developed by author AA, then independently reviewed and discussed with authors CO and KH to ensure consensus and reliability. Cases lacking responses to these questions were omitted from the analysis.
Results
Demographic data
Demographic characteristics of participants from PR settings.

Abbreviations: PR: pulmonary rehabilitation; MPhil: master of philosophy; PhD: doctor of philosophy; N: total sample size; n: subgroup sample size; IQR: interquartile range.
Demographic data (PR programs).

Abbreviations: PR: pulmonary rehabilitation; N: total sample size; n: subgroup sample size; IQR: interquartile range.
aPercentages may exceed 100% because respondents were able to select multiple. Outpatient programs involve scheduled, clinical treatment at facilities like—hospitals or clinics, focusing on medical or therapeutic care. Community-based programs offer flexible, non-clinical support in local settings—like community centres, schools, churches, or even patients’ homes, emphasising social integration and peer-led assistance.
Current practice
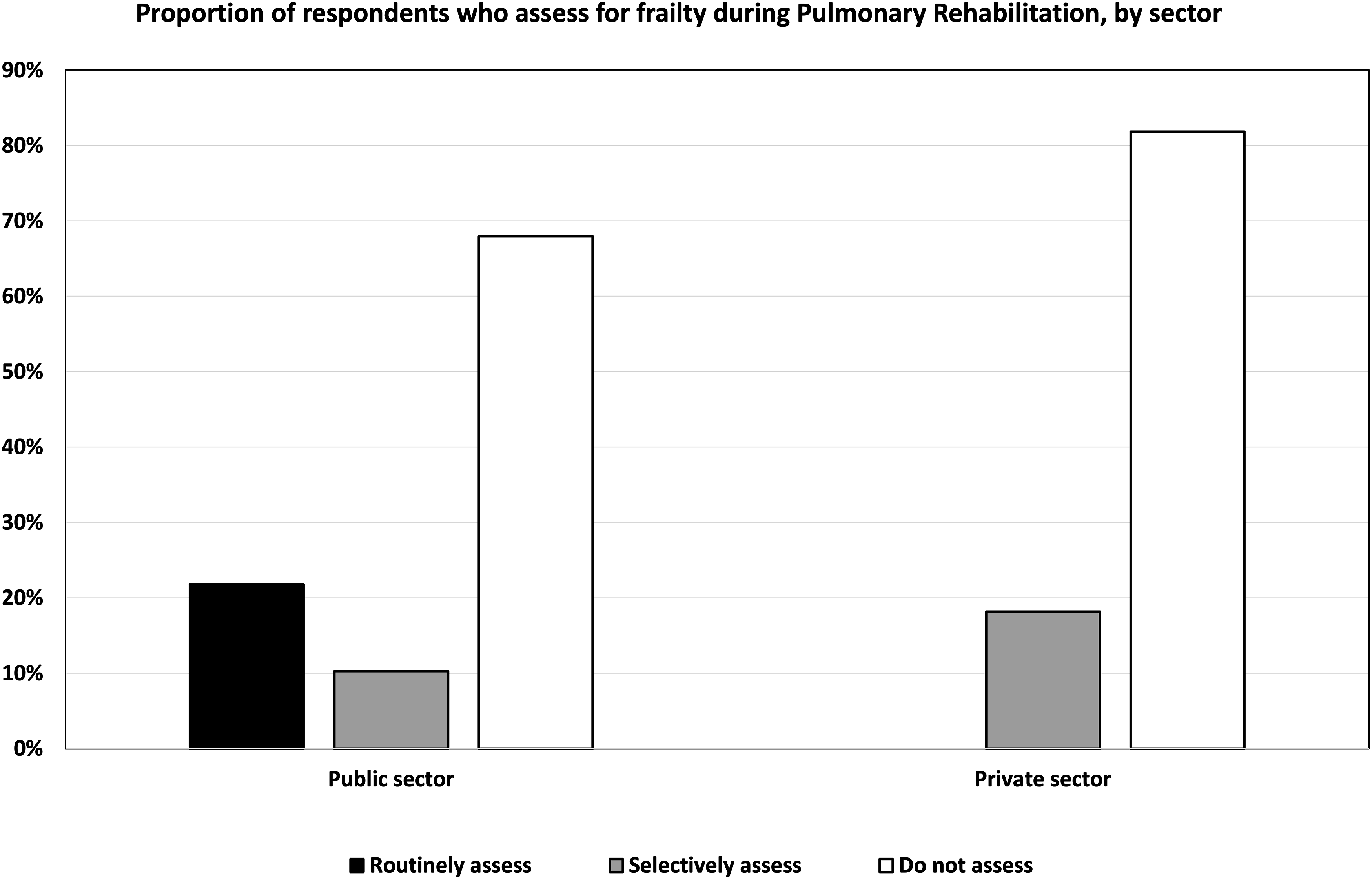
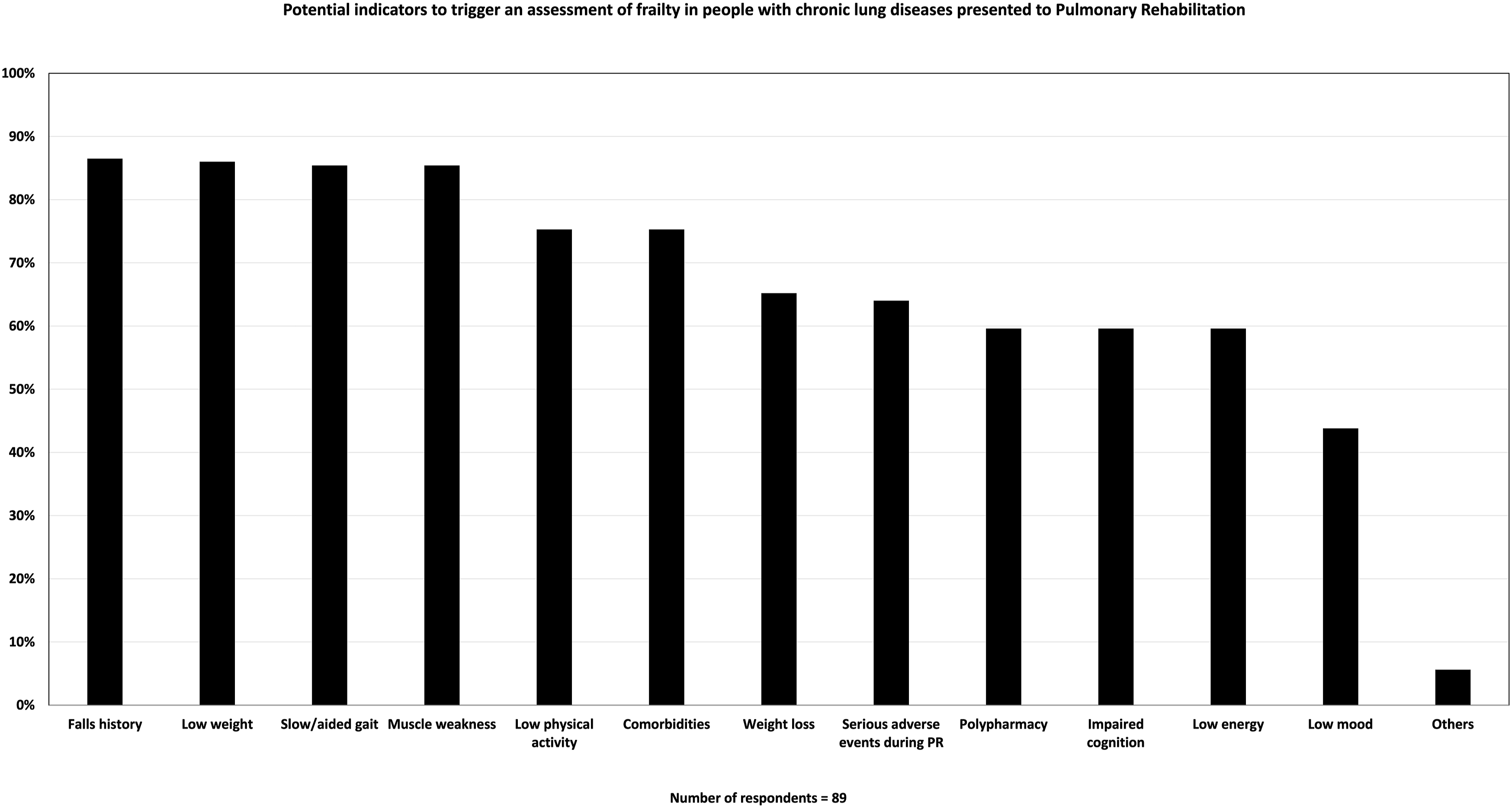
Nineteen percent (17/89) of respondents reported they routinely assessed frailty during PR (Figure 1). Interestingly, there appeared a difference in the use of routine frailty assessment between public and private sector sites with it only occurring in public health services, however this were not statistically significant (p = 0.202; Figure 2). The use of specific instruments to assess frailty was varied and low in general. The most commonly used instruments were: Short Physical Performance Battery (SPPB): 6% (5/89); Clinical Frailty Scale (CFS): 4% (4/89); FRAIL: 3% (3/89); Fried Frailty Phenotype (FFP): 2% (2/89); and Frailty Index (FI): 2% (2/89). The reasons respondents selected a specific assessment tool over others also varied, with the most reported factor being the ease of using the instrument (ease of administering the tool, ease for clinicians to understand/administer, and/or ease for patients to understand/perform), as indicated by 38% (34/89) of respondents. As 14.6% (13/89) of respondents indicated, low cost also influenced their tool selection. Other reasons included centre protocols, no training required, equipment availability, widespread usage, no-cost licensing, and evidence-based support, which together accounted for 40% of responses—(34/89) selected one or more of these options. However, only 4.5% (4/89) of respondents attributed sensitivity to detecting change during PR as the reason for their selected instrument (see Supplemental S-3). The most common indicators for assessing frailty reported by participants were evidence of a fall history 86.5% (77/89), low weight 86.5% (77/89), slow or aided gait 85.4% (76/89), and muscle weakness 85.4% (76/89) (Figure 3). Frequency with which respondents routinely assess, selectively assess, or don’t assess for frailty during Pulmonary Rehabilitation. Proportion of respondents who assess for frailty during Pulmonary Rehabilitation, by sector. Potential indicators to trigger an assessment of frailty in people with chronic lung diseases presented to Pulmonary Rehabilitation.
Perceptions regarding PR to manage frailty
Respondents’ perceptions regarding frailty assessment and management in PR settings.

Abbreviations: PR: pulmonary rehabilitation; N: total sample size; n: subgroup sample size; IQR: interquartile range.

Perceived effectiveness of Pulmonary Rehabilitation in managing frailty.
Barriers to assessment and treatment of frailty during PR.

Abbreviations: PR: pulmonary rehabilitation.
aPercentages may exceed 100% because respondents were able to select multiple.
Aspects of PR requiring adapting
Clinicians identified multiple aspects of PR programs they felt required adaptation to address frailty in people with chronic lung disease. These are described in detail in the Supplemental S-4 and Figure 5. Example topics included: exercise prescription (e.g., tailored intensity and balance components), education (e.g., cognitive adaptations and frailty-specific content), safety (e.g., fall risk management), staffing (e.g., improved ratios and multidisciplinary input) and program structure (e.g., flexible duration, support for community transport). Qualitative themes from clinician responses to “Aspects of Pulmonary Rehabilitation requiring adaptation due to Frailty in people with Chronic Lung Diseases”.
Priorities areas for future work related to frailty in PR
Several multifaceted aspects of PR were perceived to require future research to enhance the management of frailty. These included improvements to assessment methods (e.g., standardisation of tools), guideline development (e.g., protocols for exercise prescription and progression), program structure (e.g., flexible models, multidisciplinary team input, staff ratios), and future education (e.g., of patients and the health workforce). Further information regarding these perspectives is available in Figure 6 and Supplemental S-5. Qualitative themes from clinician responses to “Priority area for future investment/research on Frailty in people with Chronic Lung Diseases undertaking Pulmonary Rehabilitation”.
Discussion
Pulmonary rehabilitation (PR) is an essential component in the management of a range of chronic lung diseases; however, its precise role in addressing the complex needs of individuals affected by coexisting frailty has yet to be fully defined. Frailty is an important “treatable trait” 11 and PR appears to address some of the potentially contributing factors underpinning its development. However, the limited evidence in this field 17 means gaps in knowledge and clinical guidance exist, which can lead to clinical uncertainty and service variability. This underpins the importance of the present study to seek perspectives from clinicians at the forefront of this important area of practice. While contextualised to Australia and New Zealand respondents, the findings are likely transferable to many other settings with similar health systems and PR program structures.
It was interesting to note that most respondents felt they lacked adequate training in the assessment and management of frailty in people with chronic lung diseases, while 70% (62/89) of clinicians reported not assessing frailty during PR, despite its high reported prevalence.6,17,22–26 Further, frailty assessment were only routinely conducted in public and not private health settings. While the reasons for this are not clear, it is plausible frailty awareness could be greater in settings attached to hospital-based healthcare settings (e.g. outpatient departments) due to educational opportunities that might traverse such boundaries. Of the instruments used to evaluate frailty, the SPPB was the most frequently reported tool. The SPPB demonstrates good responsiveness to PR interventions in multiple studies,14–19 and its preference for use might reflect this rationale. Alternatively, it may also be perceived a simple tool to implement or may be a familiar tool to clinicians and/or one that pertains relevance to aspects of treatment decision-making. It is multi-component in nature, but focuses on physical performance and thus the concept of ‘physical frailty’. If considering frailty through a broader lens, one might argue use of the SPPB neglects the necessary dimensionality to gain accurate insights into patients’ individual contributing factors to their condition (e.g. cognition, environmental and/or psychosocial domains). This poses a challenging clinical dilemma as broader instruments possessing a more comprehensive focus to one’s frailty may impose time cost burdens for implementation and lack sensitivity to change following an intervention such as PR. Examples of such tools, such as the Edmonton Frailty Scale, 27 Groningen Frailty Indicator (GFI) 28 or Tilburg Frailty Indicator (TFI), 29 were rarely used by survey participants. No specific instrument has yet been advocated for use as a ‘gold standard’ in PR. There may, however, be benefit in exploring the roles of different instruments to determine the potential to better tailor personalised treatments during PR based on the underlying frailty components that might exist within individuals.
Almost 75% (66/89) of survey participants perceived PR as not being extremely or very effective for managing frailty in this population (Figure 4). This appears at odds with previous studies that suggest individuals with very poor exercise tolerance actually have the greatest potential and magnitude for improvement from PR.17,30 Several factors could explain this observation. One may relate to the increasing multi-systemic clinical complexity inherent in frailty, which can contribute, almost by definition, to various physical, social, and psychological challenges to engage with and derive benefit from. 31 Another factor can be the downstream impacts of frailty on access to services, transport, and facilities, which can hinder progress. This may also relate to findings indicating frailty as an independent predictor of program non-completion. 17 An alternative explanation for this perception could be a lack of experience or knowledge by clinicians about how to manage frailty in a PR setting, indicated by respondents’ reported difficulty in adapting PR to frailty 69% (48/70), insufficient training 73% (52/71), a strong desire for new resources 94% (68/72), and perceived barriers such as low awareness, lack of confidence, and absence of guidelines (Table 3). This suggests a possible need to develop and disseminate resources and training for clinicians to improve their knowledge, skills and confidence in managing frailty optimally in people undergoing PR. These could take the form of informal ‘professional development’ resources through professional societies or more formalised training courses/credentials through specialist centres or education providers. Ultimately, it will be important that future practice guidelines incorporate necessary adaptations to account for the unique issues imposed by frailty and that quality improvement measures or standards are considered to ensure effective implementation.
It is interesting to speculate how these insights might impact future clinical practice. Important perspectives that are presently lacking include the patient and caregiver perspectives on frailty during PR. This is an important gap worthy of further research. Another interesting issue is the ‘fit’ of PR for the management of frailty in people with chronic lung disease. On the one hand, frailty is now well recognised as a treatable trait of importance, and PR is arguably one of the leading interventions to help address it due to its multidisciplinary focus and ability to target the physical components of frailty. However, this does not mean PR effectively manages all aspects of frailty nor that all individuals who participate in PR gain the optimal benefits from PR. Survey respondents in the present study suggested adaptations may be indicated to better account for the issues unique to frailty, and it is plausible that conventional approaches to exercise training might not ideally suit the limitations specific to this patient sub-group. Further, the high dropout rate previously highlighted in people with COPD and frailty 17 suggests the PR model itself might require careful consideration to ensure optimal engagement and completion. This has been highlighted previously.12,13,32
Limitations
The present study is not without some limitations. Our use of snowballing sampling of clinicians meant determining an accurate response rate relative to the total potential sample pool is not possible. Our distribution to PR coordinators and clinicians in the field may also have skewed responses mostly to physiotherapists (who most commonly coordinate these services in Australia and New Zealand) despite the goal to sample multidisciplinary staff more broadly. While we were unable to determine an accurate response rate for this survey, we note the 89 responses compare favourably to prior national efforts33,34 which similarly yielded informative perspectives on the health workforce landscape. Despite these limitations, the study offers valuable insights into clinicians’ perspectives on frailty assessment and management during PR that have not previously been explored. Additionally, while consumer input from patients with frailty would have been desired, this was deemed beyond the scope of the present study remit.
Conclusion
Clinical practice for the assessment and management of frailty during PR in Australia and New Zealand is varied and requires greater focus and support in order to embed systematic improvements aimed at improving clinical outcomes for this important patient group. Several key areas for future improvement were highlighted that could serve as a useful foundation for future research.
Supplemental Material
Suppplemental Material - Assessment and management of frailty during pulmonary rehabilitation: An international survey of Australian and New Zealand clinicians
Suppplemental Material for Assessment and management of frailty during pulmonary rehabilitation: An international survey of Australian and New Zealand clinicians by AL Alzubaidi, S Soh, M Wuyts, P Munro, KD Hill, CR Osadnik in Chronic Respiratory Disease
Footnotes
Author Contribution
Anita Stieglbauer, Melbourne, Australia
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.