
Abstract
Background
Centre-PR may not be accessible for people living distant from PR centres. Remote digital PR may have equivalent benefits to centre-PR; however, previous trials were potentially biased towards digitally literate patients, and largely excluded participants with a preference for centre-PR. There is limited data on the real-world implementation of, and acceptability for, Digital-PR alone or as an adjunct to other models of PR.
Objectives
To gather patients’ views about the acceptability of Active+me REMOTE, a digital pulmonary rehabilitation app (Digital-PR).
Methods
A qualitative exploratory study using semi-structured interviews with a subset (n = 15) of patients in a mixed method, feasibility study of a hybrid pulmonary rehabilitation, blending Digital-PR with other models of PR. Transcribed data were coded descriptively using Braun and Clarkes’ methodology, data interpretation was facilitated through a Miro virtual whiteboard.
Results
There was appreciation for the concept of Digital-PR, indicated by positive responses in the domains of “friends and family recommendation,” “intention to continue using the app,” and “privacy concerns.” Benefits were reported by two participants who had declined centre-based PR. The app was rated low regarding user-friendliness. Challenges in understanding/using the app and a perception of challenges for others were reported and were associated with poor digital literacy and tech savviness. High digital skills did not predict a favourable assessment of the app as user-friendly.
Discussion
Whilst there was a general appreciation for the concept of digital PR as an adjunct or alternative to traditional centre-based PR, the app did not appear to be user-friendly, nor acceptable to people with low digital literacy. The findings have implications for the wider routine implementation of Digital-PR.
Keywords
Introduction
Pulmonary rehabilitation (PR) is recommended for people with chronic respiratory diseases. It improves exercise capacity, breathlessness, muscle strength and health related quality of life.1,2 Demand for standard centre-based delivery models (CB-PR) supervised by specialist healthcare professionals, outstrips supply 3 and CB-PR may not be accessible for some people. There is interest in digital technology-enabled models of pulmonary rehabilitation (Digital-PR) for increasing capacity, uptake and accessibility. 1 Trial evidence continues to build for Digital-PR as an alternative to CB-PR2,4,5 but there are limited data on the real-world implementation of, and acceptability for, Digital-PR as an adjunct to traditional models of PR delivery.
The Active+me REMOTE App (Aseptika Ltd, St Ives, UK) is a UKCA/CE class I-approved smartphone application (App), which has previously been used in the cardiac rehabilitation setting and shown to be associated with increased patient skill, knowledge, and confidence to manage their condition. 6 However, the acceptability of this app in the pulmonary rehabilitation setting has not been previously studied.
This study presents qualitative findings from a mixed method feasibility study of Hybrid Pulmonary Rehabilitation (Hybrid-PR), a blending of Digital-PR (Active+me REMOTE) with other models of PR, in a real-world setting. 7 The aim of our study was to explore the acceptability of the app among patients with chronic respiratory disease undergoing Hybrid-PR, and to describe potential factors promoting or limiting patient acceptability.
Methods
Design and ethical considerations
The wider feasibility study 7 used a prospective single-centre design and was registered on ClinicalTrials.gov (registration number: NCT05881590). Ethical approval was obtained from the Wales Research Ethics Committee 6 (23/WA/009) and the Health Research Authority on March 29, 2023.
Participant recruitment and eligibility
Participants were prospectively recruited from the Harefield Pulmonary Rehabilitation service in northwest London between May 4, 2023, and August 24, 2023. Inclusion criteria encompassed: (1) Individuals with chronic respiratory disease (COPD, bronchiectasis, interstitial lung disease, and asthma) (2) Age 18 years or older (3) Medical Research Council (MRC) dyspnoea scale score of 2-5
Intervention
The Hybrid-PR intervention offered participants a choice of three PR modalities: (1) CB-PR: A supervised, centre-based programme consisting of two in-person supervised exercise and education sessions weekly for 8 weeks (16 sessions). (2) Video-PR: An 8-week, home-based programme supervised via real-time video-conferencing twice a week (16 sessions). (3) Home-PR: An 8-week home-based programme supervised through a manual and weekly telephone calls.
Additionally, all participants were offered access to Digital-PR, irrespective of their chosen primary delivery model. Digital-PR was delivered through the Active+me REMOTE app (Aseptika Ltd, St Ives, UK).
5
The app facilitated: • Logging of independent exercise sessions, symptoms, and medication • Bluetooth connection to pulse oximeter or manual SpO2 logging • Step counting • Access to physiotherapy-led, pre-recorded exercise classes • Educational sessions with a read-aloud feature
Participants, who did not have access to a smartphone, were offered a pre-paid phone with internet access for the study. All participants received a scheduled 60-minute “onboarding,” in-person, one-to-one session where they were taught how to download/activate the app and use all app features. These sessions were conducted by staff from Aseptika Ltd. Following onboarding, a dedicated support line was made available to all participants by Aseptika Ltd., which offered technical support for the app.
Participants were encouraged to use the app (Digital-PR) to supplement their PR programme. In those undergoing CB-PR or Video-PR, after eight supervised sessions, participants were offered the option of replacing the remaining scheduled supervised sessions with the app only or to continue using the app as an adjunct.
Qualitative study
The nested qualitative study embraced the idea that service users’ acceptance is crucial for determining an intervention’s feasibility. 8 A qualitative exploratory design was used, comprising semi-structured interviews, via virtual video, or by telephone.
Participant characteristics.
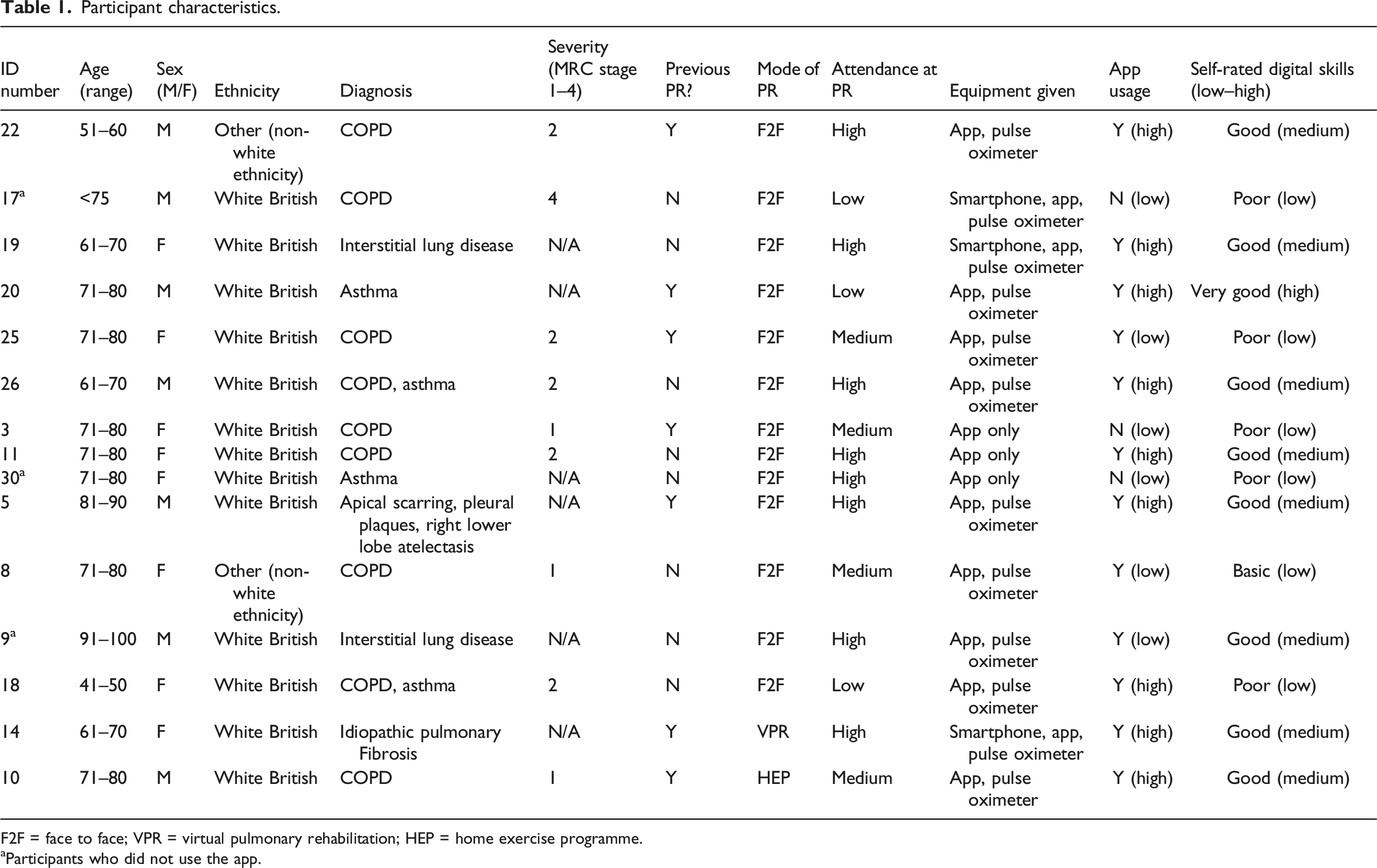
F2F = face to face; VPR = virtual pulmonary rehabilitation; HEP = home exercise programme.
aParticipants who did not use the app.
Data collection
The interview topic guide (Table S2) drew from two technology acceptance questionnaires8,9 Questions were relevant to, behavioural intention to use the technology; perceived usefulness, and the specific context of Hybrid-PR. We undertook a construct validity assessment of the concept of “acceptability,” whereby acceptability is represented as a perception that a given treatment, service, practice, or innovation is agreeable, palatable, or satisfactory according to participants needs, preferences, or expectations. 10 Team members individually assessed the questions in the interview guide (Table S2) to ensure they adequately captured the essence of the construct. The 8-week PR programme ran between 12/9/23–07/11/2023. Interviews took place between 10/10/23–18/12/23 and within 4 weeks from the end of the initial 8-week period of App usage. Two independent researchers (PK-D and OFM) conducted the interviews, which ranged in duration from 15–75 minutes. Recruitment was stopped when thematic saturation 11 was reached, in the data analysis.
Data analysis
Thematic analysis followed Braun and Clarke’s
12
approach. Descriptive codes were generated and ordered into categories according to question clusters of the interview guide (using NVivo version 14, Figure 1) and subjected to interpretation, according to theoretical conceptualisations of “acceptability,” using concept mapping in the online whiteboard, Miro,
13
and through a collaborative, peer review approach to minimise bias.
14
Relationship between descriptive coding and interpretative coding.
Results
The sample consisted of 47% men (n = 7) and 53% women (n = 8). Eight (53%) were ≥75 years old and seven (47%) were aged <75 years (see Table 1 for further details) Thirteen (86%) were White British and two (13.3%) were of Other (non-white ethnicity). Nine (64%) were diagnosed with mild-to-severe COPD and six (36%) had other chronic respiratory conditions. Some participants were provided additional health monitoring equipment (e.g., pulse oximeters (n = 9), which were not necessary to undertake PR or to use the app), or loaned basic model smartphones with pre-paid data for the study duration (n = 3).
Mode of delivery, attendance and app usage
Most participants (n = 13, 87%) opted for CB-PR (F2F). One, (6%) for Video-PR (VPR) and another participant (6%) opted for Home-PR (HEP). Eighty percent of participants (n = 12) had medium to high attendance at PR, 3 (20%) had low attendance.
App usage and self-rated digital literacy and skills
App usage was divided into tertiles of % of days used over the 8-week intervention period (<33%, 33–67%, >67%) and defined as opening the APP and engaging in an app-related activity.
Overall, app usage was high (60%). There was an association between app usage and participants’ self-rating of their digital literacy and skills, (see for example15,16 for similar self-reporting approaches to the assessment of digital skills). The two participants who opted for remote, VPR/HEP, self- rated as having good digital skills and had high app usage. They were among participants who provided favourable evaluations through satisfaction and intention to use it (see interpretative themes). Some participants, (n = 3, 20%), although selected because of some interaction with the app, indicated no use or minimal use of it. These participants reported challenges in understanding/using the app. They were among those who self-rated as having low digital skills (n = 6, 40%, see Table 1) or indicated that they required further training and support. Exceptionally, participant 9 reported good digital literacy yet had low app usage. Most participants who had high app usage (n = 9, 60%) self- rated as having medium or high (good) digital skills. Exceptionally, participant 18 had high app usage despite a self-rating of low digital skills.
Interpretative themes
Six interpretative codes were developed (Figure 1) in accordance with concepts of effort expectancy, performance expectancy and agreeability: (a) satisfaction and perceived benefits, (b) intention to continue using it, (c) friends and family recommendation, (d) perceived challenges/disadvantages for others (barriers, burdens), (e) perceptions of user-friendliness/ease of use, (f) privacy concerns. Figure 1 provides an overview of the weighting of acceptability (high vs low) 1 in these domains and shows the process of mapping quotes to descriptive codes and subsequent interpretations of high/low acceptability (NB not all participants provided a rating/response in all domains). The interpretations are discussed in more detail below.
Satisfaction and perceived benefits
There were mixed ratings/responses relating to satisfaction with the Active+me REMOTE app. Four participants (27%) evaluated the app as highly satisfactory. Among them was participant 14, (opted for VPR), who indicated that the app was motivating.
2
…I can see a pattern of how I am. … the exercise classes starting with this sitting one. They were quite good. And they were different to what I was taught when we did the pulmonary rehab online with the team at [Hospital]. … I found it quite motivating. (P14)
Likewise, P19, reported a benefit through being able to participate in remote-PR when they were unable to attend CB-PR. …it did benefit, some days I couldn’t come to the class, on those days I could continue by using the app and following the exercises. I didn’t feel as if I was giving up. I could just continue it in my own time. So it helped just to supplement the course (P19)
Conversely, eight participants (53%) indicated low satisfaction. For example: I didn’t feel happy. …, I can’t say I benefitted a lot from using it. I felt maybe the app could have done more for me … (P8)
Three participants reported that they did not use the app at all; two of these people indicated that they didn’t engage because they felt they needed further training/support to use the app [P17 and P30] and one person indicated that they didn’t see a reason for using the app alongside CB-PR. Notably, these explanations correspond to two reasons for declining Digital-PR only (in the main study), i.e., enjoying or finding CB-PR motivating or not being able to use the Active+me Remote app/Digital-PR independently.
Intention to use
The participants were given the App for free for 12 months. As per the ethical approval, we collected app usage data for 8 weeks from the time the participant received the app. There was no ethical approval to collect objective App usage data beyond this 8-week period although participants could continue to use a limited version of the app.
High acceptability through intention to use was indicated (Figure 1), by nine people (60%). Only three (including participants 10 and 14) did so categorically, however. For example: I plan to use the app to record the use of my inhalers, and to follow any pulmonary rehab lessons and [to read] any more articles. (P10)
The majority indicated a tentative intention to use the app, e.g., if future need for PR arose. For example, P22 and P18. If I start doing the physio again then I’ll start using it. I don’t really need it now. (P22) I’m gonna still use it. I’ve got it for a year and then obviously it will go on to the pay (P18).
Among participants who self-rated as having low digital skills/literacy, there was no intention to use the app in future, e.g.: I don’t know what I’m doing with it. If I was computer literate, yes, I would but we’re just not compatible (P3).
Friends and family recommendation
A high percentage, (11/15, 73%), of participants indicated friends and family recommendation. Some gave caveats, namely, challenges might arise for others, therefore the digital/computer literacy of the person would be a consideration (e.g., P8 and P5 below). If they are more computer literate than me, I would tell him about the app …it depends on the person. (P8) I’d go back to being technology savvy … I’m sure it would benefit somebody who understood it all from top to bottom, I found it a minefield. (P5)
Perceived challenges for others
Six participants (excluding those who did not use it) perceived challenges for others, relating to poor digital literacy/ fear of technology and understanding the benefits of the app. Some people of my age and older will struggle…, they struggle with computers anyway. (P10) On the course, all bar a couple of people were older than me. I heard them saying things like-… “apps, I don’t even know what an app is, don’t get me to try and start using one of those things,” They take the view that they're getting older and that’s for younger people. (P26) People I met in these groups, to what extent they have any computer skills at all, I’d be surprised. I could imagine them getting in a right panic. (P17)
The biggest challenge-you have to demonstrate the benefits of using the app. (P20)
Six other participants indicated no challenges or that challenges could be overcome with better explanation/training. For example, I think they need to get it explained to them a bit more, some people might feel daunted by it and think it’s too difficult [to] navigate. (P14)
User-friendliness
User-friendliness was rated/ indicated qualitatively as low, (between 4-5/10), by six participants, as below. 4 or 5/10, I gave up towards the end, I thought “this is just getting too much for me. (P5) I would say 5 or 6/10. I’ve always had phones and laptops, and my PC, so I’m not completely ignorant of things, but I did find it complicated. (P11) I got in a bit of a pickle with it. It wouldn’t do what I was expecting it to or what I was asking it to. (P25) For a person that’s dyslexic It isn’t friendly. I was getting flustered and frustrated (P18) I don’t find the information easy to see, it’s an awful lot of work to put in. I haven’t really understood the charts. (P20) No matter how much I tried, I couldn’t make it out. (P3)
Six other participants indicated user-friendliness as high (between 7-8/10), some noting better understanding with familiarisation and use support, as below: Initially, it was a little uncomfortable. But once I got through the first week of using it then it was all very straightforward. (P10) To start off with, it was moving around the app to get to find the information I wanted. I was shown them, if I hadn’t had that, I probably would have but I had a session with them …and they showed me how to connect everything together. And how to use the app. I found that useful. (P14)
Five of these people, also self- rated their digital skills as high. However, having high digital skills did not predict better ease of use, three people who self-rated their digital skills as medium/high also reported usage difficulties. Only P8, who self-rated their digital skills as low, rated user-friendliness as high.
Privacy concerns
Data privacy was not reported as a significant concern among participants. This was the strongest domain of high acceptability. However, a sense of trust in the hospital as gatekeeper was also expressed by three participants (P5, P19 and p22). Some participants perceived additional background monitoring by their clinicians, (see P10 and P14 below) which provided some reassurance. I don’t have any problem with any of that. I'm very open. There’s nothing there that bothers me. (P10) .. it’s not something that makes me say, oh my God, I must go and check their data protection stuff or anything like that. So, that's not a big issue. (P20) I’d just trust it because it was at the hospital who were doing it. … It was a trusted medical professional setting. So, I felt safe. They’ve got all your medical data anyhow. (P19) I knew it was developers, but because they were in the hospital setting, I’m assuming that the hospital have approved what they’re doing and they’ve looked into it and they’ve allowed it. … Put them as sort of the gatekeeper. I was assured that it was all confidential. (P5)
Discussion
This study is the first to explore the patient acceptability of using a Digital-PR app as an adjunct to other PR modes of delivery, primarily CB-PR and the first study to evaluate the Active+me REMOTE app in the pulmonary rehabilitation setting. Despite structured onboarding, the provision of necessary equipment and a technical helpline, a significant proportion did not use the app at all. 7 Of those who did utilise the app, there were mixed views around acceptability (Figure 1).
This was a qualitative study nested within a feasibility study of Hybrid-PR, blending Digital-PR with traditional supervised models of PR (see Ref. 7). This feasibility study demonstrated that only 35% of 69 participants were engaged (defined as activating Active+me REMOTE app at least weekly for 8 weeks) with Digital-PR despite the provision of necessary equipment and the app free of charge, as well as considerable technical support through in-person onboarding and a technical helpline (see Ref. 7). The results from this qualitative study suggest that poor digital literacy and skills was a barrier to engagement with the app.
For those who did engage with the app, there were some positive views supporting acceptability, including perceived benefits (e.g., flexibility to partake in PR activities around own schedule, using it as a substitute for missed scheduled classes, features that encouraged self-monitoring); intention to continue using the app in the future; willingness to recommend to friends and family, and low concerns about privacy/security (Figure 1). Conversely, there was a recognition that the app might be challenging to use for those with poor digital literacy and skills, and there were mixed views about the user-friendliness of the Active+me REMOTE app. These findings indicate that challenges may be encountered if this app is incorporated into PR services in its current format.
Contexts of our study (digital-PR app used as an adjunct to hybrid models of PR; real-world setting) differ from those described in similarly evaluated, technology-enabled PR studies (e.g., Refs. 17, 18, 19, 20, and 21). However, some of our findings are consistent with those identified in recent studies and thus strengthen the evidence base. Of note, the convenience and flexibility of technology-enabled PR is evidenced16,20 and patient satisfaction and appreciation for app features that track progress and motivate participants to exercise is also commonly reported.16,19,20 These findings suggest partial acceptance among PR users for technology-enabled PR. Similarly poor digital literacy, perception of use difficulties and scepticism associated with using technologies are commonly reported as barriers to engagement with digital models of PR.18,20,22 These latter findings along with reported preferences for in-person PR 20 suggest that Digital-PR may be limited to a select cohort of PR users- those who are technologically literate and skilled.
There is also clear indication from previous studies that PR patients benefit from ongoing clinician support.16,17,19 This is consistent with findings of a preference for in-person PR. 20 Patients in these studies of technology- enabled PR reported benefits such as, effective participant–clinician relationship, facilitating orientation to the PR programme and technologies 16 clinicians motivating, encouraging 16 and reassuring them, 19 clinicians addressing concerns quickly and troubleshooting the technologies.18,19 The support offered by the app developers Aseptika, in this study, to understand and use the app was reported as useful, and there was also built in notifications designed to motivate participants. However, given the prominence of findings in the literature of the added benefits of clinician support, it is an important point of consideration for the model of PR adopted for Active+me REMOTE app. Notably, there was indication in this study, that participants perceived monitoring by their clinicians. This may have provided a degree of tacit clinician motivation and reassurance.
Strengths and limitations
There are some noteworthy strengths of this study. Firstly, our approach, using Digital-PR as an adjunct to, rather than replacement of, CB-PR is novel. The feasibility study is also one of the first to evaluate the implementation of a smartphone app, which was offered to all participants irrespective of their digital literacy. Additionally, whereas some similar studies were authored by investigators with potential conflicts of interest (e.g., Refs. 4 and 5) our evaluation was made by researchers without conflicts of interest, and independently of the manufacturer of the smartphone App, Aseptika.
However, there are limitations. Despite purposive sampling, findings may not be generalisable to patients with different demographic profiles or those who live in different settings. Future studies might focus on specific patient phenotypes who might particularly benefit from the flexibility of remote digital technologies (e.g., housebound with very severe lung disease, those living in areas with limited access to CB-PR). Our approach to the assessment of digital skills, i.e., participants perceptions and self-reporting/rating, may have introduced reporting bias 21 as participants may have overestimated/underestimated their digital abilities, affecting their experiences with, or perceptions of the application. Whilst more objective measure of participants computer literacy such as used in recent studies (e.g., Ref. 20) and less contemporary measures like eHEALS 22 are available, it is notable that these tools are also based on self-reporting. Additionally, there is often a focus on the ability of participants to use the internet to find health information which do not necessarily cover the whole range of skills (or access to equipment) participants need to use an app. Our findings are specific to the Digital-PR app, Active+me REMOTE. Aspects around user friendliness cannot be extrapolated to other apps used for supporting PR delivery e.g., 23 and 24.
Conclusions
In conclusion, this study of acceptability among patients undergoing hybrid models of PR has shown that patients find the Active+me REMOTE app acceptable in that it provided flexibility and convenience and encouraged and motivated participants to self-monitor. These findings suggest that it is partially acceptable, as an adjunct to traditional models of PR among some patients, with chronic respiratory conditions but may not be applicable as a widespread service for the population under study, due to reported usage difficulties and a perception of challenges for others.
Supplemental Material
Supplemental material - Acceptability of a digital pulmonary rehabilitation app as an adjunct or alternative to usual care for people with chronic lung diseases: A qualitative study of patients’ views and experiences
Supplemental material for Acceptability of a digital pulmonary rehabilitation app as an adjunct or alternative to usual care for people with chronic lung diseases: A qualitative study of patients’ views and experiences by Pamela Knight-Davidson, Oluwasomi Festus Meshe, Timothy O Jenkins, George D Edwards, Suhani Patel, Carmel Moore, Karen Hayden, Graham Ball, Karen A. Ingram, Claire M. Nolan and William D-C. Man in Chronic Respiratory Disease
Footnotes
Acknowledgments
The authors gratefully acknowledge the Harefield Pulmonary Rehabilitation Unit for facilitating this study and the participants.
Authors’ Contributions
Study design and procedures: PK-D and OFM, TOJ, WM and SP; Data collection: PKD and OFM. Analysis and interpretations: PK-D and OFM; Manuscript PKD, OFM, TOJ and WM; Critical feedback on the manuscript: SP, CM, GB, KH, CN, KI, GE
Funding
The authors received financial support for the research, authorship, and/or publication of this article; NHS Accelerated Access Collaborative through a Small Business Research Initiative (SBRI) healthcare award. Neither funder nor Aseptika Ltd played a role in the design, analyses, data interpretation, nor decision to submit results.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.