
Abstract
Keywords
Introduction
Pulmonary rehabilitation (PR) is an interprofessional, personalized intervention based on a detailed patient assessment. 1 PR includes, but is not limited to, exercise training, patient education and behaviour change, aiming to enhance the physical and psychological well-being of people with chronic respiratory diseases and to support sustained adherence to health-promoting behaviors. 1 Patient education aims to support people to optimally cope with their disease, to adopt and maintain several health behaviours and to adhere to the recommendations for these health behaviors. 1 Although patient education is recommended by multiple guidelines,1–3 the optimal design of education as part of PR remains unknown.
Chronic obstructive pulmonary disease (COPD) and asthma are the most prevalent chronic respiratory diseases and account for a large proportion of the disease burden associated with chronic respiratory diseases. 4 Moreover, the vast majority of patients referred to PR have COPD or asthma. However, COPD and asthma are complex conditions with varying phenotypic appearances, 5 most probably resulting in people with different educational needs. For example, they may have low health literacy, poor reading skills and/or mild cognitive impairment.6,7 Moreover, information needs can also differ between people with a chronic respiratory disease.8–10 All underline the importance to develop personalized education for these people during PR. Indeed, international experts in the fields of PR and education stated in a recent report 11 : “Effective educational design in PR requires a better understanding of the learners and their needs, and the factors that may influence their learning processes.”
Significant others, like close relatives, have an important role in the disease management of many people with a chronic respiratory disease. 12 Due to their involvement, they need to be well-informed and prepared to assist in disease management. 13 Therefore, involving significant others in educational interventions is important, as this can have a positive effect on the psychological health of significant others and the management of the disease for both patients and significant others.14,15 Nevertheless, educational interventions during PR are also not specifically developed to the educational needs of significant others. 16
Learners’ information needs, learning styles and personality seem to, at least partly, determine the design of educational interventions.17–21 An information need arises when a person wants to expand or update their knowledge. 17
A multimodal learning styles educational approach increases knowledge and understanding in patients.18,22 However, current educational interventions in PR often consist of universal didactic learning with limited participant interaction. 23 Therefore, identifying the learning styles within a specific population may be essential to target and include multiple learning styles in developing patient education. 24 Learning styles are the ways people think, feel, and behave that shape how they understand, interact with, and react to their learning environment. 25
Finally, tailoring messages to someone’s psychological profile increases the impact of the message. 19 Indeed, previous studies showed that personality is associated with adherence to medication 20 and treatment compliance. 21 Personality refers to patterns of thought, emotion, and behaviour that characterize an individual, along with psychological mechanisms that drive these patterns. 26 Yet, information needs, learning styles and psychological profiles have not been studied in people with COPD or asthma entering PR or in their significant others before.
This study aims to identify (a) information needs, (b) learning styles, and (c) psychological profiles of people with COPD or asthma referred for PR and their significant others.
Methods
Study design
This observational study was performed with a cross-sectional quantitative research design. Data was collected between October 2022 and March 2023 at a tertiary care centre for people with chronic respiratory diseases. Based on a 2.5-day pre-PR assessment, patients were allocated to either an outpatient or inpatient PR program. This study received ethical approval.
Population and eligibility criteria
Using consecutive sampling, people referred for PR and eligible for this study, along with one of their significant others, were approached during the pre-PR assessment. If the significant other of an eligible patient was not present, the patient was provided with a package to deliver to their significant other. This package contained a participant information letter, consent form, questionnaire and return envelope. Inclusion criteria were diagnosis of COPD or asthma (spirometry confirmed) or being a significant other of a participating patient, aged 18 years or older and being able to complete a written or verbal questionnaire. Significant other was defined as “a person who spent most time with the patient and/or provided most of the care, assistance and support.” 27 People were excluded if they were unable to understand Dutch.
Data collection
Information needs, learning styles and psychological profiles were assessed with a paper questionnaire. Participants signed an informed consent form and completed the questionnaires during their pre-PR assessment or at home. Participating patients received an informed consent form and a questionnaire for their significant other, if available, which was returned by post mail. For participants who could not read or write, the opportunity for an in person or telephone interview was offered. Additional questionnaires as part of clinical routine were digitally assessed and collected through the electronic patient file. For people with asthma and for significant others, some of the additional questionnaires were added to the paper questionnaire due to a difference in clinical routine.
Outcome measures
Information needs in patients and significant others were assessed by the Lung Information Needs Questionnaire (LINQ). The LINQ is a validated questionnaire to identify information needs of people with a pulmonary disease. 28 It measures information needs on the following domains: the disease, medications, self-management, exercise, diet and smoking. 28 The total score and the score for each domain is provided. Higher numbers indicate a greater need for information.
Learning styles in patients and significant others were assessed with one multiple choice question, according to the learning style categorization of the model of Fleming and Mills. 29 Previous research showed that assessing learning style with multiple choice options is a commonly used method within patient populations. 30 Therefore, learning style was assessed by asking participants to indicate their preferred learning method: visual, aural, reading/writing or kinaesthetic - with the option to select multiple preferences.
Psychological profiles in patients and significant others were assessed by an instrument, developed by a medical technology company, using four psychological profiles: fighter, analyst, optimist and sensitive. 31 Psychological profiles identify how to effectively tailor the style of health information to appeal to the profile’s motivational drivers and information processing preferences by means of verbal and visual design of educational materials (supplemental material 1). 31 Psychological profile was determined by one question asking to circle one out of four statements that describes the participant the best (supplemental material 2).
The following additional characteristics were assessed during the pre-PR assessment as part of routine clinical care or assessed through the paper questionnaire: a. For patients and significant others: Age, sex, educational level, smoking status, medical history, cognitive functioning (Cognitive Failure Questionnaire (CFQ)) with a cut-off >41.6 points for patients and a cut-off >37.8 points for significant others considered as high cognitive failure (mean score plus one standard deviation)
32
and health literacy (Dutch Health Literacy Survey-Europe Q16 (HLS-EU-Q16)) with a cut-off ≤12 points considered as low health literacy.
33
b. For patients: diagnosis, living situation, body mass index (BMI, weight in kg/height in m2), long-term oxygen therapy (LTOT, yes/no) use, rollator use (yes/no), current medication, number of exacerbations within the previous year, number of hospital admissions within the previous year, symptoms of anxiety and depression (Hospital Anxiety and Depression Scale (HADS)) with a cut-off ≥8 points considered as possible or suspected depression or anxiety disorder,
34
symptoms of fatigue (Subjective Fatigue subscale of the Checklist Individual Strength (CIS))
35
with a cut-off ≥36 points considered as severe fatigue,
36
functional exercise capacity (six-minute walk distance (6-MWD)),
37
breathlessness severity (modified Medical Research Council (mMRC))
38
with a cutoff ≥2 grade considered as high breathlessness,
39
post-bronchodilator spirometry (forced vital capacity (FVC), FVC% predicted, forced expiratory volume in the first second (FEV1), FEV1% predicted, and FEV1/FVC)
40
and care dependency (Care Dependency Scale (CDS)) with a cutoff ≤68 points considered as care dependent.
41
c. For people with COPD: health status (COPD Assessment Test (CAT))
42
with a cut-off ≥10 points considered as highly symptomatic.
39
d. For people with asthma: health status (Asthma Control Test (ACT)
43
with a cutoff ≤19 points considered as poorly controlled
44
and Asthma Control Questionnaire (ACQ))
45
with a cutoff ≥1.5 points considered as poorly controlled asthma.
44
e. For significant others: relationship with the patient.
Data analysis
Data was analysed using ‘Statistical Package for the Social Sciences’ (SPSS), version 28. Data were described using mean with standard deviation (SD), median with interquartile range (IQR) or number with percentages, as appropriate. Group comparisons were done using the Pearson’s Chi-square Test, Independent-Samples t test or Mann-Whitney U test, as appropriate. Alpha level of 0.05 was used for statistical significance. Questionnaires were only included for analyses if they were complete.
Results
Participants
In total, 173 patients were screened for eligibility and 148 patients and 137 significant others were asked to participate (Figure 1). 121 patients (57% female; age: 65 ± 10 years; 81% COPD; response rate: 82%) and 67 significant others (55% female; age: 61 ± 12 years; response rate: 49%) were included for analyses. Most participants (43% of patients, and 54% of significant others) had a medium educational level. The score of the cognitive failure questionnaire of 14% of patients and 8% of significant others reflected high cognitive failure. Moreover, 22% of patients and 27% of significant others had low health literacy. Participant characteristics are summarized in Table 1. Flowchart of participants inclusion. Characteristics of patients and significant others. Note. Data are shown as mean ± SD or n (%). Significant differences (=p < .05) are depicted in bold. Abbreviations. 6MWD: 6-min walking distance; ACQ: asthma control questionnaire.; ACT: asthma control test; BMI: body mass index; CAT: COPD assessment test; CDS: care dependency scale; CFQ: cognitive failure questionnaire; CIS: checklist individual strength; FEV: forced expiratory volume; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; LTOT: long-term oxygen therapy; mMRC: modified medical research council; n/a: not applicable; SD: standard deviation. a=patients: n = 120. b=significant others: n = 66. c=patients: n = 118. d=patients: n = 98; significant others: n = 64. e=patients: n = 118; significant others: n = 65. f=patients: n = 115. g=patients: n = 114. h=patients: n = 113. i=patients with COPD: n = 96. j=patients with asthma: n = 21.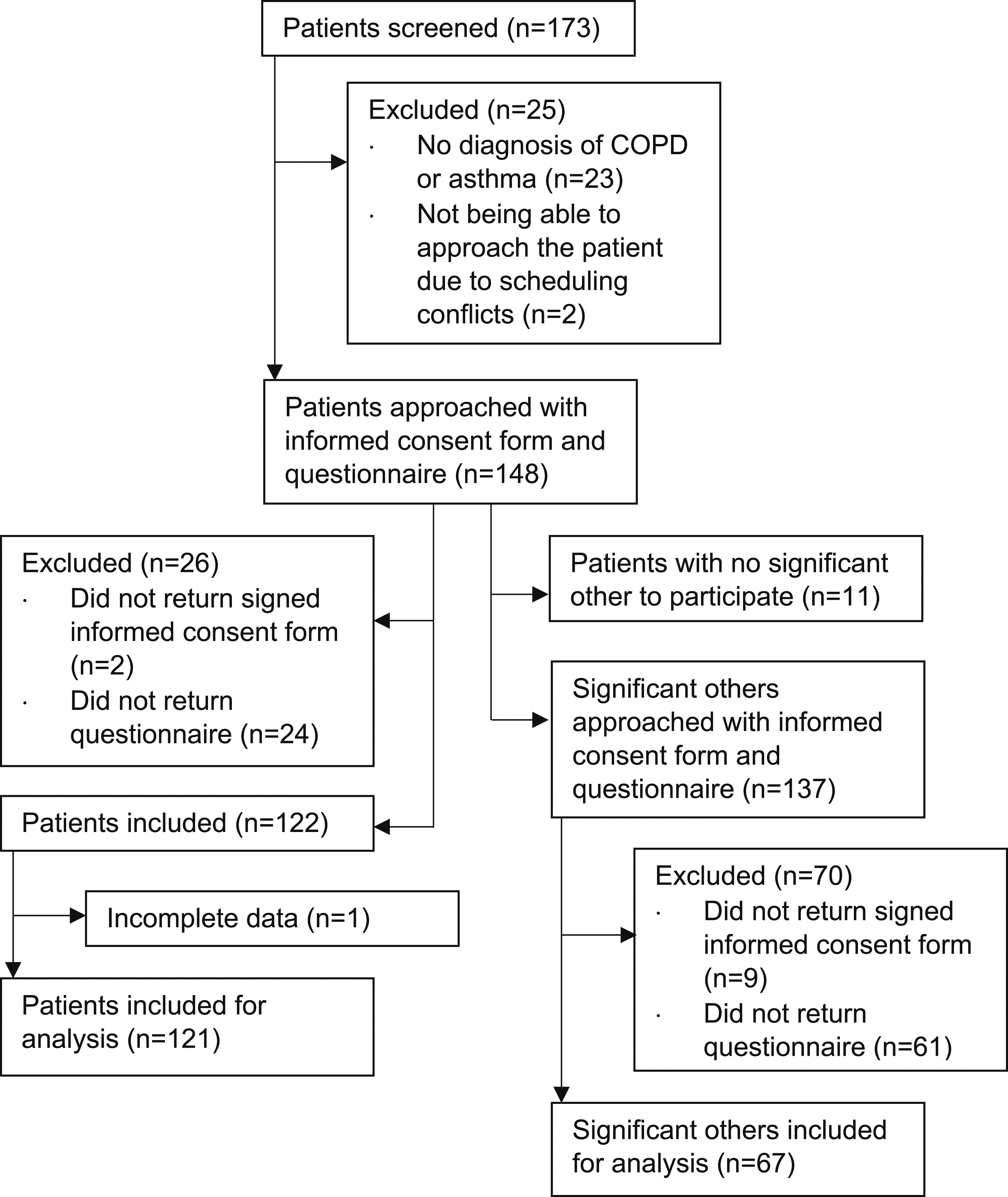

Information needs, learning styles and psychological profiles
Information needs, learning styles and psychological profiles of patients and significant others.
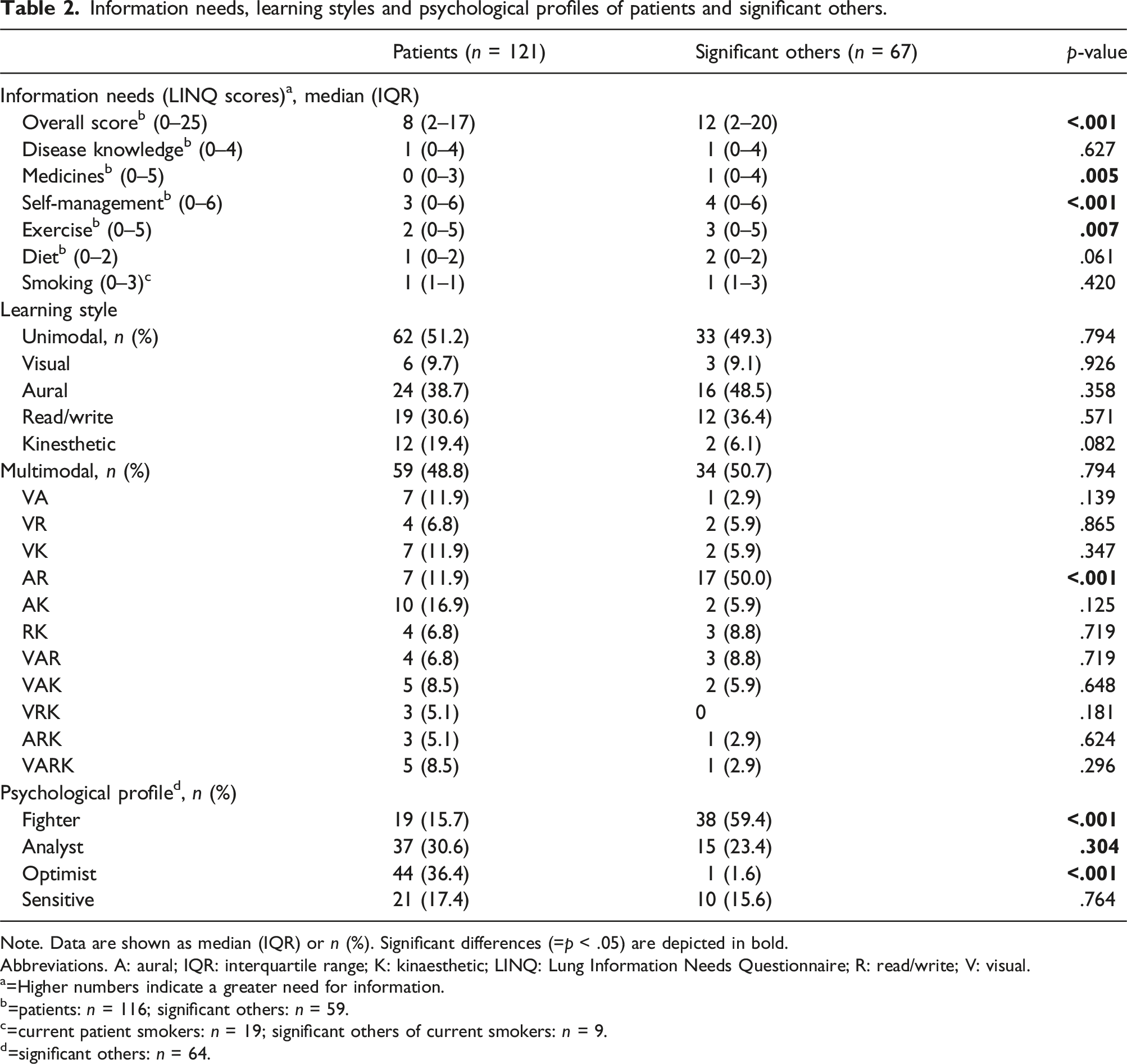
Note. Data are shown as median (IQR) or n (%). Significant differences (=p < .05) are depicted in bold.
Abbreviations. A: aural; IQR: interquartile range; K: kinaesthetic; LINQ: Lung Information Needs Questionnaire; R: read/write; V: visual.
a=Higher numbers indicate a greater need for information.
b=patients: n = 116; significant others: n = 59.
c=current patient smokers: n = 19; significant others of current smokers: n = 9.
d=significant others: n = 64.
Patients as well as their significant others mostly preferred the aural (39% and 49%, respectively) and read/write learning styles (31% and 36%, respectively) as unimodal learners. 49% of patients and 51% of significant others preferred more than one learning style. The most preferred multimodal learning style was a combination of aural and kinaesthetic (17%) in patients and a combination of aural and read/write (50%) in significant others. Within multimodal learners, the visual (59% and 32%), aural (69% and 79%), read/write (51% and 79%) and kinaesthetic (63% and 32%) learning styles are all prevalent in patient and their significant others, respectively (Table 2).
Most prevalent psychological profiles were optimist in patients (36%) and fighter in significant others (59%) which were significantly different compared to patients (p < .001) (Table 2).
Information needs, learning styles and psychological profiles were generally comparable between people with COPD and asthma (supplemental material 3). Additionally, information needs, learning styles and psychological profiles of only the patients of which their significant other participated and their accompanying significant others were identified. These were comparable to the general sample of patients and significant others with similar significant differences between patients and their significant others (supplemental material 4).
A variety of combinations of learning styles with psychological profiles were identified within participants (Figure 2). Moreover, for both low and adequate health literacy levels, a variety of learning styles were identified, with each learning style being present (Figure 3). Prevalence of the combinations of learning styles with psychological profiles. Note. Larger symbols indicate a larger percentage of the prevalence of the combinations of learning styles with psychological profiles. Prevalence of learning style within different health literacy levels.

Discussion
Main findings
This is the first study demonstrating a variety of information needs, learning styles and psychological profiles among people with COPD or asthma entering PR and their significant others. These findings indicate the importance of addressing this diversity of individual needs within PR.
Previous studies highlight the importance of including significant others in patient education.12,14–16 This is justified by our study since the LINQ scores were found to be significantly higher in significant others, indicating their need for education. The greatest information needs were found in the domain self-management, exercise and diet in significant others. Our study is the first using the LINQ to examine information needs of significant others of people with COPD and asthma. In patients, the greatest information needs were found in the domain self-management and diet. Previous research found similar information needs of people with COPD from primary care, rehabilitation, hospital or respiratory patient organizations using the LINQ.8–10,46–48 However, palliative care, social security, fatigue, anxiety, stress and depression were found to be an information need using an additional questionnaire with a holistic approach. 8 Our study did not find these information needs with only using the LINQ. Therefore, information needs should be interpreted with caution, since the LINQ measures knowledge gaps which do not automatically imply that the respondent wants to receive this information. To understand what participants truly need and desire, in-depth insight into the perspectives of the participants is an essential follow up research. Nevertheless, the variety in information needs emphasizes the importance of interprofessional collaboration to develop patient education tailored to individual needs. PR offers this opportunity, as it is an interprofessional intervention based on a comprehensive patient assessment. 1 For example, healthcare professionals with different professional backgrounds can offer education in specific topics. This enables patients and their significant others to receive specific and tailored information from expert healthcare professionals, but also requires and supports interprofessional collaboration in the development and delivery of educational programs during PR.
Our study found that both patients and their significant others mostly preferred the aural and read/write learning style, as well in unimodal learning as in multimodal learning which is in line with a previous study assessing learning styles among people with COPD: the authors found that “in person, talking to someone who knows” (i.e. the aural learning style) was the most preferred learning style. 49 Moreover, written and aural information is preferred by adults in general that receive health education. 30 Nearly half of the participants in our study preferred the multimodal learning style which is comparable to the learning style of other patient populations and significant others. 30 Although some participants have a unimodal learning style, there is a lack of evidence supporting to focus on one primary preferred learning style, as learners generally benefit from multimodal educational approaches.18,22,24,50 Additionally, this study found that all four learning styles were prevalent among both unimodal and multimodal learners, highlighting their essential role in educational interventions. Therefore, it is not essential to tailor to a single preferred learning style. 24 In clinical practice, education should be tailored by incorporating multiple learning styles, allowing learners to engage with more than one method and empowering them to choose their preferred methods. This may increase their sense of autonomy and potentially enhance their motivation to learn. 51 Examples of applying learning styles in education include visually, by means of diagrams, graphics or illustrations, auditory, by means of talking one-on-one, lectures or discussions, reading/writing, by means of books, brochures or manuals, and kinaesthetically, by means of demonstrations, exercises and applications. The systematic review of Stoilkova et al. provides additional examples of educational tools linked to various learning styles which have been identified in educational programmes within COPD management interventions. 52
Psychological profiles of people with COPD or asthma and their significant others have not been investigated before. Our results show that people with COPD or asthma were more often an optimist and their significant others were more often a fighter. Interindividual differences of personality traits in people with COPD referred for PR have been identified earlier. 53 However, our results are not in concordance with a study that investigated solely the personality traits of people with COPD referred for PR. 53 These authors found that most patients (31%) were classified as dominant, 53 which could be comparable to the psychological profile fighter (16%) in our study. Moreover, the fewest patients (16%) were classified as conscientious, 53 while our results show that 31% were analyst. These differences can partly be explained by the fact that our psychological profiles results are based on personality traits and psychological characteristics, 31 while Grosbois et al. only on personality. 53 More than half of significant others reflect the psychological profile fighter. Due to their feeling of responsibility and alertness, 54 significant others might feel more dominant than patients in a caregiving role and might feel the need to be strong for their caring other which relates to the psychological profile fighter. The variation in psychological profiles indicates that different communication strategies should be considered for educational interventions in PR. Future research is needed to explore the positive impact of tailoring education to the specific psychological profiles of learners. 31 For example, the fighter may receive a positive to-the-point message, the analyst factual elaborate information, the optimist a non-threatening personal story and the sensitive an empathic message from an authority.
Moreover, our study shows that the combinations of learning styles and psychological profiles are heterogenous. This indicates that both learning styles and psychological profiles should be considered in education. Even for different health literacy levels the learning styles differ, emphasizing that health literacy should be taken into account for all learning styles in tailored education. Multiple strategies for health communication and information provision are available to target persons with low health literacy and to use for educational interventions. 55 For example, the Patient Educational Materials Assessment Tool (PEMAT) can evaluate the understandability of written and audiovisual materials. 56 Additionally, for both written and verbal education, using an accessible reading level, such as Common European Framework of Reference for Languages (CEFR) level B1, is recommended.57,58 Furthermore, the teach-back method, in which patients or their significant others summarize their understanding, can be effective for improving comprehension in verbal education. 59
Strengths and limitations
Since the information letter and questionnaires of interest could be read aloud if needed, four illiterate persons or persons with low reading ability were able to participate. Therefore, the impact of poor literacy and reading ability was reduced and could be considered a strength of this study. However, low health literacy, which is often associated with low levels of education, 60 may still have been a barrier to participation. Given that the prevalence of patients with low education levels in our study is slightly lower than in a comparable sample, 61 health literacy may still be a source of bias by underrepresenting people with low health literacy levels in our study.
Moreover, multiple methods to assess learning styles in adults receiving health education exist. 30 We have chosen one multiple choice question. Others have used the Visual-Aural-Read/write-Kinaesthetic (VARK) questionnaire in adults receiving health education. 30 The VARK is a 16-item validated questionnaire that requires reading comprehension. Therefore, our study used one multiple choice question to assess learning style, since our population of interest faces several challenges that may limit their understanding of the VARK questionnaire. Furthermore the multiple choice question has shown to have close alignment with the VARK questionnaire. 30
As educational interventions are a core part of PR, 1 it was very reasonable to recruit patients at the start of a PR program. Obviously, this may limit the generalizability of the current findings to people with COPD or asthma in other care settings. Another limitation concerns the unequal proportion of patients and significant others, and the unequal proportion of people with COPD and asthma. However, participation of significant others was high compared to a study conducted in similar circumstances. 6 Nevertheless, our results show no differences between our general sample and a sample with an equal proportion of patients with their accompanying significant other. Lastly, the instrument used to assess psychological profiles has been validated in patients, not in significant others.
Conclusions
This study identified a variety of information needs, learning styles and psychological profiles among people with COPD or asthma and their significant others, which indicates the need to develop and deliver tailored education within PR. Tailoring education requires a different approach to education than universal didactic learning. In practice, to address different information needs, an interdisciplinary educational program is essential. Learners should have the opportunity to choose among a variety of topics from different specialties and have access to multiple learning styles that align with their individual needs and preferences. Furthermore, educational interventions should consider to incorporate different communication strategies. Since PR provides this opportunity, it is possible to offer education to patients and their significant others based on their psychological profile which can be assessed during their pre-PR assessment. Moreover, PR can offer interdisciplinary topics to choose from and it provides the opportunity for multiple learning styles, for example practical learning through exercise training which benefits the kinaesthetic learning style.
Supplemental Material
Supplemental Material - Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study
Supplemental Material for Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study by Anouk JL Muijsenberg, Sarah Houben-Wilke, Jan Tatousek, Joyca Lacroix, Martijn A Spruit and Daisy JA Janssen in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study
Supplemental Material for Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study by Anouk JL Muijsenberg, Sarah Houben-Wilke, Jan Tatousek, Joyca Lacroix, Martijn A Spruit and Daisy JA Janssen in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study
Supplemental Material for Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study by Anouk JL Muijsenberg, Sarah Houben-Wilke, Jan Tatousek, Joyca Lacroix, Martijn A Spruit and Daisy JA Janssen in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study
Supplemental Material for Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: A cross-sectional study by Anouk JL Muijsenberg, Sarah Houben-Wilke, Jan Tatousek, Joyca Lacroix, Martijn A Spruit and Daisy JA Janssen in Journal of Chronic Respiratory Disease.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AJLM and SHW declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. JT and JL are both salaried employees of Philips with no conflict of interest. MAS reports grants and/or fees from Netherlands Lung Foundation Netherlands, Stichting Astma Bestrijding, Boehringer Ingelheim, AstraZeneca, Chiesi, GSK and TEVA, all paid to the institution and all outside the submitted work. DJAJ has received lectures fees from Boehringer Ingelheim, and non-personal lecture fees from Chiesi, AstraZeneca and Abbott within the previous 3 years, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.