
Abstract
Ghrelin, an endogenous ligand for growth hormone secretagogue receptor, has been implicated in chronic obstructive pulmonary disease (COPD). Recently, several studies reported inconsistent levels of ghrelin in plasma/serum of COPD patients. This meta-analysis aims to determine the circulating level of ghrelin in COPD. Published case–control or cohort studies were retrieved from Pubmed and Embase databases. Pooled standardized mean difference (SMD) with 95% confidence interval (CI) was calculated in a random-effects model. Nine studies involving 515 subjects were included. Pooled effect size showed that circulating ghrelin levels were significantly enhanced in COPD patients compared with those in controls (SMD: 0.83, 95% CI: 0.04 to 1.62, p = 0.039). Noticeably, five studies stratified for body mass index in COPD group and we further found ghrelin levels were significantly higher in underweight COPD patients than those in normal weight cases (SMD: 1.52, 95% CI: 0.43 to 2.61, p = 0.006). However, no significant difference regarding ghrelin levels was indicated between normal weight COPD and controls (SMD: 0.64, 95% CI: −0.36 to 1.63, p = 0.210). In this meta-analysis, circulating level of ghrelin is significantly elevated in patients with COPD, especially in those underweight, indicating supplement with exogenous ghrelin could be a therapeutic choice for underweight COPD patients.
Introduction
Chronic obstructive pulmonary disease (COPD), a worldwide disease characterized by persistent airflow limitation, often develops progressive muscle dysfunction and malnutrition. 1 Those abnormalities are independent of the degree of airflow limitation and even contribute to poor prognosis and mortality. 2 Mechanisms underlying muscle dysfunction and malnutrition in COPD remain not very clear. 3
Ghrelin, a peptide of 28 amino acids, was first discovered in the stomach in 1999. 4 It is an endogenous ligand for the growth hormone secretagogue receptor (GHSR), which has a variety of physiological functions, including modulation of food intake and energy expenditure, improvement of cardiac performance, stimulation of gastric motility, as well as regulation of glucose metabolism and thermogenesis. 5,6 Meanwhile, therapeutic value for ghrelin has been also reported, such as relieving gastroparesis symptoms in gastroparesis, stimulating hunger and feeding in anorexia nervosa, and increasing peak oxygen consumption and peak workload during exercise in chronic heart failure. 7 –9
In addition, ghrelin levels have been found to be altered in pulmonary diseases, such as COPD and pulmonary hypertension. 6 Several studies recently examined the level of ghrelin in plasma/serum of COPD patients and suggested it might serve as a biomarker relating to weight loss and pulmonary dysfunction in COPD. 10 –18 However, although the circulating ghrelin was reported to be higher in COPD patients in six of these studies, 10 –15 the other three informed conversed results. 16 –18 Meta-analysis has been considered to be a useful means to pool the independent statistical powers and thus achieve a quantitative understanding of inconsistent results. Therefore, we performed this meta-analysis to draw a pooled conclusion on the level of circulating ghrelin in COPD patients.
Methods
Search strategy
To identify all published studies relevant to ghrelin and COPD, literature search was performed using the databases including Pubmed and Embase. The search terms used were (1) ghrelin and (2)chronic obstructive pulmonary disease, chronic obstructive airway disease, chronic airway disease, and COPD (Figure 1).
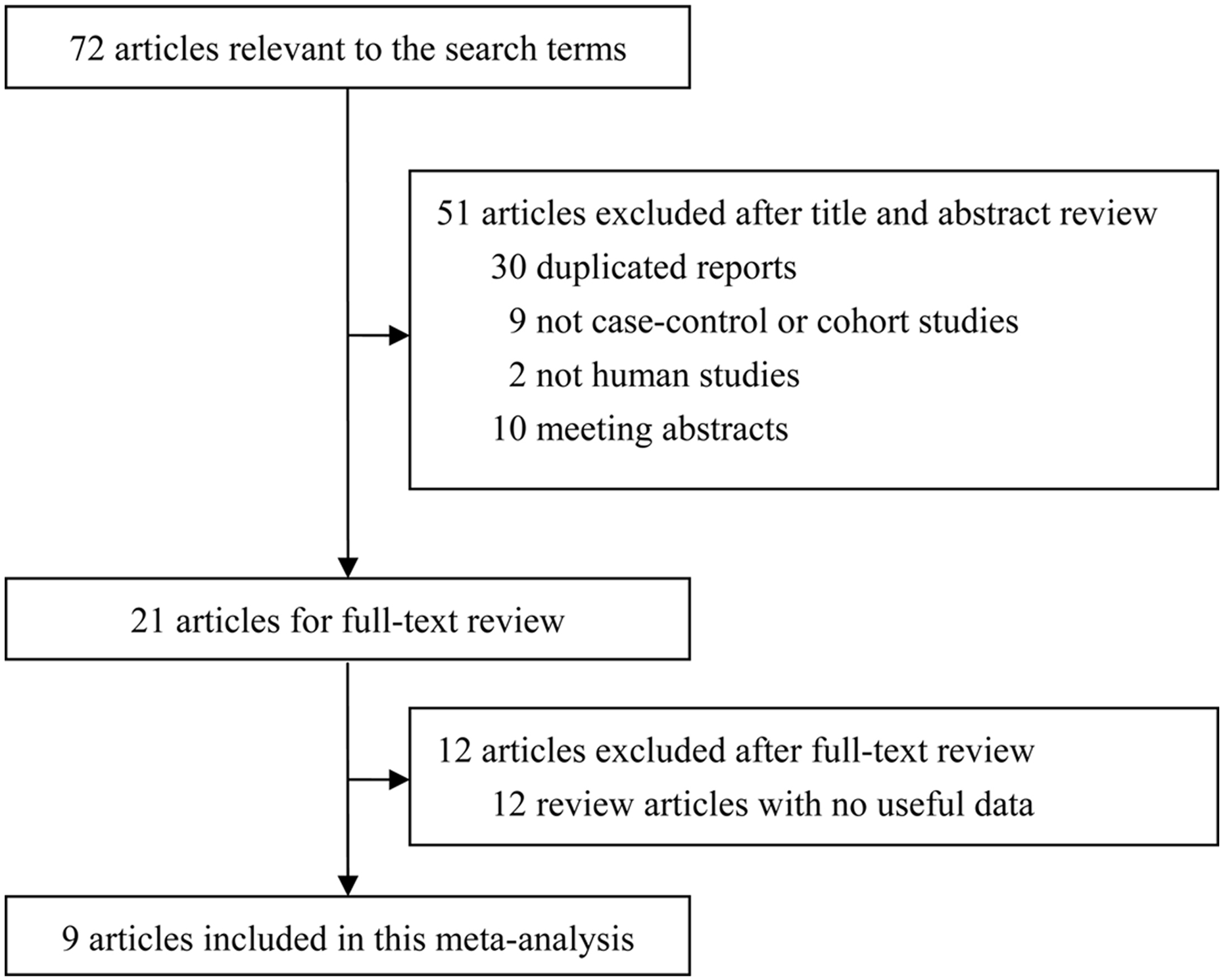
Flow diagram of search process.
Data extraction
Two independent reviewers collected the data according to inclusion and exclusion criteria. Inclusion criteria were retrieved case–control or cohort studies which clearly informed the circulating level of ghrelin in COPD patients and controls. Exclusion criteria were (1) non-case–control or non-cohort studies, (2) nonhuman study, (3) duplicated report, (4) meeting abstract, and (5) review articles with no useful data. Unpublished data were not considered. Disagreement was resolved by discussion before reaching a consensus.
Quality assessment
To assess the quality of the included studies, two reviewers independently rated the studies according to the Newcastle–Ottawa quality assessment scale for case–control study. The Newcastle–Ottawa scale (NOS) contain three main aspects: selection of subject (0–4), comparability of cases and controls (0–2), and exposure of subject (0–3). Studies were considered as high qualities if their total scores were 7–9. When disagreement existed between the two reviewers regarding the NOS scores, a discussion would be carried out.
Statistical analyses
Due to the different measuring methods with various units for ghrelin, continuous variables were presented as standardized mean differences (SMDs) with 95% confidence intervals (CIs). Pooled SMD with 95% CI was calculated and p < 0.05 was accepted with statistical significance. Heterogeneity was checked by the Q test. Meta-analysis was done with the fixed-effects model when there was no heterogeneity (p ≥ 0.1). Otherwise, the random-effects model was used. The leave-one-out sensitivity analysis was performed by removing one study each time to check if individual study influenced the pooled results. Funnel plots, as well as the Begg’s rank correlation test and Egger’s linear regression test, was used to inspect the potential publication bias, and p < 0.05 was considered significant publication bias. All analyses were conducted using Stata 11.0 (Stata Corp LP, College Station, TX, USA).
Results
Characteristics of included studies
Seventy-two studies were relevant to the search terms. After reviewing the titles, abstracts, and articles, 63 studies were excluded and thus 9 studies matched the inclusion criteria. The nine included studies had been carried out in China, Japan, Turkey, and Sweden. The main features of the studies included in this meta-analysis are presented in Table 1.
Clinical features of included studies.

UW: underweight; NW: normal weight; COPD: chronic obstructive pulmonary disease; N: number; RI: radioimmunoassay; EI: enzyme immunoassay; LFT: lung function test; Ref: reference; NOS: Newcastle–Ottawa scale; BMI: body mass index, NR: not reported; FEV1: forced expiratory volume in one second; FVC: forced vital capacity.
Quantitative synthesized results
All included studies measured ghrelin levels in patients with COPD and control subjects. Pooled effect size showed that circulating ghrelin levels were significantly higher in COPD patients than those in the healthy controls (SMD: 0.83, 95% CI: 0.04–1.62, p = 0.039; Figure 2). Noticeably, five studies stratified for BMI in COPD group: underweight (BMI ≤ 21 kg/m2) and normal weight (BMI > 21 kg/m2). Due to the importance of ghrelin in body weight, we further found that ghrelin levels were higher in underweight COPD patients than those in normal weight cases (SMD: 1.52, 95% CI: 0.43–2.61, p = 0.006; Figure 3). However, no significant difference regarding ghrelin levels was indicated between normal weight COPD patients and controls (SMD: 0.64, 95% CI: −0.36 to 1.63, p = 0.210; Figure 4).
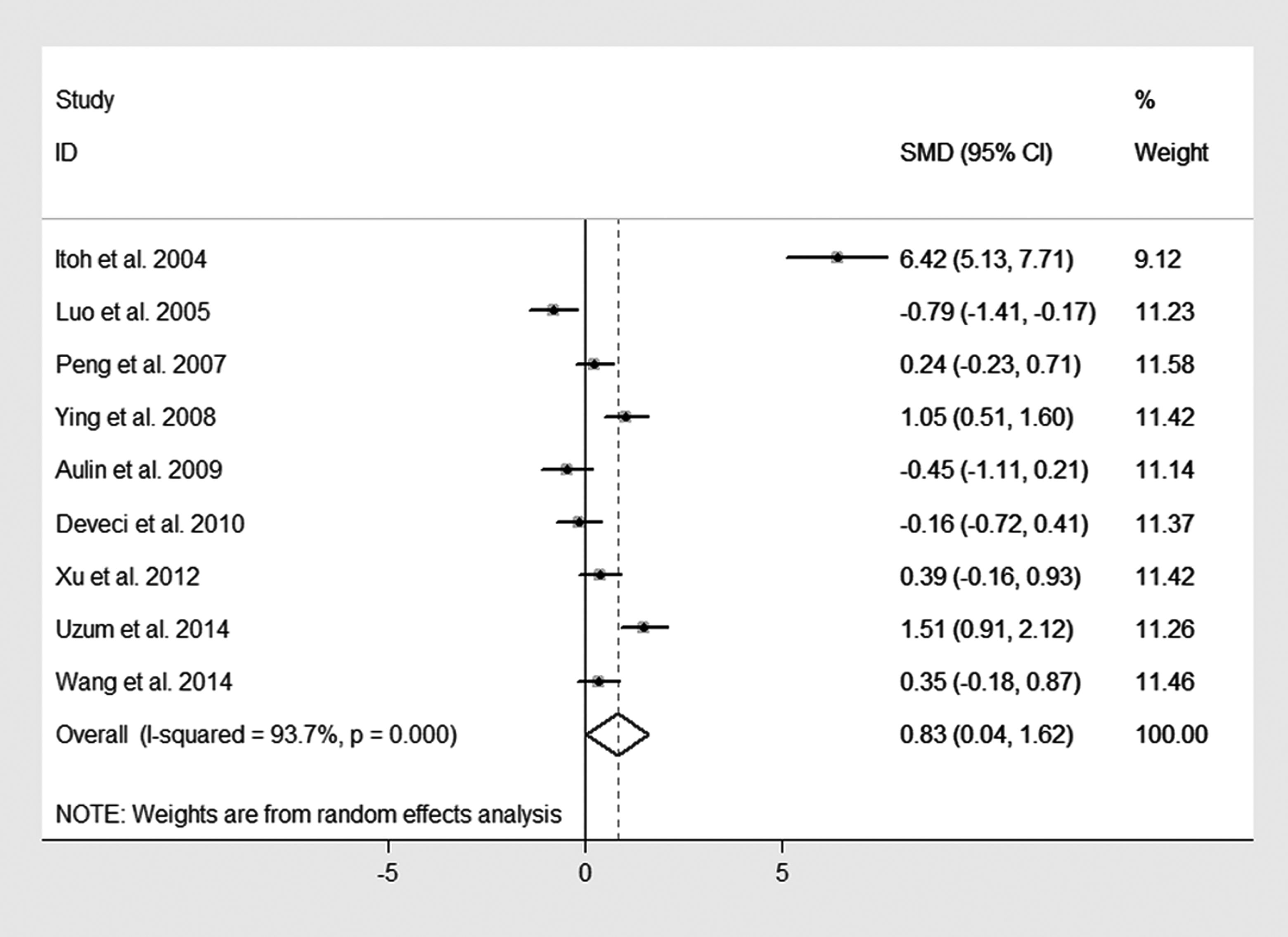
Forest plots of SMD with 95% CI for the circulating level of ghrelin in COPD patients compared with controls. SMD: standardized mean difference; CI: confidence interval; COPD: chronic obstructive pulmonary disease.

Forest plots of SMD with 95% CI for the circulating level of ghrelin in underweight COPD patients compared with normal weight cases. SMD: standardized mean difference; CI: confidence interval; COPD: chronic obstructive pulmonary disease.

Forest plots of SMD with 95% CI for the circulating level of ghrelin in normal weight COPD patients compared with controls. SMD: standardized mean difference; CI: confidence interval; COPD: chronic obstructive pulmonary disease.
Heterogeneity and sensitivity and publication bias
Significant heterogeneity was revealed among all studies in the meta-analysis. To identify the source of heterogeneity, subgroup analyses according to sample origin and assay methods were performed. However, the heterogeneity still remained significant in the subgroup analyses. Further, the leave-one-out sensitivity analysis was performed to check the influence of individual study on the pooled results. Interestingly, after removal of the three studies each time, 10,12,15 the pooled results were altered significantly as follows: 0.27(−0.21 to 0.76); 0.75(−0.10 to 1.59); 0.81(−0.07 to 1.70), respectively, which possibly owed to the different sample origin and assay methods in these studies. Although the funnel plots showed some asymmetry in the studies (Figure 5), publication bias was not suggested by Begg’s rank correlation test (p = 0.602) and Egger’s linear regression test (p = 0.180).

Begg’s funnel plots for evaluation of publication bias in the included studies on the circulating level of ghrelin in COPD patients compared with controls. COPD: chronic obstructive pulmonary disease.
Discussion
Ghrelin, a bioactive peptide, is mainly synthesized in the stomach, which plays an important role in regulating body weight. Through binding to GHSR-1a, ghrelin can stimulate growth hormone release and provide signals to the nervous system which increase food intake and reduce fat utilization and energy expenditure, which in turn contributes to weight gain. 19 –21 Moreover, weight loss can lead to increase in circulating ghrelin level. 22 COPD patients are usually complicated with extrapulmonary disorders, including weight loss and muscle dysfunction. BMI and percentage of body fat, as well as FEV1% pred (FVC% pred), were found to be negatively correlated with serum ghrelin levels in COPD cases. 13,14 In our meta-analysis, circulating ghrelin level was significantly increased in COPD patients, especially in those underweight. However, no significant difference of circulating ghrelin level was revealed between normal weight COPD patients and healthy controls. These data indicate a compensatory mechanism of ghrelin for body weight loss in COPD. 3
In a COPD model of chronic cigarette smoke-exposed rats, skeletal muscle strength, respiratory function, and emphysema were ameliorated after ghrelin administration, but neutrophils in the bronchoalveolar lavage fluid were not inhibited by ghrelin, 23 supporting the potential compensatory mechanism for ghrelin, which may be not related to inflammatory response, but nutritional status in COPD. Clinically, Nagaya et al. reported that administration of ghrelin in cachectic COPD patients could increase body weight and respiratory muscle strength. 24 Recently, Miki and his colleagues further performed a multicenter, randomized, double-blind, placebo-controlled trail, indicating underweight COPD patients benefited from intravenous treatment of high-dose ghrelin (2 µg/kg) twice daily for 3 weeks with improvements in St. George Respiratory Questionnaire score, exercise capacity, ventilatory–cardiac parameters, and exertional cardiac function. 25 –28 These data further suggest that compensation with exogenous ghrelin may be a potential choice in treatment of underweight COPD patients.
Noticeably, ghrelin levels were measured using radioimmunoassay (RI) or enzyme immunoassay (EI) in these studies. These two methods have strong specificity and sensitivity by using an enzyme- or radioisotope-labeled antibody/antigen. RI does not use enzymes, thereby reducing the risk of influence from cleaning and concentration of the samples, but radioisotope exposure is not fully avoided. EI can better distinguish between the more modest changes, but it might have a less effect of nonspecific competition by plasma proteins. 29 Thus, it is difficult to tell which one is better.
When applying the results in the present study, some limitations should be taken into account. First, these studies had small sample size and might not have adequate power. Second, lack of the original data in the studies limited our further analysis, such as adjustment with confounded factors and source of heterogeneity. Third, conference proceedings and unpublished articles were not included. Finally, these studies were cross-sectional analysis and it was unable to establish causation.
Taken together, in this meta-analysis, circulating level of ghrelin is significantly elevated in patients with COPD, especially in those underweight. However, no significant difference of circulating ghrelin level is revealed between normal weight COPD patients and healthy controls. A compensatory mechanism may be the reason for those results and thus ghrelin as a complementary treatment for weight loss in COPD is encouraging. However, large-scale randomized trials are needed to verify the effect of ghrelin in COPD.
Footnotes
Author contribution
Xue Zhang, Ting Yang, and Junli Wang contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grant 2017SZ0120 from the Key Research Development Program of Sichuan Province and grant 17PJ009 from the Health and Family Planning Commission of Sichuan Province and grant 81200031 from the National Natural Science Foundation of China.