
Abstract
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disease characterized by irreversible airway obstruction. It affects 16.4 million people, including 1.25 million Veterans, and is the fourth leading cause of death and disability in the United States (US).1,2 The Veterans Health Administration is the largest integrated health care system in the US, providing care at 172 medical centers. It serves approximately 9 million military Veterans who have been found to have a higher prevalence of COPD at 8–19%. 3 There are national, international, and Department of Veterans Affairs (VA)-based Clinical Practice Guidelines (CPG) for optimal diagnosis and management of COPD.4,5 Implementation of these COPD-CPG can improve patient outcomes by decreasing symptom burden, reducing exacerbations, and improving health status.1,2 However, uptake of COPD-CPG has huge voids. Spirometry, the objective tool for COPD diagnosis, is severely underused resulting in both under- and mis-diagnoses. 6 Only 56% of US COPD population receives guideline-concordant pharmacotherapy, 7 and only 3.7% of eligible Medicare patients 8 and 2% eligible Veterans 32 with COPD receive pulmonary rehabilitation. Fewer than half the patients receive COPD disease management education. 9 There is a significant relationship between guideline discordance and adverse outcomes.7,10 Reasons behind this insufficient uptake of COPD guidelines include providers’ low familiarity with guidelines, perception of minimal value of guidelines, and time constraints. 11
Studies attempting to improve COPD-CPG uptake have shown mixed results and the best practice to bridge this implementation gap remains unknown.11–13 For any attempt to improve COPD-CPG uptake, few salient points need to be considered. First, the majority of COPD patients are managed by primary care physicians, even outside the US. 14 Approximately 3.7 million adults in the US do not have access to a pulmonologist within a 1-hour driving distance. 15 Thus, primary care has a key role in COPD management. Second, we need comprehensive knowledge of all the factors that influence COPD-CPG uptake at primary care level. Thus, a systematic and rigorous evaluation of these contextual factors at the primary care level is the imperative first step. This is where use of implementation science principles could prove to be invaluable.
Implementation science is the scientific study of methods to integrate evidence-based practices (EBP), which in this case are the COPD-CPG, into routine clinical practice. 16 This interdisciplinary field is gaining momentum as the need to bridge the ‘knowledge to practice gap’ is becoming more palpable. Evidence suggests the time lag for incorporating research evidence into clinical practice may be as long as 17 years. 17 Furthermore, the EBP may need to be modified or ‘adapted’ from the way it was used in the original clinical trial for various reasons such as acceptability to target population or its feasibility in a clinical setting. These adaptations may in turn, augment or negate the effect of the EBP. 18 Thus, the adaptations also need to be systematically evaluated and reported. In implementation science language, the EBP is the ‘innovation’ and the set of activities to put the EBP into place would be the ‘implementation’. To bring about implementation, we use ‘strategies’ and ‘tools’, that can be identified systematically by a detailed assessment of the current state of practice, barriers, facilitators, and stakeholder priorities preceding and during the actual implementation. These factors that influence implementation outcomes are called ‘determinants.’ Another core element of implementation science is the use of conceptual models, theories or ‘frameworks’. 19 Frameworks provide a broad set of constructs that organize concepts and data descriptively without specifying causal relationships. 20
We conducted a pilot study applying a known implementation framework, the Consolidated Framework for Implementation Research (CFIR), in a qualitative study design, to identify factors that might influence implementation outcomes or could be important to inform implementation interventions. 21 The paper endeavors to report provider and patient perspectives about COPD-CPG in relation to four key aspects of COPD care: inhaler education and assessment of technique, pulmonary rehabilitation, spirometry testing and COPD-specific patient education; identify potential key implementation barriers; while illustrating the use of an implementation framework in analyzing provider and patient feedback to prepare for next steps of COPD-CPG implementation. These four COPD-CPG were chosen based on knowledge of existing contextual practice gaps, the actionable nature of these COPD-CPG and lack of pre-existing improvement initiatives to address these gaps.
Methods
Design
We used a qualitative study design to explore our aims via semi-structured interviewing. We used CFIR, a determinant framework, to ensure that we could identify the barriers and facilitators of COPD-CPG implementation. CFIR provides a menu of known determinants of implementation outcomes organized into five overarching domains (1) the intervention characteristics, (2) the characteristics of individuals involved with the implementation process, (3) the inner setting, (4) the outer setting, and (5) the implementation process itself. Moving systematically through the five CFIR domains, we narrow in on information that is relevant to implementation. 21 This information can be used to select strategies to address barriers and increase likelihood of success of implementation. The study was conducted in the US at a tertiary VA facility in primary care clinics. It was approved by local VA Institutional Review Board (Approval Number: 1682659-10). At the VA, primary care follows a team-based model of care in which a team of health professionals (including a physician/advanced practice nurse (APN), nurse, social worker, pharmacist, and administrative staff), works collaboratively with the patient to provide comprehensive patient care.
Participants
To obtain a range of perspectives we included both provider and patient participants. We aimed to enroll a pragmatic sample of 5-10 participants from each category. The ‘Providers’ category was comprised of physicians, APNs, pharmacists, and nurses to understand different viewpoints of all relevant provider types.
Patients with COPD (ICD-10 J44) who had a primary care encounter in the previous 6 months were identified based on international classification of diseases, tenth revision codes. Opt-out letters were mailed to these potential participants. Those who declined to participate or had underlying medical conditions that precluded their optimal participation in telephone interviews such as adults with impaired decision-making capacity were excluded.
Provider participants were contacted via email. To increase the rate of enrollment, we used Microsoft Teams (Microsoft, Redmond, USA), an online communication platform approved by the VA, which enables users to host virtual meetings and send instant messages. This has been shown to be efficacious in increasing provider participation. 22 We sent up to three instant messages to providers who did not respond before considering them a passive decline. All participants were verbally consented.
Procedures
Stakeholders were interviewed using semi-structured interview guides designed using the most relevant constructs of the CFIR framework [see Figure 1] as well as our known target components of COPD-CPG. Interviews were conducted virtually using Microsoft Teams software or telephone and lasted between 30 and 60 minutes. Interviews were audio recorded and transcribed verbatim. CFIR* domains and constructs addressed in this study. * CFIR- consolidated framework for implementation research.
Analysis
Transcripts were analyzed using rapid analysis techniques common in implementation science. In a series of steps, data was organized, reduced, and systematically analyzed, following an approach developed by Hamilton et al. 23 First, each interview was summarized using a template created in a Word document, organized by the topics of the interview guide (domains/constructs of CFIR). Two authors independently populated a draft summary for each interview and then met to compare and refine a final summary. Summaries were then compiled by entering results into an Excel table, known as a matrix in rapid analysis, which allows for comparison of results across participants and both within and across participant groups. Our matrices were organized by CFIR domains/constructs as outlined in Figure 1. The analysts then examined matrices for patterns and differences and created Word documents to describe results for both patients and providers for study domains of interest (e.g., inhaler education).
Results
Demographic characteristics of respondents.

Qualitative interview data: select quotes.
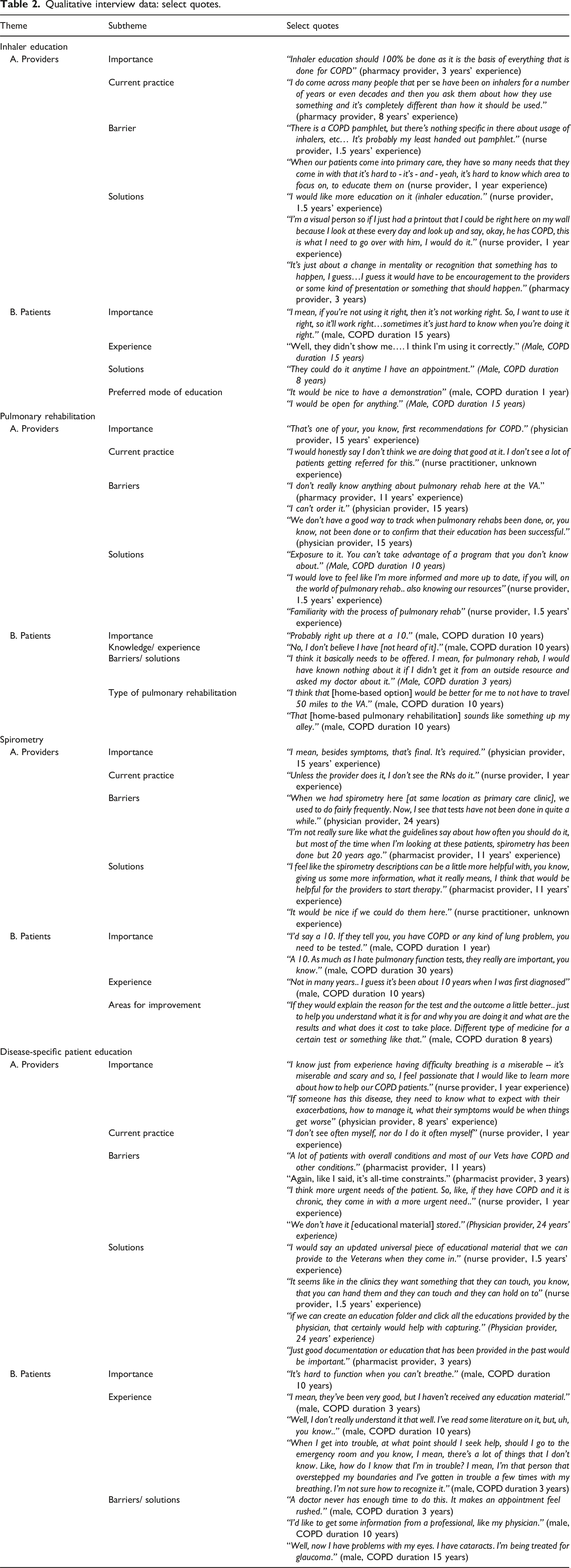
Inhaler education and assessment of technique
Providers reported very low rates for inhaler education using terms like “not being done at all” to describe it. Inhaler education was perceived to be complex but there was high receptivity to this intervention. The most common provider reported barriers to providing inhaler education included time constraints, lack of existing processes for inhaler training or educational resources such as educational handouts or demonstration inhalers for teaching purposes, and low familiarity with inhaler education (except for pharmacist-providers). Lack of standardized practices related to communication between primary care team members, documentation, and billing practices for inhaler education were other reported barriers. Providers suggested multifaceted interventions were needed to address this issue. Some recommendations mentioned by respondents to improve inhaler education included: (1) augmenting educational resources such as easily accessible patient educational videos/resources and procuring placebo inhalers; (2) use of the electronic medical record to facilitate reminders, communication and documentation; (3) increasing accountability by including COPD in performance measures; and (4) workflow adaptations to schedule inhaler education appointments.
Patients echoed provider statements regarding frequency of inhaler education. Most patient participants reported wanting in-person demonstration. When probed on using video telehealth for this, most respondents gave positive inputs. Patient-respondents had mixed opinions on handouts.
Pulmonary rehabilitation
The main provider-related barriers were knowledge about pulmonary rehabilitation, unfamiliarity with local resources, and challenges with referral process. Provider education on the benefits/indications of pulmonary rehabilitation, familiarizing primary care teams with the available resources, and adapting referral process to fit primary care workflows were the most recommended solutions to increasing referrals for pulmonary rehabilitation.
Most patients were not familiar with pulmonary rehabilitation, but once the program was explained to them in the interview, all the patient respondents rated pulmonary rehabilitation as ‘highly important’. Besides lack of knowledge of pulmonary rehabilitation, other barriers reported by patients were potential distance from the medical center, lack of transportation, and concerns about costs/billing. Education about pulmonary rehabilitation and its benefits was mentioned as most likely to increase patient acceptance of pulmonary rehabilitation. Between home-based and center-based pulmonary rehabilitation, patient-respondents’ reported highly favorable views of home-based option with responses such as “right up my alley” or “very good option”. Decreased mobility, transportation issues or work were major factors for patients rating home-based highly.
Spirometry use
Providers stated spirometry helped them to understand disease severity and/or direct further treatment. Most provider-respondents stated that primary care clinics were doing reasonably well but some of them noted a decline in the use of this test since the COVID pandemic due to alteration of resources/infrastructure. Facilitators from provider perspective to optimize use of spirometry testing included education on frequency of retesting with spirometry, spirometry testing location being adjacent to primary care clinics, and decreased appointment wait times. Clinical reminders to order spirometry were mentioned as an option to increase its use. However, providers stated that frequency of reminders would need to be carefully weighed; to avoid “reminder fatigue.”
Interestingly, only about 50% patient-respondents believed that spirometry had been done for them. Approximately a third of those, reported doing spirometry only at the time of initial diagnosis several years ago, but not since. Patients reported they would like more information about the test such as its indications, results, implications, and cost.
Patient education on COPD
There was considerable variation in providers’ reports of current practice in patient education. Inhaler education, medications, exacerbation management, vaccinations and smoking cessation were some of the topics addressed by providers who reported doing the education. Handouts from Mayo Clinic/Up to Date websites or online videos for inhalers were some resources providers used. Time constraint was the leading barrier for providers followed by lack of readily available and updated educational material. For specific topics like smoking cessation, patient receptivity was a perceived barrier. Providers were split on comparative value of handouts, which patients can “hold and touch” versus online resources. Workflow changes enabling other primary care team members to perform COPD-education and electronic medical record modifications to allow for easy documentation and capture of patient-education were additional solutions that emerged.
No patients reported receiving COPD education from primary care, and most were dissatisfied with their level of understanding of COPD. One recurring sub-theme was confusion about whether their lung disease was COPD or asthma. There was variability in patients’ preferred modality for disease-specific education. Over half the patients reported they would prefer some kind of face-to-face education, including telemedicine. An important sub-theme that emerged was the personalization of education to patient. For example, a patient with visual impairment noted how they could not use handouts. Patients stated they would like education on topics such as COPD treatment options, medication choices, prognosis, how to use inhalers, how to clean inhalers, symptom management and vaccination.
Discussion
The aim of this study was to explore the implementation determinants of COPD EBPs in a primary care setting in the US in relation to four key COPD guideline components. The qualitative interviews with providers and patients uncovered several important themes related to their perceived importance, current practices, existing gaps, and provided a deeper understanding of the reasons behind these practice gaps.
Providers and patients uniformly rated each of these EBPs as ‘highly important’. Despite this, our site has similar gaps in COPD-CPG implementation as reported in literature.2,6–9 This finding highlights the need for active implementation strategies to address the knowledge to practice gap. Provider or stakeholder education as a strategy to improve COPD-CPG uptake has a definitive role, but this study was able to uncover more nuanced targets for an educational strategy. Pulmonary rehabilitation was the least familiar guideline component for respondents. Most provider respondents were aware of the term ‘pulmonary rehabilitation’ but reported unfamiliarity with its indications and benefits. Most primary care providers (except pharmacists) reported they would need re-education to confidently educate patients on inhaler technique as well as an update on choice of inhalers. Lack of clarity regarding indications/ intervals for repeat spirometry testing was another area of knowledge gap. The perception of ‘high importance’ of these COPD-CPG practices by providers is a positive sign. Implementation science literature suggest that ‘perceived usefulness’ or ‘value’ of an ‘innovation’ (in this case the four COPD-CPG) has a positive correlation with adoption of the innovation. 24 Thus, implementation efforts targeting practices perceived as ‘highly important’ or ‘valuable’ are likely to have a higher chance of success.
Several themes regarding each of these COPD-CPG were identified including barriers and potential solutions. Frequently, the barriers described were multilevel. For example, to implement an inhaler education process, we need to consider provider time constraints, lack of easily accessible educational resources, multiple needs of a patient during primary care visit, lack of systematic practices regarding communicating need for inhaler education (for example, pharmacists did not know if physicians had done inhaler education and vice versa), and lack of standardized means of documentation. Each of these subthemes is ‘an active intervening variable’ that influences outcomes of an implementation effort addressing inhaler education. Use of implementation science frameworks promotes systematic and more comprehensive evaluation of such complex barriers. CFIR additionally offers a ‘matching tool’ which provides a list of implementation strategies to consider based on the identified CFIR-based barriers. 25
A previous study using surveys to understand barriers to adherence to COPD guidelines among primary care providers from US, identified poor familiarity with recommendations, low self-efficacy, and time constraints as important barriers. 10 Another study evaluating therapeutic nihilism by comparing continuing medical education interview responses of primary care providers from 2007 to 2013-14, found that the latter group reported greater awareness of COPD care guidelines and confidence in utility of COPD treatments. 26 Our data validates the continued importance of time constraints, and provider and patient belief in the ‘high importance’ of COPD guidelines.
In the current US practice model, a physician or APN is primarily responsible for addressing all aspects of COPD care. These providers often must address multiple comorbidities and meet several disease-specific metrics in a single encounter. Time-constraint is thus a commonly identified barrier. Consistent with recommendations from our providers, any implementation effort must be adapted to workflow and account for this barrier to be sustained. One possible option is to explore use of ‘non-physician/APN’ resources such as nursing and pharmacy. One example of this is the COPD Coordinated Access to Reduce Exacerbations program which has gained national prominence within VA health care in the US. In this collaborative program, veterans discharged from the hospital for an exacerbation receive a 45-min clinic visit with a clinical pharmacist and a registered nurse. The pharmacist provides COPD management such as prescribing therapy, ordering labs, and placing referrals, and the nurse provides education on flares and symptoms. 27 Such collaborative approaches serve to address time constraints and enhance relational coordination, an important attribute. A study looking at intersite differences in care coordination in relation to COPD readmission rates found that the most notable differences between high- and low-COPD readmission sites were related to the quality of relational coordination (high quality work relationships, high-quality communication) and the presence of structural barriers to coordination, rather than specific readmission reduction initiatives. 28 Such relationships could then be leveraged for management of other chronic diseases.
One limitation of most qualitative studies is the small sample size. The rigor of this exploratory study is reinforced with use of implementation science frameworks, and high concurrence in themes reported by providers and patients. The study respondents were from a single center and patients were predominantly male. These limitations may inhibit the generalizability of this data. However, this patient sample is reflective of the overall demographics of the COPD cohort, both at our center and in the overall VA health care system.2,29–31 We are aware that the team-based care model available at our setting may not be available in other contexts. The findings from the study highlight that Primary Care physician time-constraints are a significant barrier and collaborative care for COPD could be a potential solution.
Interpretation
Since primary care physicians are the first checkpoint for most patients with lung disease, this study examined the implementation determinants of four key COPD-CPG: inhaler education, pulmonary rehabilitation, spirometry, and disease-specific patient education in primary care. Using a determinant implementation framework like CFIR can enhance comprehensive identification of barriers and facilitators for implementation of complex EBPs. We found multilevel contextual barriers and this conceptualization is vital to promote appropriate choice of implementation strategies that help address more levels than one. Physician time constraint was a reported predominant barrier for any implementation effort. Thus, in addressing COPD-CPG use of non-physician resources such as nurses and pharmacists may have higher buy-in and chances for success.
Footnotes
Author contributions
DSR and JK are the guarantors of the article and take responsibility for the content, including data and analysis. All authors (DSR, JK and SAS, excluding KLD) were involved in data acquisition. KLD has made specific contributions to the use of qualitative methodology. The authors take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed substantially to the concept and design of the study, acquisition of the data, data analysis, interpretation of the data, or a combination thereof. All authors reviewed the manuscript for important intellectual content and jointly approved the final manuscript. The authors thank Danielle J. Bailey and James S. Williams for their contribution and all participants in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by funding from Department of Veterans Affairs, Veterans Health Administration, Health Services Research and by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Numbers KL2TR003108 and UL1TR003107. The views expressed in this article are those of the authors and do not represent the views of the U.S. Department of Veterans Affairs, US Government or National Institutes of Health.