
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is associated with alterations in brain function that contribute to reduced respiratory and skeletal muscle strength, ultimately limiting exercise capacity. Transcranial direct current stimulation (tDCS), a non-invasive neuromodulation technique, has demonstrated efficacy in enhancing lower extremity function in healthy older adults.
Objective
To evaluate the effects of a single session of anodal tDCS on exercise capacity, respiratory muscle strength, and physical performance in individuals with COPD.
Methods
In a randomized, double-blind, sham-controlled trial, 26 participants with COPD underwent baseline assessments of exercise capacity (Six-Minute Walk Distance, 6MWD), respiratory muscle strength (Maximum Inspiratory Pressure, MIP), and physical performance (4-m Gait Speed, 4MGS). Participants then received either active or sham tDCS, followed by reassessment 1 day post-intervention.
Results
Compared to sham, the active tDCS group showed significant improvements in physical performance, including increases of 46 ± 11.45 m in 6MWD (p < 0.001), 12.54 ± 4.52 cm, H2O in MIP (p < 0.01), and 0.24 ± 0.08 m/s in 4MGS (p < 0.05).
Conclusion
A single session of anodal tDCS may enhance exercise capacity, inspiratory muscle strength, and gait speed in patients with COPD, suggesting its potential as a supportive intervention in pulmonary rehabilitation.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent inflammation and oxidative stress, which contribute to muscle atrophy, reduced muscle strength, and diminished endurance. These effects are exacerbated by hyperinflation-induced inspiratory loading, ultimately leading to exercise intolerance.1,2 In addition to peripheral manifestations, COPD is frequently associated with hypoxia, which impairs cerebral oxygen delivery, causes neuronal damage, and may induce structural brain changes that reduce corticospinal excitability to skeletal muscles.3,4
Previous studies have shown that increased corticospinal inhibition and decreased excitability from the primary motor cortex to peripheral muscles contribute to reduced voluntary muscle activation and the development of clinical muscle dysfunction in individuals with COPD.4,5 Therefore, interventions that reduce corticospinal inhibition may enhance neural transmission from the motor cortex to spinal motor neurons, thereby improving muscle activation and overall physical function in this population.5,6
Transcranial direct current stimulation (tDCS), a non-invasive brain stimulation technique, has shown promise in modulating motor cortex excitability and enhancing physical performance. 7 Specifically, anodal tDCS has been demonstrated to increase corticospinal excitability by elevating the resting membrane potential, thereby facilitating neuronal depolarization.6,8 While the benefits of tDCS have been explored in various populations, including healthy individuals and those undergoing physical training, its effects on exercise capacity and respiratory muscle strength in patients with COPD remain unclear.
The primary objective of this study was to assess whether anodal tDCS improves exercise capacity, respiratory muscle strength, and overall physical performance in patients with COPD. The primary endpoint was the change in 6MWD; secondary endpoints included MIP and 4MGS. This study addresses a key gap in current management by evaluating the role of tDCS as a non-pharmacologic adjunct to pulmonary rehabilitation. Findings may inform the development of novel strategies to enhance functional outcomes in this population.
Methods
Study design
A pilot randomized control trial with 26 COPD patients randomized to sham and active tDCS was conducted over 7 days. The study included baseline assessment, single treatment session, and post-treatment assessments. Participants continued their usual activities without intervention, and adverse events were monitored 7 days post-treatment.
Participant recruitment and informed consent
The sample size was calculated based on a formula for randomized controlled trials designed to detect differences between two groups, using effect size estimates from a previous study. 9 That study reported a mean difference of 22.5 m in six-minute walk distance (6MWD) between anodal tDCS and sham groups in patients with multiple sclerosis, with standard deviations of 17 m and 14.5 m, respectively. A power of 80%, a type I error rate of 0.05, and an anticipated dropout rate of 20% were incorporated into the calculation. Therefore, the sample size for each group was determined to be 13 participants.
Inclusion and Exclusion criterion.
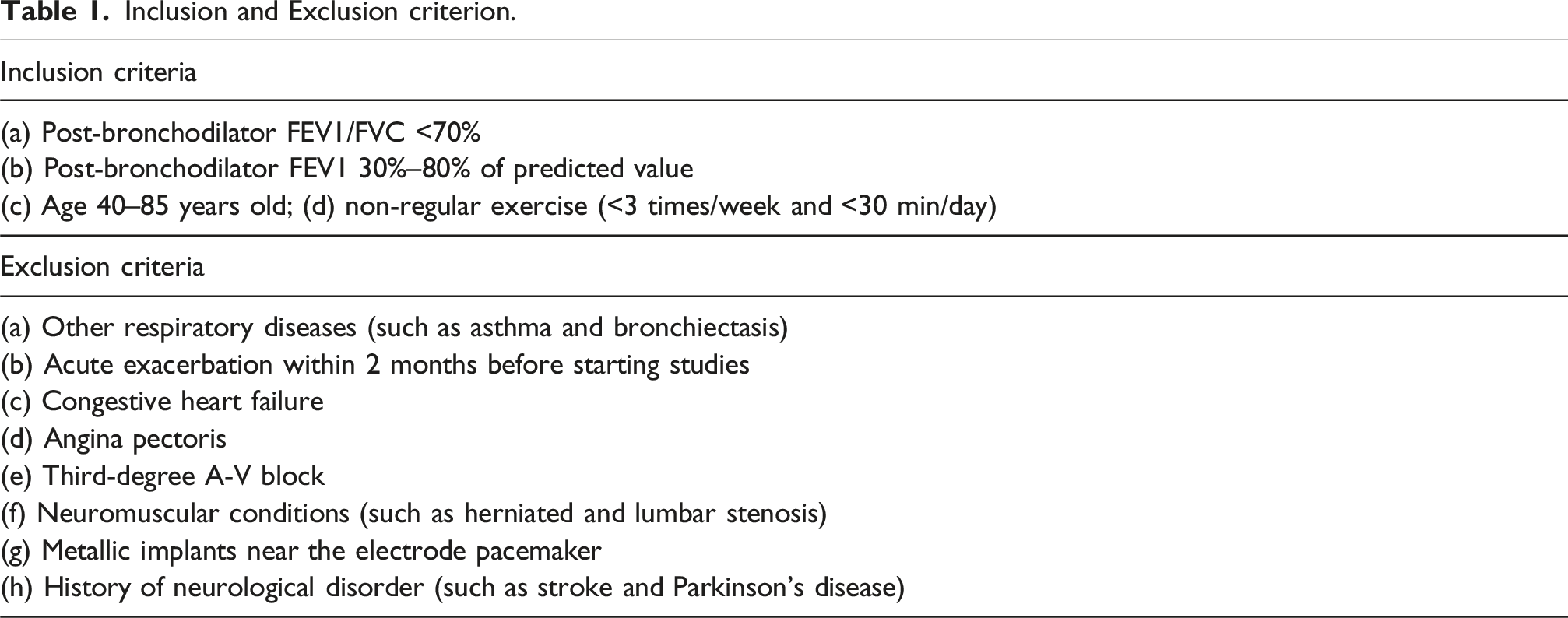
All participants underwent a history and physical examination by a chest medicine specialist. The study was conducted in accordance with the Declaration of Helsinki, approved by the Ethics Committee of Khon Kaen University (Approval No. HE651421), and registered with the Thai Clinical Trials Registry (ID: TCTR20241111001).
Randomization and blinding
Participants were stratified and randomized into two groups (Group A and Group B) based on baseline forced expiratory volume in one second to forced vital capacity ratio (FEV1/FVC), percent predicted FEV1, and 6MWD to ensure balanced distribution of key clinical characteristics. A biostatistician generated a computerized allocation schedule using stratified randomization to minimize intergroup variability. Randomization was performed in a 1:1 ratio.
To maintain methodological rigor, outcome assessors were blinded to participants’ clinical profiles and group assignments. Personnel responsible for sequence generation, participant enrollment, and intervention allocation were independent from those conducting outcome assessments. Each participant was assigned a unique identifier, and their 6MWD data—the primary outcome—were submitted to the statistician for group allocation using the pre-specified algorithm. Participants were instructed to continue their usual pharmacologic treatments throughout the study. Blinding of outcome assessors was maintained to minimize detection bias.
Transcranial direct current stimulation procedure
tDCS was administered using saline-soaked sponge electrodes (5 × 7 cm) connected to a battery-powered device (PortableTDCS, Khon Kaen, Thailand) with a maximum output of 2 mA. Anodal stimulation targeted the left primary motor cortex (M1), following the international 10–20 EEG system, while the cathode was placed over the right shoulder.
The stimulation protocol consisted of a single 20-min session, including 30-s ramp-up and ramp-down periods surrounding continuous 2-mA stimulation. In the sham condition, the current was discontinued after 30 s to mimic the initial sensation of stimulation without producing lasting neuromodulator effects.7,11
As this is the first study to apply this approach in elderly patients with COPD, the use of bilateral M1 or extracephalic montages requires caution. These configurations may unpredictably affect large-scale brain networks, including regions responsible for memory and executive function. Such off-target effects are especially concerning in older adults, who are more susceptible to neuromodulatory disturbances. 12
Outcome measurement
Exercise capacity
The primary outcome of this study was exercise capacity, assessed using the Six-Minute Walk Test (6MWT). 13 Participants were instructed to walk continuously along a 30-m indoor corridor, turning at each end, in accordance with the American Thoracic Society (ATS) guidelines. 14 A trained assessor monitored each participant throughout the test and provided standardized verbal time cues at one-minute intervals. 15 The total distance walked within the six-minute period was recorded as the 6MWD.
Pulmonary function and respiratory muscle strength
Pulmonary function was evaluated using standard spirometry, following ATS recommendations. 16 Respiratory muscle strength was assessed using a Micro Respiratory Muscle Pressure device. Maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP) were measured to quantify inspiratory and expiratory muscle strength, respectively. 17
Physical performance
Physical performance was evaluated using a battery of functional tests, including: Single Leg Stance (SLS): to assess static balance. 18 Timed Up and Go (TUG): to evaluate dynamic balance, 19 Five Times Sit-to-Stand Test (FTSST): to measure lower extremity strength, 20 and 4-m Gait Speed (4MGS): to assess gait speed. 21 Each test was administered by trained assessors following standardized protocols to ensure consistency and reliability.
Statistical analysis
All statistical analyses were performed using SPSS version 29.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of distribution for continuous variables. Descriptive statistics are presented as mean ± standard deviation (SD). Baseline characteristics between groups were compared using independent samples t-tests.
To evaluate within-group and between-group differences before and after the intervention, repeated-measures analysis of variance (ANOVA) was conducted. Effect sizes were calculated using Cohen’s d to determine the clinical relevance of observed changes. 22 All analyses were conducted under the intention-to-treat (ITT) principle.
Results
Of the 90 individuals screened, 26 met the eligibility criteria and were randomized equally into the active tDCS (n = 13) and sham tDCS (n = 13) groups. All participants completed a single intervention session. The participant flow is presented in Figure 1. Flow of participate.
Demographic characteristics of participants.

Participants received a single session of transcranial direct current stimulation (tDCS). The Sham-tDCS group had the tDCS device turned off after 30 s of stimulation, whereas the tDCS group received an anodal tDCS for 20 min.
Comparative analysis of outcomes between sham tDCS group (n = 13) and active tDCS group (n = 13) over the same timepoints.

Data are expressed as mean ± SD and mean difference ± SE. ##indicates a statistically significant difference between the active tDCS and sham groups (P < 0.01).
1Represents a significant difference between group (p < 0.05).
Exercise capacity
Post-treatment, the active tDCS group demonstrated a significantly greater improvement in 6MWD compared to the sham group (Table 3 and Figure 2). Within-group analysis confirmed a statistically significant increase in 6MWD in the active group, whereas no meaningful change was observed in the sham group (Table 4). Effects of tDCS on exercise capacity and respiratory muscle strength. The differential outcomes within the group observed at baseline and post-treatment. Data are expressed as mean ± SD” to “Data are expressed as mean ± SE. ** denotes a statistically significant within-group difference compared with baseline (P < 0.01). 1Represents a significant difference after treatment within group (p < 0.05).

Baseline respiratory rate (RR) did not differ significantly between groups. However, following the intervention, RR was significantly lower in the active tDCS group compared to the sham group (21.50 ± 1.93 vs 24.54 ± 1.80 breaths/min; p < 0.001). The change from baseline showed a significant reduction in the active group (−1.83 ± 2.62 bpm), while the sham group exhibited a slight increase (0.90 ± 2.26 bpm; p < 0.05). Within-group analysis confirmed that the reduction in RR was significant only in the active group.
Respiratory muscle strength
The increase in MIP was significantly greater in the active tDCS group compared to the sham group (Table 3 and Figure 2). Within-group analysis revealed a significant improvement in MIP following the intervention in the active group, with no significant change observed in the sham group (Table 4). No significant differences were found between or within groups for MEP.
Physical performance
Improvements in physical performance, assessed via the SLS, FTSST, and 4MGS, were significantly greater in the active tDCS group compared to the sham group (Table 3). Within-group analysis showed a significant enhancement in gait speed (4MGS) in the active group, while no significant changes were observed in the sham group (Table 4).
Adverse events
All participants completed the study without experiencing serious adverse events. Mild itching at the electrode site was reported by five participants in the active tDCS group; symptoms were transient, self-limiting, and did not require medical intervention.
Discussion
This study provides preliminary evidence that a single session of anodal transcranial direct current stimulation (tDCS) significantly improves exercise capacity, inspiratory muscle strength, balance, lower limb strength, and gait speed in individuals with COPD. These findings support the potential of tDCS as an adjunctive intervention to enhance physical performance in this population. Consistent with prior research in older adults and neurological populations, these effects are likely mediated by increased cortical excitability, promoting motor learning and neuroplasticity.23,24
Exercise intolerance in COPD is multifactorial, often driven by skeletal and respiratory muscle dysfunction and dyspnea. 2 Anodal tDCS enhances corticospinal excitability, facilitating greater voluntary muscle activation and functional capacity.7,9 It may also modulate diaphragmatic corticospinal pathways, reducing dynamic hyperinflation—a key barrier to exercise in COPD.25,26 The observed increase in 6MWD exceeded the minimal clinically important difference of 30 m, underscoring the clinical relevance of this intervention. 27
The diaphragm and external intercostal muscles, which constitute the primary inspiratory muscles, are innervated by both corticospinal and bulbospinal pathways. 28 In COPD, a shift in muscle fiber composition—particularly a reduction in type II fibers—contributes to diaphragmatic weakness. 29 This study found that anodal tDCS significantly improved maximal inspiratory pressure (MIP) and reduced respiratory rate following exertion. These effects may be attributed to enhanced neuromuscular control of the diaphragm, potentially through modulation of corticospinal excitability.26,30 The reduction in respiratory rate further suggests improved ventilatory efficiency and reduced work of breathing.
Reduced corticospinal excitability in COPD has been implicated in peripheral muscle weakness and impaired physical performance.2,4 Anodal tDCS targeting the leg motor cortex has been shown to increase motor evoked potential (MEP) amplitude and muscle activation, thereby enhancing motor output. 31 In line with these findings, the current study demonstrated significant improvements in gait speed, balance, and lower limb strength following tDCS. The observed enhancement in 4-m gait speed (4MGS) aligns with previous reports in healthy older adults and individuals with multiple sclerosis, further supporting the role of tDCS in augmenting motor function9,32
Limitations
This study has several limitations. The small sample size limits generalizability and statistical power. Only short-term effects were assessed, and the use of convenience sampling may introduce selection bias. Future research should explore optimal stimulation parameters, long-term outcomes, and the integration of tDCS with conventional rehabilitation strategies.
Conclusion
Anodal tDCS appears to enhance exercise capacity, inspiratory muscle strength, and physical performance in individuals with COPD. These findings support its potential role as a non-pharmacological adjunct in pulmonary rehabilitation.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Fund for Supporting Lecturer to Admit High Potential Student to Study and Research on His Expert Program Year 2021 of Khon Kaen University (641JH214).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.