
Abstract
This study aimed to determine the physical activity level of people admitted to hospital with an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and whether physical activity changed immediately after discharge and 6 weeks post hospital admission. In this prospective observational study, people admitted to hospital with an AECOPD had physical activity levels monitored using the SenseWear® Armband (model MF-SW) for 3 days in hospital (T1), during the first week at home following discharge (T2), and at home during the sixth week after admission (T3). Fifty participants (mean age (SD) 71 (10) years) completed the study. There was a linear increase in average steps per day over the three time periods (T1, mean (SD) 1385 (1972) steps/day; T2, 2040 (2680); T3, 2328 (2745); analysis of variance (ANOVA) p = 0.001) and time spent in moderate activity (3.0–6.0 metabolic equivalents; minutes/day) (T1, mean (SD) 16 (27) minutes/day; T2, 32 (46) minutes/day; T3, 35 (58) minutes/day; ANOVA p = 0.008). For both outcomes, post hoc t-tests showed significant improvements from T1 to T2 and from T1 to T3, but not between T2 and T3. Physical activity was low in hospital and significantly improved in the week after discharge but showed no further significant improvement at 6 weeks following a hospitalized AECOPD.
Introduction
Chronic obstructive pulmonary disease (COPD) remains a leading cause of global morbidity and mortality and substantially increases economic and social burden. 1 Mortality risk increases in those who experience an acute exacerbation of COPD (AECOPD) requiring hospital admission. 2 Furthermore, people with COPD are at higher risk of hospital readmission for exacerbations if they have low levels of daily physical activity. 3
There have been very few studies to examine the levels of physical activity in people experiencing an AECOPD, 4,5 despite the growing literature on physical activity in people with stable COPD. 6 –9 Two small studies in participants with COPD (17 and 20 participants, respectively) examined physical activity outcomes during hospitalization and 1 month following discharge. 4,5 The measurement period in both studies was limited being a 12-hour period over 1 to 2 days. 4,5 The results in both studies indicated that physical activity was low in people with COPD during hospitalization and improved 1 month following discharge, but the levels remained lower than people with stable COPD. The time course of improvement was not indicated by these studies. Given the advances in physical activity monitoring devices, continuous measurement over several days is now more viable, enabling further examination of physical activity during and after hospitalization in larger numbers of people with COPD.
In Australia, there is an increasing drive to reduce the length of hospital stay for people with an AECOPD in order to reduce costs and increase availability of acute beds. 10 It is conceivable that earlier discharge from hospital may impact on physical activity levels. Understanding physical activity levels during and following hospital discharge may help to inform future interventions which may reduce hospitalization and improve disease management after an AECOPD.
The primary aim of this study was to quantify the time course of change in physical activity levels by measuring physical activity during hospitalization for AECOPD and then during the first week at home after discharge and again at home during the sixth week after the original date of hospital admission. We hypothesized that there would be an increase in physical activity from hospitalization to the first week at home, with a further increase by 6 weeks following hospital admission. The secondary aims of the study were to (1) examine the pattern of physical activity within the hospital admission period and (2) determine the change in lung function, functional exercise capacity and physical performance and health and psychological status from the day of discharge to 6 weeks following hospital admission.
Methods
Participants
Participants were recruited from an inpatient respiratory ward at a major tertiary hospital in Sydney, Australia, if they met the inclusion criteria of a primary medical diagnosis of an AECOPD. The participants were recruited on day 1 of their hospital admission and were either newly diagnosed people with COPD or previously diagnosed with COPD with an acute exacerbation. The diagnosis of an acute exacerbation was determined by a respiratory physician with criteria of increased dyspnoea, increased sputum production and change in sputum colour, which required treatment with corticosteroids and/or antibiotics in patients with documented COPD as defined by Global Initiative for Obstructive Lung Disease (GOLD) criteria. 11 Participants were excluded if there was cognitive impairment (mini–mental state examination score <24), unstable cardiac or neurological disease, requirement to use a walking aid for mobility, were unable to understand English, were unable to use the physical activity monitor independently or lived in rural areas that would make it difficult to return for final testing (i.e. 6 weeks post admission date) at the hospital. Medical notes were reviewed on the ward by the investigators to screen appropriate participants who were included if they met the inclusion and exclusion criteria and gave written consent.
Study design
This prospective, observational study was conducted over a 7-week period with three assessment points. Participants were initially assessed on days 2, 3 and 4 of the hospitalization period (T1). Standard medical and physiotherapy (chest physiotherapy and gentle mobilization with no formal rehabilitation) care was provided over the course of this admission. The participants were next assessed over the 7 days at home following discharge (T2), and final assessment was 6 weeks after the hospital admission date (T3). The study was approved by the South Eastern Sydney Local Health District Human Research Ethics Committee. The trial was registered in the Australian New Zealand Clinical Trials Registry (ACTRN12611000369921).
Outcome measures
Physical activity
The SenseWear®Armband (SWA; BodyMedia®, Pittsburgh, Pennsylvania, USA) was used to measure participants’ physical activity levels at T1, T2 and T3. The SWA was worn on the left upper arm over the triceps muscle and incorporated a triaxial accelerometer and physiologic sensors that provided an indication of energy expenditure. The SWA has been validated for estimating energy expenditure in people with COPD. 12,13 Participants were asked to wear the SWA for 24 hours/day, with the exception of the time spent showering or participating in other forms of water immersion such as swimming. Participants wore the SWA for a maximum of 3 days during T1 (second to the fourth day of hospital admission) and for 7 days during each of T2 and T3. Total energy expenditure, steps, metabolic equivalents (METs) and active energy expenditure (energy expenditure >3 METs) were measured every minute. Physical activity level per day was also determined using the following five categories: sedentary (0–1.5 METs), light (1.5–3.0 METs), moderate (3.0–6.0 METs), vigorous (6.0–9.0 METs) and very vigorous (≥9.0 METs). An a priori criterion for the definition of a ‘completer’ was at least 3 days of recorded measurements in each of T1, T2 and T3 with ≥85% (20.5 hours) wear time in each 24-hour time period. Participants with incomplete data, based on less than 3 days of 85% wear time during T1 or T2 or T3, were excluded from analysis. SWA data were downloaded using the accompanying software (SenseWear Professional 8.0; BodyMedia).
Pulmonary function test
Forced expiratory volume in one second (FEV1) and forced vital capacity (FVC)) were measured using the Micro Medical Microlab MK8 spirometer (Care Fusion, Chatham, Kent, UK) and was performed according to recommended guidelines. 14
Exercise capacity
Exercise capacity was assessed by the 6-minute walk test (6MWT) on the day of discharge and at T3. A hospital corridor that was 15 metres long was used for the walking track, which was the space available on the acute respiratory ward where testing was conducted. The majority of participants (70%) were familiar with the 6MWT, having completed a 6MWT previously. On the day of discharge, all participants completed one test only because it was felt that participants were recovering from an AECOPD and would not be able to manage two tests. At T3, participants completed two 6MWTs on the same 15-metre walking track, separated by a period of at least 30 minutes, with the best result used in the analysis. Self-reported dyspnoea at rest and during exercise was measured on the modified Borg 0 to 10 category ratio scale for dyspnoea. 15 Reference values for the 6MWT were based on an Australian study of healthy individuals. 16
Physical performance
Physical performance was assessed using the Functional Performance Inventory–Short Form (FPI-SF) designed to evaluate functional performance in people with COPD in six domains including body care, maintaining the household, physical exercise, recreation, spiritual activities and social interactions. 17
Health performance
COPD health status was assessed using the COPD Assessment Test™ (CAT), which is positively related to exercise capacity. 18
Dyspnoea
Dyspnoea was assessed with the Modified Medical Research Council (MMRC) dyspnoea scale, which has a strong relationship with mortality. 19 The MMRC assesses dyspnoea as part of the BODE (body mass index, airway obstruction, dyspnoea, exercise capacity) index. 20
Psychological status
Anxiety and depression were measured using the Hospital Anxiety and Depression (HAD) scale. 21
Sample size
A total of 56 participants were required to ensure that 50 participants completed the study allowing for 10% loss to follow-up. Fifty participants were sufficient to provide 80% power to detect as significant, at the 5% level, a minimum 1000 steps difference in average steps/day from hospitalization to first week at home and from first week at home to 6 weeks following hospital admission. This assumes a standard deviation (SD) of 2500 steps in average steps/day, which has been reported previously. 7
Statistical analysis
Data were analysed using SPSS software (version 20 for Windows, SPSS Inc, Chicago, Illinois, USA). The value of p ≤ 0.05 was considered significant. For the outcomes of physical activity, 3 days of data were chosen at each of T1, T2 and T3 (i.e. 9 data points were included in total in the analysis). In order to reduce variability in the measurement of activity, SWA worn for 3 days of the week during T1 were matched to the same 3 days of the week during the 7-day wear time of T2 and T3. For the primary outcome of physical activity, a repeated measures analysis of variance (ANOVA) was conducted across T1, T2 and T3. For any significant differences determined across these time points, a paired means comparison was conducted to determine the change in scores and the 95% confidence interval (CI; e.g. T1 to T2, T1 to T3 and T2 to T3). The pattern of activity within T1 only was also examined using a repeated measures ANOVA. For any significant differences determined across these days, a paired means comparison was conducted to determine the change in scores and the 95% CI (e.g. day 2 to day 3 and day 3 to day 4).
The secondary outcome of FEV1 and FVC was measured at T1, day of discharge and T3 and was analysed with repeated measures ANOVA. For the secondary outcomes of functional exercise capacity, physical performance, health performance, dyspnoea and psychological status measured on the day of discharge from hospital and at T3, analysis was conducted using a t-test for dependent groups.
Results
One hundred and sixty-eight people with an AECOPD were screened as eligible to enter the study, and 59 gave consent to participate. The mean (SD) and median (interquartile range) length of stay was 4.4 (0.7) and 4 (3–7) days, respectively. Participant flow and reasons for exclusion are shown in Figure 1. Nine participants dropped out of the study, either due to skin irritation from the SWA (n = 4) or removal of the SWA prior to the end of the data collection period so that less than 3 days or less than 20.5 hours/day of data were available for analysis (n = 5). A total of 50 participants completed all three time points with adequate compliance of wear time (i.e. T1 average wear time = 98% of 24 hours, T2 average wear time = 97% of 24 hours and T3 average wear time = 97% of 24 hours).
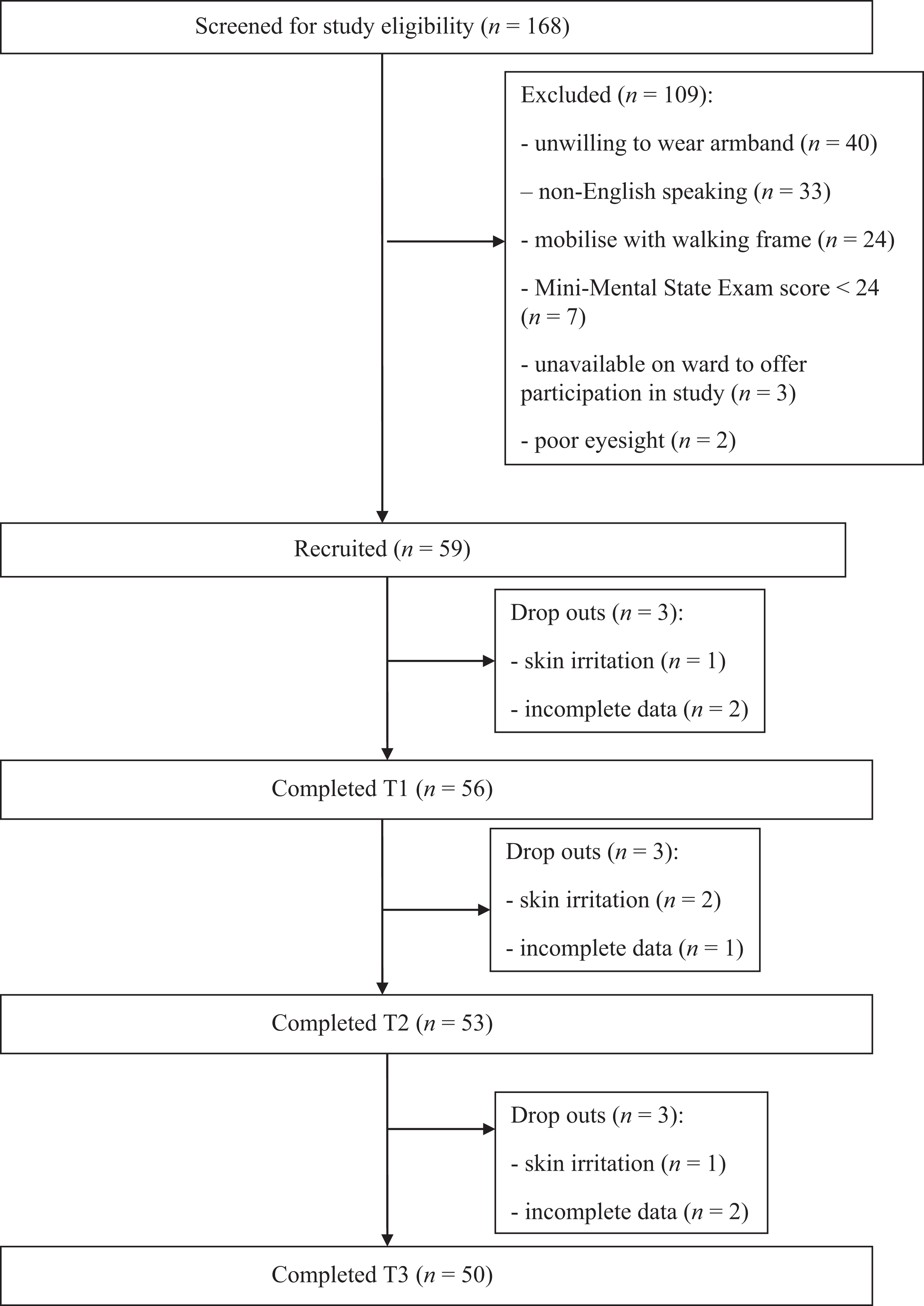
Participant flow chart. n: number; T1: hospitalization period; T2: first week at home following hospital discharge; T3: 6 weeks post hospital admission.
Participant characteristics
The characteristics of the participants who completed all three time points (n = 50) are shown in Table 1. The average lung function in 43 of 50 participants (86%) during the hospital admission was in the severe category, classified as GOLD stages III and IV.
Characteristics of study participants at hospital admission (n = 50).a

BMI: body mass index; LTOT: long-term oxygen therapy; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; GOLD: Global Initiative for Obstructive Lung Disease.
aData are presented as mean (SD) unless otherwise indicated.
Physical activity
There was a significant linear increase in steps, active energy expenditure and time per day spent in moderate activity (3.0–6.0 METs) across the three time points (Table 2). For each of these outcomes, a significant improvement occurred from T1 to T2 and from T1 to T3, whilst the increases from T2 to T3 were not statistically significant (Table 3). The results for physical activity during T1 are presented in Table 4. There was no significant improvement in any physical activity outcomes across days 2, 3 and 4 of the hospitalization period.
Physical activity levels during T1, T2 and T3.a
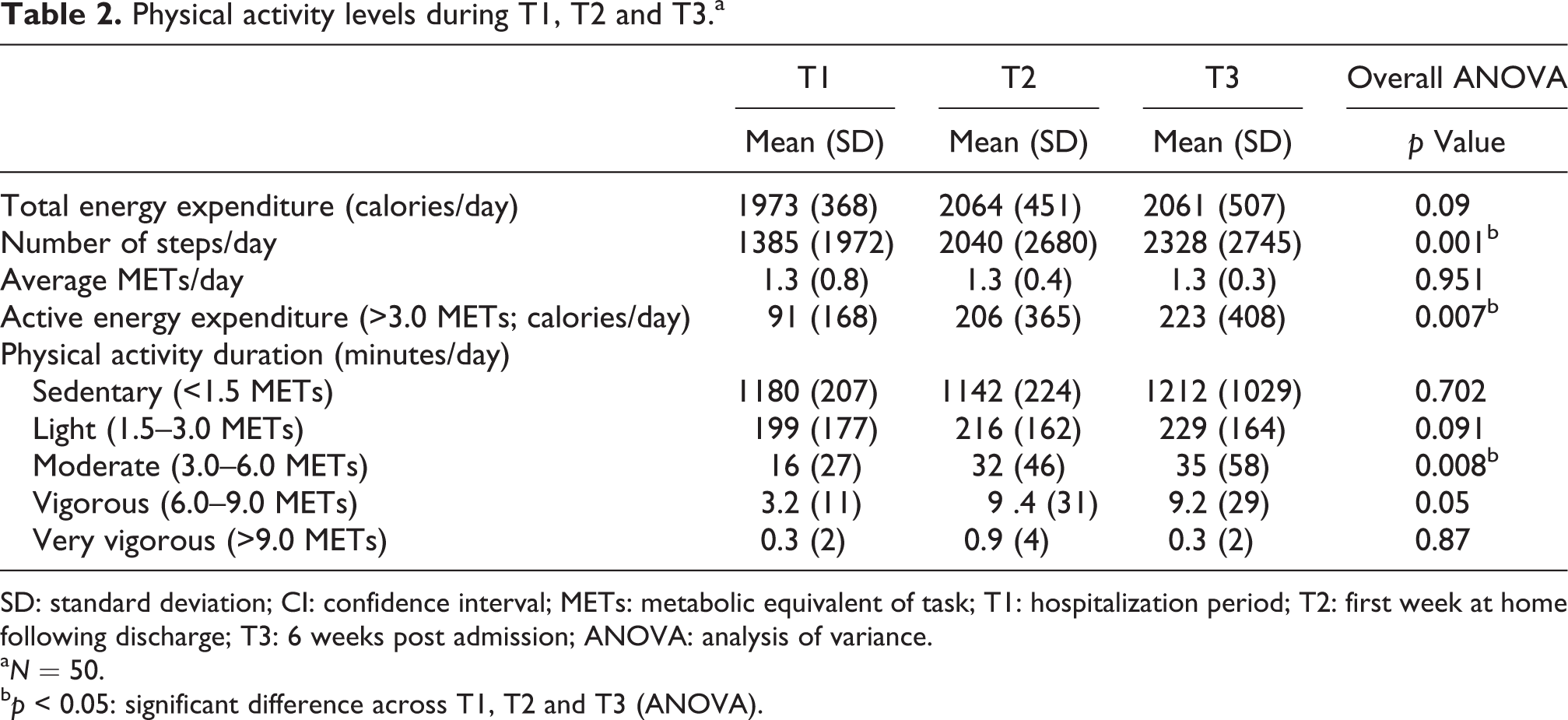
SD: standard deviation; CI: confidence interval; METs: metabolic equivalent of task; T1: hospitalization period; T2: first week at home following discharge; T3: 6 weeks post admission; ANOVA: analysis of variance.
aN = 50.
bp < 0.05: significant difference across T1, T2 and T3 (ANOVA).
Differences in physical activity from T1, T2 and T3.a

CI: confidence interval; METs: metabolic equivalent of task; T1: hospital admission period; T2: first week at home following discharge; T3: 6 weeks post admission.
aN = 50.
bp < 0.05: significant difference.
Physical activity during day 2, day 3 and day 4 of the hospital admission (T1).a

SD: standard deviation; CI: confidence interval; METs: metabolic equivalent of task; T1: hospital admission period; ANOVA: analysis of variance.
aN = 56.
Pulmonary function tests
There was a significant increase in FEV1 and FEV1 (% predicted) from day 2 of hospitalization to day of discharge but no further improvement in lung function at T3 (Table 5).
Change in pulmonary function from day two of the hospitalization period, day of discharge and six weeks following hospital admission (T3).a
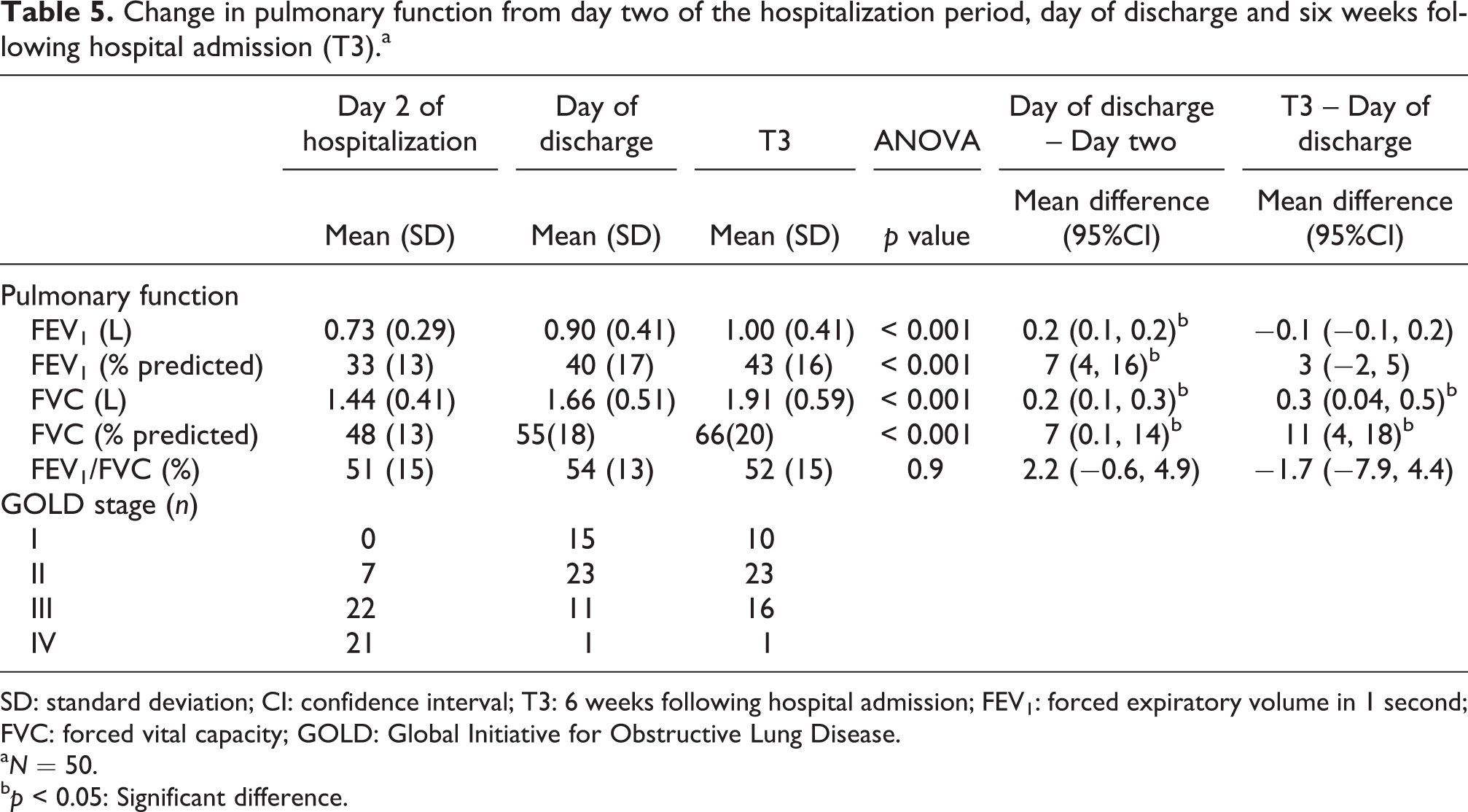
SD: standard deviation; CI: confidence interval; T3: 6 weeks following hospital admission; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; GOLD: Global Initiative for Obstructive Lung Disease.
aN = 50.
bp < 0.05: Significant difference.
Exercise capacity
The 6-minute walk distance at day of discharge was 178 (126) metres (mean (SD)) or 30 (21) % predicted. The 6-minute walk distance improved 70 metres (39%) from day of discharge to T3 (p < 0.05; Table 6).
Secondary outcome measures difference from day of discharge to T3.a

CI: confidence interval; MMRC: Modified Medical Research Council; BODE: body mass index, airflow obstruction, dyspnoea and exercise capacity index; 6MWT: 6-minute walk test; FPI-SF: Functional Performance Inventory–Short Form; CAT: COPD assessment test; COPD: chronic obstructive pulmonary disease; HAD: Hospital Anxiety and Depression scale; N/A: not applicable.
aData are presented as mean (SD) unless otherwise indicated.
bLower score in MMRC dyspnoea scale, BODE index, CAT and HAD equates to better outcome.
cp < 0.05: Significant difference.
dHigher score in FPI-SF equates to better outcome.
Physical performance, health performance, symptom status, psychological status
FPI-SF, CAT, MMRC and the HAD scale did not show a significant change from day of discharge to T3. However, the BODE index was reduced by one unit (16%) from day of discharge to T3 as a consequence of the improvement in lung function and 6-minute walk distance (p = 0.001; Table 6).
D iscussion
This is the first study to comprehensively examine physical activity levels in people hospitalized with an AECOPD as well as to examine the time course of improvement in physical activity levels over 6 weeks following hospital admission. The study showed that physical activity levels were low in hospital with no change to activity levels during an admission, but physical activity did significantly improve during the first week after discharge home and showed no further significant improvement at 6 weeks.
There have been very few studies examining physical activity levels objectively during and following an AECOPD. 4,5 This study has shown that physical activity levels were low in hospital but improved over 6 weeks with an increase in steps of 944 steps/day, active energy expenditure of 132 calories/day and time spent in moderate level activity of 19 minutes/day. For all of these outcomes, the majority of the improvement occurred in the first week at home with further improvements in physical activity 6 weeks later being small and non-significant. The two studies that have previously examined physical activity levels following an AECOPD concur with our results showing that physical activity levels are low in hospital and improve 1 month following discharge. 4,5 However, these studies did not examine the changes immediately following hospital discharge, so our study has clarified the timing of when these improvements occur. It is interesting that the levels of physical activity improved quickly following hospital admission and did not appear to continue to improve significantly over time as the individual’s disease state became more stable. This result is concordant with the finding that pulmonary function did not improve between discharge and 6 weeks post admission. These results suggest that an intervention promoting physical activity for this group may be required in the period up to 6 weeks following hospital admission to improve activity levels with the aim of preventing readmission to hospital, given these outcomes have been shown to be related. 22
Previous studies examining physical activity in the hospital period in people with an AECOPD have only measured activity on 1 or 2 days over a 12-hour period. 4,5 The current study examined physical activity more comprehensively by measuring activity in hospital 24 hours a day over a period of three consecutive days. There was no significant improvement in physical activity levels across these days, despite the significant improvement in lung function. This result agrees with the study by Pitta et al, 4 where no significant improvement was shown in physical activity from day 2 to day 7 in people hospitalized with an AECOPD. Not surprisingly, previous studies indicated a very low level of baseline activity in hospital. A group of Brazilian COPD participants admitted with an AECOPD only walked 602 steps/day in hospital, 5 which was approximately half of the 1385 steps/day recorded in the current study over the same period. However, these findings are not comparable, given the different measurement periods used in the studies (i.e. 24 hours vs. 12 hours). These results suggest that more attention could be given to attempts to increase the physical activity of COPD patients during their admission.
The average length of stay in hospital in our cohort was 4.4 days. This was considerably shorter than the length of stay of the other studies reporting physical activity in people with an AECOPD of 8 to 9 days. 4,5 At 8 days post admission, participants in our study were having their activity measured at home. The increased level of physical activity at home by our participants compared to the low level of physical activity by participants in hospital across the studies, 4,5 including at day 7 in the study by Pitta et al, 4 provides encouraging evidence that early discharge home may help to promote greater activity in the home environment.
The level of physical activity at 6 weeks following admission for an AECOPD was low compared to the reported levels of activity in people with stable COPD of a similar GOLD stage. In the current study, the majority of participants at 6 weeks following an AECOPD were at GOLD stage II–III and at this time were walking an average of 2328 steps/day and spending 35 minutes/day engaged in moderate level activity, which is considerably less activity when compared to a larger study showing participants with stable COPD at GOLD stage II–III walking 5000–7000 steps/day and spending 100–150 minutes/day in moderate level activity. 7 It is interesting that the subjective measure of physical activity – FPI-SF – also showed no change in the total score across the study period when given these low levels of objectively measured activity. The fact that physical activity levels remain low following an AECOPD is an important health issue. A recent large study examining physical activity levels over time in COPD 6 has indicated that a decline to low levels of physical activity over time is associated with increased mortality risk.
Functional exercise capacity is another measure that remained low following the AECOPD as compared to stable COPD. In the current study, the mean 6-minute walk distance was 250 metres at 6 weeks following hospital admission compared to 400–460 metres in a study of stable COPD at GOLD stage II–III. 7 The low level of functional exercise capacity in people following an AECOPD found in this study supports the need for exercise programmes in hospital and following hospitalization to minimize the decline in functional exercise capacity and prevent hospital readmission. Whilst a Cochrane review on exercise training early after hospital discharge 23 has been shown to be effective in improving exercise capacity, to date, no studies have investigated the effects of these programmes on physical activity levels.
There are a number of limitations to this study. The inability of the SWA to reliably detect steps in people using walking aids meant that such patients (n = 22) were excluded, and this reduces the generalizability of our findings. A further limitation was that the 6MWT was only performed once on the day of discharge, as most of the participants did not feel they were able to complete a second test. This suggests that at this time, a second 6MWT may not have resulted in increased walk distance. However, the participants’ true functional exercise capacity at hospital discharge may have been underestimated. One final limitation relates to measuring physical activity levels in the hospital environment. This environment may have artificially reduced a participant’s activity level, given the amount of assistance that is provided, and as such the change in activity following discharge may represent a slight overestimation.
In conclusion, this study has shown that physical activity was low in people admitted to hospital with an AECOPD, did not improve during the hospitalization period but significantly improved during the first week after discharge home and showed no further significant improvement at 6 weeks. Future studies need to address the effectiveness of early rehabilitation programmes on physical activity during and following an AECOPD.
Footnotes
Acknowledgements
The authors thank Dr Roger Adams at the University of Sydney for statistical support And Dr Renae McNamara from the Department of Respiratory Medicine and Sleep and Department of Physiotherapy at the Prince of Wales Hospital, Australia. The authors also acknowledge support provided by all staff members from the Respiratory Coordinated Care Program and Respiratory Medicine ward at the Prince of Wales Hospital, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.