
Abstract
Keywords
Introduction
Primary ciliary dyskinesia (PCD) is a rare genetic disease, inherited mainly as autosomal recessive with a prevalence of about 1 in 7554. 1 It is characterized by abnormal structure and/or function of the cilia. Cilia are tiny hair-like structures that protrude from the surface of cells. They play a role in mucociliary clearance and transport of fluid. Common clinical features of PCD include chronic nasal congestion, chronic otitis media, recurrent chest infections, daily productive cough, bronchiectasis, situs inversus totalis (in about 50% of patients), and male infertility. 2
A multidisciplinary team approach and early diagnosis are essential for preventing the progression of lung disease. A key component of the treatment plan is regular airway clearance, which includes physical activity and chest physical therapy. 3
The active cycle of breathing technique (ACBT) is a form of airway clearance commonly used in respiratory diseases. It can be used to mobilize and clear excess pulmonary secretions; this may help prevent chronic airway infection and associated inflammation. ACBT consists of three phases: breathing control, thoracic expansion exercise, and forced expiratory technique. 4 One of the advantages of this technique is that it can be used at home under parental guidance when necessary. The technique doesn’t require the use of any specialized equipment, it is both safe and effective. 5
On the other hand, oscillating positive expiratory pressure (OPEP) devices such as the Aerobika® are drug-free, handheld, and easy to use. 6 The device reduces air trapping, facilitates sputum clearance from the lungs, and improves lung ventilation. This occurs as a result of the combination of high-frequency oscillations with positive expiratory pressure that are generated during a slightly active expiration through a device. A recent systematic review states that using positive expiratory pressure (PEP) in cystic fibrosis (CF) patients is safe without adverse effects. 7
The evidence for specific ACT in PCD is limited. However, many ACTs used in CF are applicable to PCD due to similar physiological principles involved in mucous clearance. 8
Comparing these techniques is essential, as they both aim to improve mucus clearance and lung function, offering insights for optimizing PCD management in light of the limited evidence surrounding airway clearance methods.
This is the first study addressing airway clearance interventions among PCD patients in Palestine. The purpose of this study was to explore the feasibility of using two different ACTs and to compare their effectiveness in enhancing lung function and functional exercise capacity among children with PCD.
Methods
Study design
In this experimental feasibility study, a simple randomization method was used to assign patients. A random number sequence was generated in Microsoft Excel, with patients receiving even numbers allocated to the ACBT group and those with odd numbers to the OPEP group. Stratification by age groups (6–12 years and 13–18 years) was employed. Outcome measures were conducted by an independent assessor, blinded to the treatment allocation, at baseline, week 6, and week 12. The intervention lasted 12 weeks, from June 2023 to October 2023.
Study population
48 participants (age 6–18 years) with a confirmed PCD diagnosis, were recruited from the pediatric pulmonology clinic at Caritas Baby Hospital (CBH) in Bethlehem. The Palestinian PCD cohort was confirmed through collaboration with Southampton University and University College London, where diagnostic tests, transmission electron microscopy (TEM), and genetic analyses were conducted. 9 32 patients (59.3% males, 40.6% females) fulfilled the inclusion criteria and agreed to participate. Inclusion criteria were: a confirmed PCD diagnosis by hallmark TEM and/or positive genetic testing, resident of the West Bank-Palestine, clinical stability with a predicted FEV1 >30%, capability to perform the prescribed chest physiotherapy home program (either independently or with parental assistance), and parental consent. Exclusion criteria encompassed recent pneumothorax within 1 year of study initiation, significant history of hemoptysis, chest trauma, presence of other chronic or respiratory conditions such as heart disease, asthma, delayed cognitive abilities affecting pulmonary function testing (PFTs), or parental refusal.
Outcome measures
A structured form was designed to collect patient data, including demographics, medical history, medications, sputum results, cough and sputum characteristics, and associated symptoms, along with a weekly calendar to track adherence to the prescribed home program.
Spirometry was conducted according to the American Thoracic Society (ATS) and the European Respiratory Society (ERS) guidelines 10 using Smart PFT LabTM (Medical Equipment Europe GmbH, Hammelburg, Germany). Forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), and maximum expiratory flow between 25% and 75% of FVC (MEF25-75%) z-scores were calculated using ERS Global Lung Index (GLI) reference values. Six-Minute Walk Test (6MWT) was performed following the American Thoracic Society guidelines. 11
Intervention
Before the study, each participant completed a familiarization training session on either ACBT or OPEP, based on their randomization, to ensure the correct technique. Most of the participants (80%) were practicing ACBT before the study as their airway clearance regimen, while the remaining patients used either chest percussion or none. They were instructed to follow only their assigned ACT throughout the study. Additionally, they were asked not to make any changes to all other therapies they were taking like bronchodilators, hypertonic saline (HTS), and prophylactic antibiotics during the study period. Of note, all patient were receiving Albuterol and HTS before their ACT sessions.
As a home-based treatment, the participants were required to complete two sessions daily, in the morning and the evening, before meals. Each session lasted 15 min. Participants were instructed to adhere to the prescribed program and to document their treatments on a weekly calendar. The respiratory therapist (BF) monitored and observed the procedure remotely by contacting the participant twice weekly. Emojis and encouraging statements were sent to participants to keep them motivated to adhere to the given program.
ACBT sessions were performed in a sitting position. Each cycle included 2–3 min of breathing control, 3–4 deep breaths with a 3-s hold, followed by 1–2 low-volume huffs and 1 high-volume huff, then a return to breathing control before repeating another cycle (Figure 1). Illustrating ACBT performance: (A) breathing control, (B) thoracic expansion, (C) huffing.
Aerobika sessions were performed in a seated position (Figure 2), the participant was instructed to inhale slightly larger than the tidal volume through the device’s mouthpiece. Subsequently, the patient was instructed to hold breath for 2–3 s followed by a slight active expiration through the mouthpiece. It is recommended to exhale 3–4 times longer than the inhalation. A typical cycle of OPEP therapy consists of 10–20 breaths through the device followed by the forced expiration technique and then coughing to further mobilize secretions. Illustrating aerobika therapy.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS) version 26 (SPSS Inc., Chicago, IL), was used to conduct the statistical analysis. Descriptive statistics were used to characterize the sample according to age, clinical manifestations, and other variables. ANOVA, Independent sample T-tests, and paired sample tests were performed to compare the mean values of the study variables between and within the groups. Cohen’s d was used to compute the effect size. Statistical significance was set at p-value <.05.
Results
Baseline characteristics.
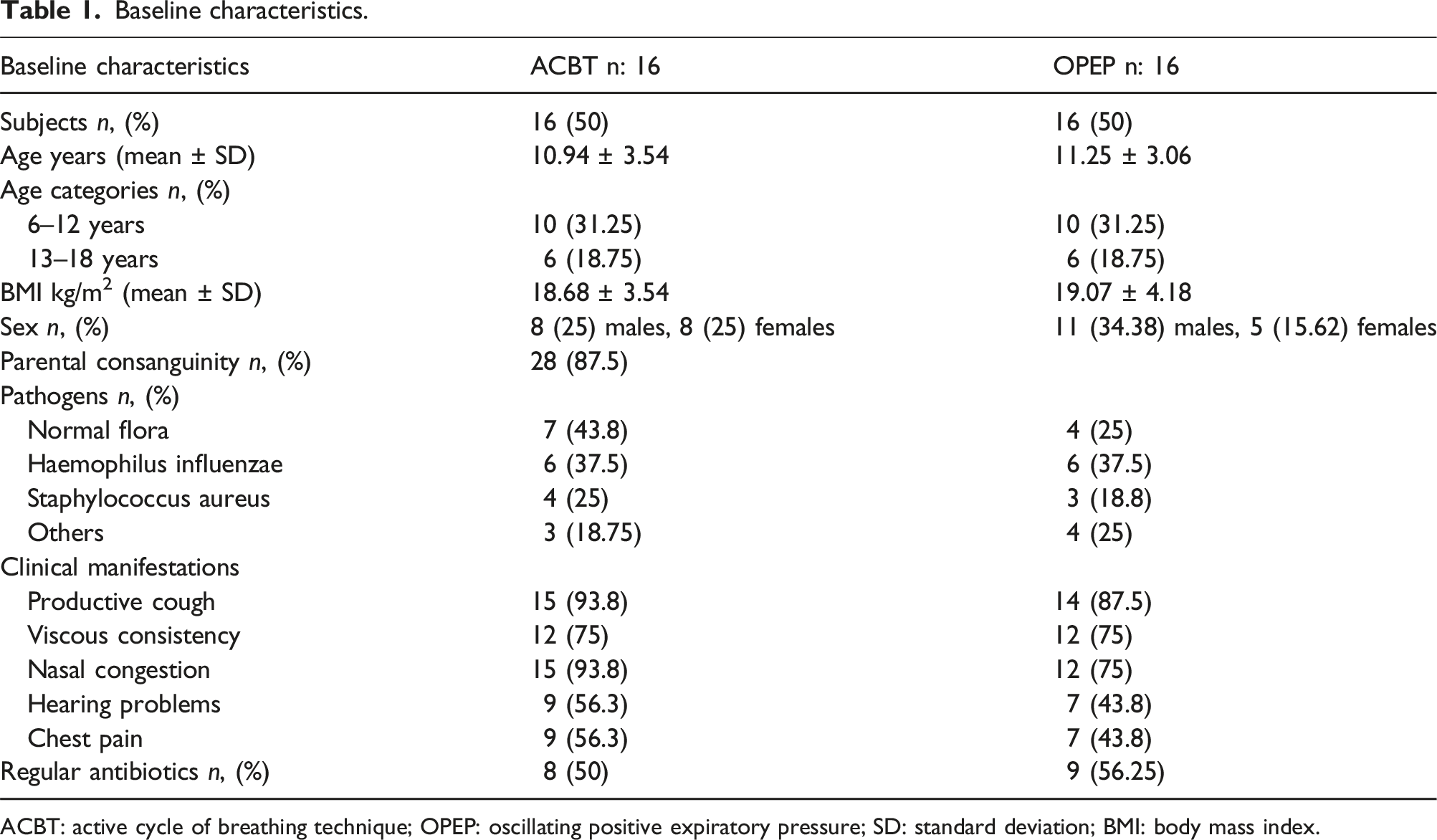
ACBT: active cycle of breathing technique; OPEP: oscillating positive expiratory pressure; SD: standard deviation; BMI: body mass index.
The main clinical manifestations were productive cough (90.6%), with a viscous consistency (75%), nasal congestion (84.4%), hearing problems (50%), and chest pain (50%). Additionally, 40% had situs inversus totalis. Based on the results of sputum cultures obtained during the last 6 months, 34.4% had normal flora. Haemophilus influenzae was the most prevalent respiratory pathogen (37.5%), followed by Staphylococcus aureus (21.9%).
Participant recruitment was successful, with all participants selected from the CBH pulmonology clinic database. 48 were identified for eligibility screening, five did not meet the eligibility criteria, nine families declined to participate, and two were unavailable due to travel (see Supplemental 1). This method allowed for efficient and easy recruitment of the study sample. Self-reported nebulizer adherence was 95.2% for ACBT and 88% for OPEP (p = .064). ACT adherence was 95.6% for ACBT and 87.5% for OPEP (p = .067). All outcome measures and follow-ups were completed effectively.
Children and caregivers were satisfied with the interventions. In the ACBT group, 81.25% found the technique was effective for clearing secretions, while 31.25% indicated a need for parental guidance. In the OPEP group, 93.75% found it easy to use, and 75% reported that it was effective for mobilizing secretions, appreciating its motivating nature and potential for independent use. During the study period, two participants received additional antibiotics; one in the ACBT group for a chest infection and another in the OPEP group for an ear infection.
Comparison between the 2 groups (ACBT and OPEP) at baseline and after the intervention
The mean difference of the study variables between the two groups.
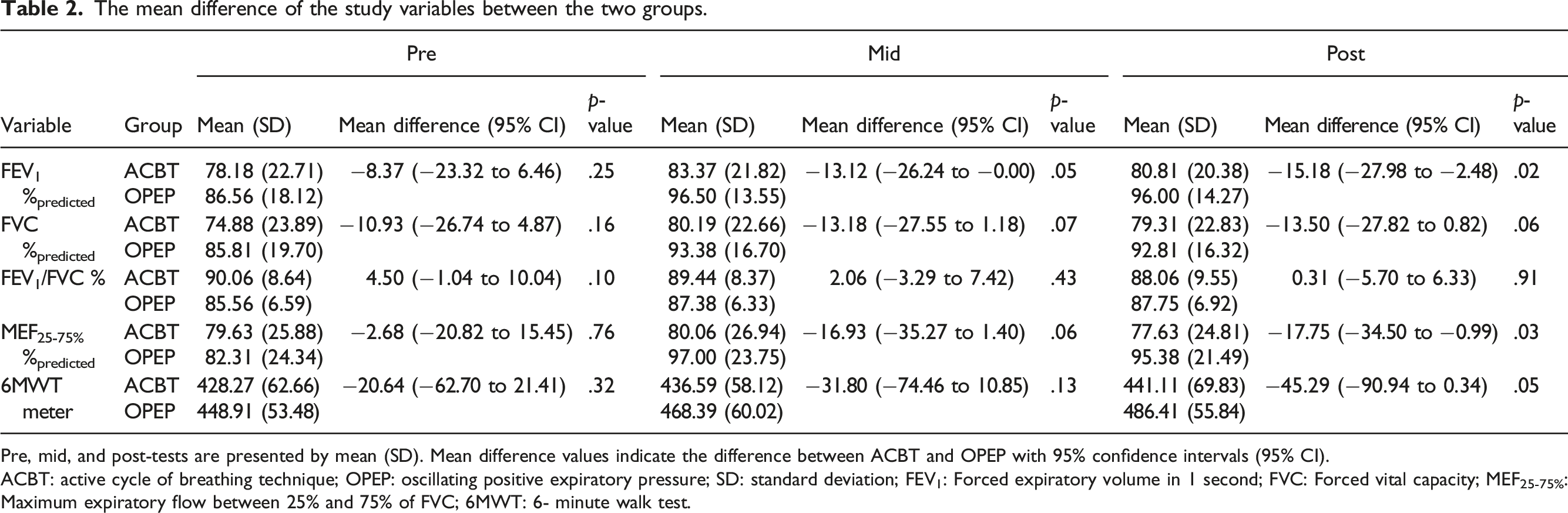
Pre, mid, and post-tests are presented by mean (SD). Mean difference values indicate the difference between ACBT and OPEP with 95% confidence intervals (95% CI).
ACBT: active cycle of breathing technique; OPEP: oscillating positive expiratory pressure; SD: standard deviation; FEV1: Forced expiratory volume in 1 second; FVC: Forced vital capacity; MEF25-75%: Maximum expiratory flow between 25% and 75% of FVC; 6MWT: 6- minute walk test.
After 12 weeks of regular ACT, significant differences were found between the two groups in post-tests for FEV1 (p = .02), MEF25-75% (p = .03), and the 6MWT (p = .05). These findings indicate that OPEP was more effective than ACBT, with effect sizes (Cohen’s d) of 0.86, 0.76, and 0.71 respectively. On the other hand, no statistically significant difference was observed between the two groups in FVC and FEV1/FVC (p > .05).
Comparison within the same group at baseline and after the intervention
The ACBT group showed no statistically significant differences between the pre and post-tests for FEV1 and 6MWT (p > .05). In contrast, the OPEP group showed statistically significant differences between the pre and post-tests for FEV1 (p = .00) and 6MWT (p = .00), as illustrated in Figures 3 and 4. FEV1 percentage between both groups during the intervention (n = 32). FEV1: Forced expiratory volume in 1 s. Box-Whisker plot shows mean (x), median (horizontal line), interquartile range (box), and minimum/maximum (whiskers). The total distance walked in meters in 6 MWT between the two groups in the intervention. Box-Whisker plot shows mean (x), median (horizontal line), interquartile range (box), and minimum/maximum (whiskers).

Discussion
This was the first PCD clinical trial conducted in Palestine, and adds to the limited global data to compare two ACTs for patients with PCD. It was designed to assess the feasibility of implementing these techniques, as well as their effects on lung function and other outcome measures over a 12-week period.
This study demonstrates that both ACBT and OPEP are feasible for use in home settings for children with PCD, with high adherence rates indicating that these techniques are acceptable to both children and their caregivers. The results indicate that ACTs can be effective and manageable options for improving respiratory health in children with PCD. Compared to ACBT, OPEP appears to be more user-friendly and may be preferable, especially for younger children requiring more independent treatment. Its combination of oscillation and positive expiratory pressure helps clear secretions, which is beneficial for children with impaired ciliary function. While OPEP shows potential advantages, treatment should remain individualized. Larger, multicenter trials are needed to confirm these findings and evaluate whether OPEP should be widely recommended.
Using spirometry and the 6MWT is feasible for assessing respiratory function in children aged 6 to 18 years. Combining both methods can enhance understanding of respiratory health. Spirometry offers objective measurements of lung function, 10 but its accuracy can be influenced by the children’s ability to follow instructions and perform maximal efforts. The 6MWT, on the other hand, is a useful measure of functional exercise capacity, 11 though its outcomes can vary due to factors like motivation, fatigue, and external encouragement. To address these challenges, a familiarity session was held prior to the study to help the children understand the procedures and reduce variability in their performance.
This study included 32 participants aged 6 to 18 years recruited from a pediatric pulmonary clinic in Bethlehem, Palestine. A recent study conducted in Palestine identified 68 individuals with a positive diagnosis of PCD confirmed by TEM and/or genetics. 9 Most participants (87.5%) reported a positive history of parental consanguinity, likely due to the cultural practices of consanguineous marriages. 12 A similar high consanguinity was found in a Saudi study (93% of PCD patients), 13 and high PCD prevalence was noted in closed communities like the British Asian population (1 in 2265). 14
There were no significant differences between the groups at baseline that could have impacted outcomes during the treatment period. Sputum cultures showed similar organisms, and the ACTs used before the study were also comparable, minimizing potential influences on the results.
The main clinical manifestations described in our study were similar to those reported in a systematic review by Goutaki et al., 15 and a Swiss study. 16 The most common pathogens found on the sputum cultures of our patient were Haemophilus influenzae followed by Staphylococcus aureus, similar to previously published data by Piatti et al. 17
Spirometer results indicate that significant differences in lung function between the 2 groups after 12 weeks were evident only in FEV1 and MEF25-75% in favor of the OPEP, but not in the other parameters (FVC and FEV1/FVC). In line with our results, a study found that using OPEP compared to mechanical percussion for lower respiratory tract infections improved lung function by increasing oxygenation, reducing inflammation, and improving sputum drainage. 18 This may be explained by the fact that OPEP devices produce a positive expiratory pressure, which reduces airway collapsibility and promotes collateral ventilation, which facilitates the movement of secretions centrally. 19 In a randomized crossover trial to compare ACBT and Flutter in individuals with non-CF bronchiectasis, Üzmezoğlu et al concluded that both interventions had comparable effects on lung function parameters. 20 Moreover, a systematic review studied the impact of OPEP therapy on lung function in adults with non-CF stable bronchiectasis, indicated that OPEP and other ACTs had similar effects. 21 The differences in findings across these studies could be attributed to variations in sample inclusion criteria, characteristics, methodologies, and underlying diseases.
Field walking tests are widely used to assess exercise capacity, which is an important measure of respiratory-related function. At the end of the 12-week intervention, the 6MWT results showed a statistically significant improvement for the OPEP group (p < .05). Findings are consistent with the results of Murray et al. 22 who found that the incremental shuttle walk test distance improved in non-CF bronchiectasis patients who received Acapella twice daily for 3 months. In contrast, a study comparing five different ACT techniques (ACBT, autogenic drainage (AD), PEP, Cornet, and Flutter) found no statistically significant differences in exercise tolerance among CF patients. 23 Variations in patient effort, motivation, adherence, and technique application across studies may have influenced the results of field walking tests.
Study limitations
The study included only stable PCD patients, excluding those with acute exacerbation, and lasted 12 weeks. A longer follow-up is needed to assess long-term effectiveness. Being home-based, non-compliance was a risk. We addressed this with motivational calendars, regular communication, and mid-study follow-ups. Despite these efforts, strict adherence cannot be documented. Additionally, some participants declined to participate due to geographic distance, long commute, and the unstable political situation.
Conclusion
The study supports the feasibility of implementing a randomized comparison of ACBT and OPEP in children with PCD. The outcome measures, including spirometry and the 6MWT, were suitable for assessing respiratory function in this population. The findings suggest that OPEP can play a significant role in managing respiratory health for children with PCD. However, treatment should remain individualized. Further research, including larger, multicenter trials, is necessary to generalize these findings, evaluate the long-term effectiveness of these techniques, and explore their broader applicability in routine care for children with PCD.
Supplemental Material
Supplemental Material - Active cycle of breathing technique versus oscillating positive expiratory pressure therapy: Effect on lung function in children with primary ciliary dyskinesia; A feasibility study
Supplemental Material for Active cycle of breathing technique versus oscillating positive expiratory pressure therapy: Effect on lung function in children with primary ciliary dyskinesia; A feasibility study by Bishara Fashho, Nisreen Rumman, Jane Lucas and Hadeel Halaweh in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Active cycle of breathing technique versus oscillating positive expiratory pressure therapy: Effect on lung function in children with primary ciliary dyskinesia; A feasibility study
Supplemental Material for Active cycle of breathing technique versus oscillating positive expiratory pressure therapy: Effect on lung function in children with primary ciliary dyskinesia; A feasibility study by Bishara Fashho, Nisreen Rumman, Jane Lucas and Hadeel Halaweh in Journal of Chronic Respiratory Disease.
Footnotes
Acknowledgements
The authors thank the patients and their families for their participation. We acknowledge Trudell Medical International for providing the AEROBIKA* OPEP devices. Special thanks to the Physiotherapy Department at Al-Quds University for their support and to Caritas Baby Hospital-Bethlehem for their collaboration. We also appreciate the Caritas Baby Hospital physiotherapy team, led by Asma Siman, and George Iseed for his invaluable role in conducting the study’s outcome. We also thank the respiratory therapists at Southampton Hospital (Amanda-Lea Harris, Victoria Keenan, and Hannah Wilkins) for reviewing the research protocol and for their valuable input.
Author contributions
BF, NR, JL, and HH contributed to the concept and design of the work. BF and NR contributed to the acquisition of data. BF and HH contributed to the analysis and interpretation of data. BF drafted the initial manuscript; NR, JL, and HH revised it critically for important intellectual content. All authors approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.