
Abstract
Chronic obstructive pulmonary disease (COPD) is a persistent progressive respiratory disease that is increasing in prevalence and cost in the United States health care system. Delays in recognition, diagnosis, and treatment are associated with poorer clinical outcomes. These delays are seen more often in populations experiencing economic hardship, lack of access to care, and lack of insurance, such as those seen in an indigent care clinic. The COPD case-finding program was planned as an evidence-based quality improvement project with a prospective, descriptive design generating a convenience sample of patients meeting modified screening criteria (i.e. patients 40 years of age with a smoking history and no pulmonary disease history) in a community-based indigent care clinic which was not screening for COPD. Practice change recommendations were guided by the Diffusion of Innovations Model. Descriptive statistics were used to describe the sample (i.e. age, ethnicity, race, gender, income, and selected comorbidities). Sensitivity, specificity, positive predictive value, negative predictive value, prevalence, and receiver operator characteristics curve COPD Questionnaire were calculated for this sample.
Introduction
Chronic obstructive pulmonary disease (COPD) is an insidious and heterogeneous pulmonary condition characterized by a symptom cluster of cough, breathlessness, and sputum coupled with progressive airflow obstruction. 1–3 COPD is the third leading cause of mortality in the United States and is associated with almost a US$50 billion health care burden annually. 4 Although early recognition is imperative to initiate interventions, COPD diagnosis usually does not occur until the later stages of the disease trajectory with urban and underserved areas experiencing a disproportionate lack of diagnosis and treatment. 5–7
The International Primary Care Respiratory Group (IPCRG) guidelines recommend a case-finding approach to diagnose, which focuses on patient symptoms and signs consistent with COPD. 8 A tool, such as the 10-item validated COPD Questionnaire (sensitivity: 0.59–0.80; specificity: 0.58–0.77; positive predictive value (PPV): 0.30–0.37; negative predictive value (NPV): 0.89–0.93; and receiver operator characteristics (ROC) curve: 0.82), 9,10 is recommended to screen patients aged 40 years or older with a 20-pack year smoking history 5 (PYSH) or exposure to other COPD risk factors (i.e. dusts, chemicals, home cooking, or heating fuel smoke) and no history of a pulmonary disease. 11 For patients with a positive COPD Questionnaire score (i.e. score of 17 points or more), the IPCRG guidelines recommend a focused physical examination, pre–post bronchodilator challenge spirometry, a trial of bronchodilator, and/or inhaled or oral corticosteroid therapy. 11
The COPD case-finding program was planned as an evidence-based quality improvement project with a prospective, descriptive design generating a convenience sample of patients meeting screening criteria (i.e. patients 40 years of age with a smoking history and no pulmonary disease history) in an indigent care clinic. The project was designed to answer the following clinical questions: What are the characteristics of the COPD Questionnaire results in this indigent care clinic setting? What is the prevalence of undiagnosed COPD in high-risk patients seen at this indigent care clinic? If high-risk patients are diagnosed with COPD, will treatment initiation be congruent with global initiative for chronic obstructive lung disease (GOLD) guidelines?
Based on answering these clinical questions, the indigent care clinic could determine the utility of implementing the COPD case-finding program, with recommendations for practice change guided by the Diffusion of Innovations Model (DOIM).
The indigent care clinic was not screening high-risk patients before the implementation of the COPD case-finding program, leaving an estimated 10–20% of high-risk patients with a smoking history undiagnosed and lacking appropriate treatment to prevent disease progression. 12 The COPD case-finding program instigated screening high-risk patients at the indigent care clinic with the COPD Questionnaire and conducted pre–post bronchodilator challenge spirometry to confirm COPD Questionnaire findings. For patients with spirometry indicative of COPD, the GOLD guidelines were used to stage the level of COPD (i.e. level of airway obstruction, COPD assessment test scoring, and number of exacerbations in the past 12 months) and make recommendations to each patient’s health-care provider for appropriate interventions using a standardized order set.
Methods
Setting
The mission of the Lloyd F. Moss Free Clinic (LFMFC) is to provide comprehensive health-care services to the local indigent population in the Fredericksburg, Virginia region. The clinic is a privately operated nonprofit health organization governed by community citizens and leaders. In 2011, the LFMFC received US$1.7 million in donations, grants, and proceeds from fund-raising events that equated into US$33 million of services to its patients. In 2012, the LFMFC had a population of almost 2000 patients, saw over 10,000 patient encounters annually, and enrolled about 20 new patients each week. LFMFC acts as a medical home (i.e. free medical care, access to free specialty referrals, and minimal cost prescription medications) for low-income patients without health insurance in Fredericksburg, Virginia region. This evidence-based quality improvement project increased access to resources and treatment for LFMFC patients at risk for COPD.
Participants
Over nine recruitment days between November 2012 and January 2013, the COPD case-finding program screened 39 current and previous smokers without any pulmonary diagnosis at the indigent care clinic. A power analysis using nQuery Advisor 7.0 for a one group χ 2 test of proportions (i.e. assumptions: α = 0.05 with two-sided test, π 0 = 0.5; π A = 0.72; and β = 0.2) calculated the minimum required sample size to be 39 (i.e. completed screenings). Reasons for patients not being screened included left clinic before being asked (n = 9), time (n = 9), didn’t want testing (n = 3), remote history of cigarette smoking (n = 2), already screened (n = 4), recent cerebrovascular accident (n = 1), acute pain (n = 1), rib fracture (n = 1), recent eye surgery (n = 1), and unhealed abdominal surgery (n = 1). Patients meeting the screening criteria (24 women, 15 men, M age = 51.9 years, age range: 41–64 years) were screened initially with the COPD Questionnaire each recruitment day. Of the 39 participants, the majority of the sample identified themselves as not Hispanic or Latino for ethnicity (n = 37). There was a fairly homogenous racial background with two Asian, 14 Black or African American, and 23 White or Caucasian participants. The two Hispanic or Latino participants declined to identify with a particular racial group. There were nine previous smokers (M PYSH = 24, PYSH range: 1–50) and 30 current smokers (M PYSH = 25, PYSH range: 1–69). Spirometry values for those participants diagnosed with COPD (post bronchodilator challenge forced expiratory volume in 6 seconds (FEV6) = 3.12 [84% predicted]; forced expiratory volume in 1 second (FEV1) = 1.92 [64% predicted]; FEV1/FEV6 = 61%) were less than those participants not diagnosed with COPD (postbronchodilator challenge FEV6 = 3.2 [88% predicted]; FEV1 = 2.63 [89% predicted]; FEV1/FEV6 = 82%). Predicted values were manually calculated using the National Health and Nutrition Examination Survey (NHANES) spirometry reference values. 13
Evidence-based quality improvement model
DOIM was used as a guiding framework for the project. 14 The DOIM provided a comprehensive approach to address clinical practice change as an innovative process. Components of the DOIM included were system antecedents, system readiness, adopter characteristics, assimilation elements, implementation processes, linkages, resource system, knowledge purveyors, and change agency system. The sustainability of the COPD case-finding program also considered provider training, work flow integration, and durable and nondurable medical equipment costs.
Measures
Thirty-nine patients determined to be high risk for COPD and meeting inclusion criteria were included in the project. Patients unable to follow instructions and provide consent for care were not included. These patients were initially screened with the COPD Questionnaire and then had confirmatory pre–post bronchodilator (i.e. albuterol) challenge spirometry. The COPD Questionnaire was a validated 9-item tool with a possible range from 0 to 38, higher scores indicating higher risk for COPD with a positive score being 17 points or higher. Spirometry was performed using the PIKO-6 handheld spirometer with manual calculation of patient predicted values based on NHANES reference values. The PIKO-6, a spirometer validated for primary care, was selected based on initial and maintenance cost since the LFMFC did not have a spirometer nor the money to purchase. 3 Patients completed the screening process while waiting for, or just after, the clinic appointment.
COPD staging included further assessment with the COPD assessment test, and the number of self-reported exacerbations in the past 12 months, both of which were required to determine appropriate level of treatment. A COPD exacerbation was defined as a self-reported episode of acute bronchitis infection requiring antibiotics. The COPD assessment test was a validated 8-item tool with a possible range of 0–40, higher scores indicating more negative impact of COPD on a patient’s health. 15
Human subjects protection
The evidence-based quality improvement project was reviewed by the Mary Washington Hospital Investigational Review Board for primary oversight and adjunct oversight provided by the Duke University Investigational Review Board.
Statistical analysis
Descriptive statistics were used to describe the sample (i.e. age, ethnicity, race, gender, income, and selected comorbidities). Sensitivity, specificity, PPV, NPV, prevalence, and ROC curve COPD Questionnaire were calculated for this sample. Statistical analyses were conducted in the Statistical Software Package for Social Sciences version 20 (SPSS Inc., Chicago, Illinois, USA).
Results
Data
Analyses focused on the COPD Questionnaire results and their congruence with the pre–post bronchodilator challenge. There were 12 participants with a positive COPD Questionnaire score of 17 or greater (M score = 21 points, score range: 17–28 points), and there were 27 participants with a negative COPD Questionnaire score of 16 or less (M score = 10 points, score range: 4–16 points. In 27 patients (69%), the COPD Questionnaire and spirometry agreed; however, in 12 patients (31%) the COPD Questionnaire and spirometry disagreed. There were four positive pre–post bronchodilator challenge spirometry tests. There were 2 true positives (M score = 21 points, score range: 20–21 points), 25 true negatives (M score = 10 points, score range: 4–16 points), 10 false positives (M score = 21 points, score range: 17–28 points), and 2 false negatives (M score = 14 points, score range: 13–14 points; see Figure 1, for distribution with average COPD Questionnaire scores and Table 1, for clinical characteristics). Based on the congruence of the COPD Questionnaire with the findings of the pre–post bronchodilator challenge spirometry, the sensitivity was 50%, the specificity was 71%, the PPV was 17%, the NPV was 93%, and the area under the curve (AUC) was 67% for the COPD Questionnaire (see Figure 2, for the ROC curve for the COPD Questionnaire in this sample).

Mean COPD questionnaire scores distribution. COPD: chronic obstructive pulmonary disease.
Clinical characteristics.a

BMI: body mass index; PYSH: pack year smoking history; FEV6: forced expiratory volume in 6 seconds; FEV1: forced expiratory volume in 1 second; COPD: chronic obstructive pulmonary disease; GOLD: global initiative for chronic obstructive lung disease.
aData are presented as n (%) or mean ± standard deviation.
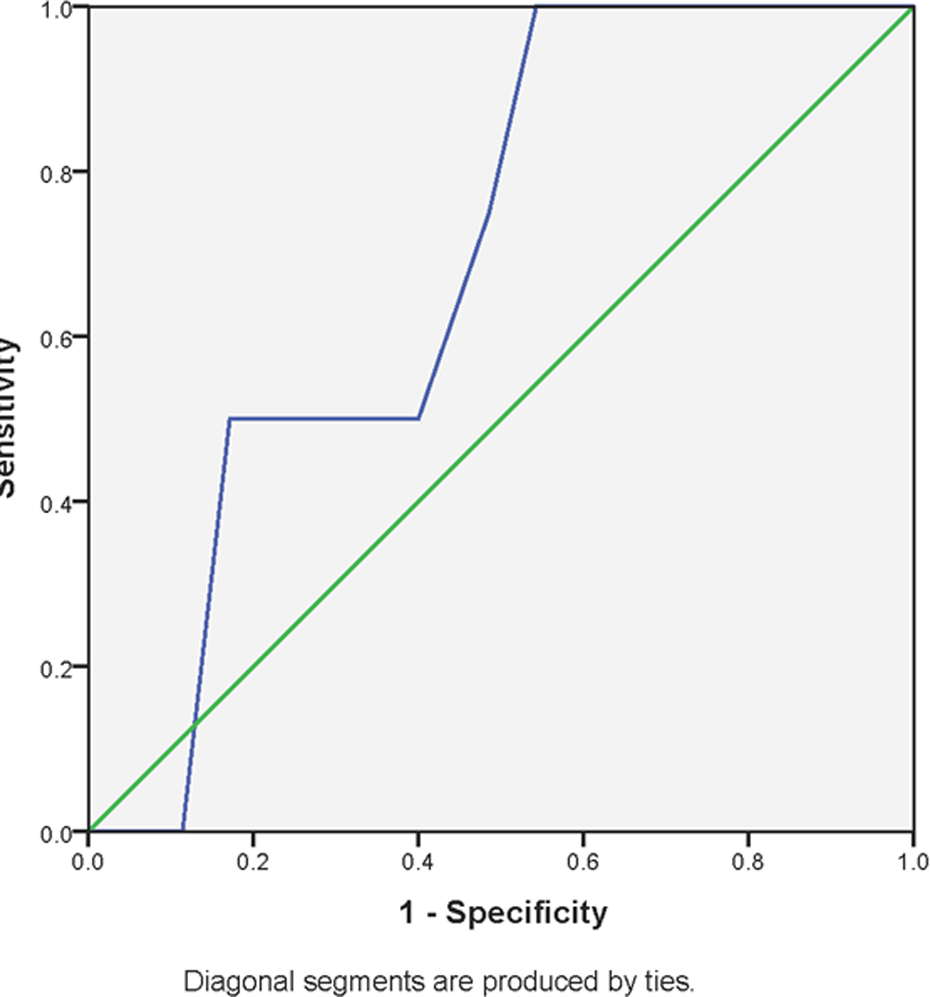
The ROC curve for the COPD questionnaire in this sample. ROC: receiver operator characteristics; COPD: chronic obstructive pulmonary disease.
The overall prevalence of COPD in the sample was 10%. All COPD patients were GOLD patient type B based on the amount of airway obstruction, COPD assessment test score, and the number of exacerbations in the last year (see Table 2, for combined assessment of COPD). The COPD assessment test score mean was 16.25 with a range of 12–20, with higher scores suggesting more impact of COPD on the patient’s health. Two patients self-reported no exacerbations in the last year, one patient self-reported one exacerbation in the last year, and one self-reported two exacerbations in the last year.
GOLD combined assessment of COPD.

COPD: chronic obstructive pulmonary disease; GOLD: global initiative for chronic obstructive lung disease.
aOne patient had two exacerbations in last 12 months but was at level B for the other two variables.
A chart review revealed that all patients diagnosed with COPD based on the COPD case-finding program had pharmacologic treatment initiated. By the end of the data collection, no smokers had been referred to the clinic smoking cessation program. However, the LFMFC’s standard practice is to assess and encourage smoking cessation at each clinic visit. All interested patients are provided an education calendar with a listing of the bimonthly smoking cessation classes. The pharmacologic treatments initiated were all congruent with GOLD guidelines.
Discussion
As discussed previously, the COPD case-finding program screened high-risk patients with the COPD Questionnaire, conducted pre–post bronchodilator challenge spirometry, staged positive spirometry tests based on the GOLD guidelines, and tracked treatment initiation. The project was designed to answer the three clinical questions posed earlier. The DOIM was also used to make recommendations to the LFMFC administration for continuing the COPD case-finding program.
What are the characteristics of the COPD questionnaire in this indigent care clinic setting?
The COPD Questionnaire has similar epidemiological properties in this sample of high-risk patients to what is published. A highly specific tool is used to “rule in” a disease and has high PPV, whereas a highly sensitive tool is used to “rule out” a disease and has a high NPV. The sensitivity (0.50) estimated in this sample is less than the lower limit published (0.59–0.80). However, the specificity (0.71) is within the published range (0.58–0.77). The PPV (0.17) is lower in this sample as compared to what is published (0.30–0.37), while the NPV (0.93) is at the higher limit published (0.89–0.93).
What is the prevalence of undiagnosed COPD in high-risk patients seen at this indigent care clinic?
Since the prevalence of COPD in this sample was fairly low at 10%, it is not surprising to find the PPV to be lower than what is published. Fletcher and Fletcher noted that as the disease prevalence decreases, so does the PPV. Furthermore, the lower sensitivity, prevalence, and PPV most likely resulted in a lower AUC. The AUC for the COPD Questionnaire in this sample is above chance (0.67), but it was less than published values (0.82). The larger the AUC is, the better the test. 16 A test that is no better than flipping a coin would have an AUC equal to 0.5.
If high-risk patients are diagnosed with COPD, will treatment initiation be congruent with GOLD guidelines?
Those patients who were diagnosed with COPD were all GOLD patient type B, indicating moderate disease. At this level of disease, patients should be treated with a smoking cessation referral, physical activity regimen, annual influenza vaccination, pneumococcal vaccine one before the age of 55 and one after the age of 55, and one of three medication regimens (i.e. SPIRIVA® HandiHaler® or SEREVENT® DISKUS®; SPIRIVA® HandiHaler® and SEREVENT® DISKUS®; or atrovent HFA or Ventolin® HFA or Combivent®). Since none of the patients were at the mild COPD level, this may explain why health-care providers preferentially initiated pharmacologic treatment at the initial visit over nonpharmacologic treatments. Also, the LFMFC culture is to assess patient smoking status at each clinic visit and encourage cessation. The clinic has its own bimonthly smoking cessation program.
The utility of the COPD Questionnaire at the indigent care clinic
The COPD Questionnaire demonstrated good epidemiological characteristics in this sample of patients. Of concern are the 10 false positive patients and 2 false negative patients. False positive patients would be subjected to further evaluation that is not necessary and the potential for side effects associated with pre–post bronchodilator challenge spirometry. False negative patients would not be diagnosed, delaying treatment that could prevent the progression of COPD. Therefore, any high-risk patients with a positive COPD Questionnaire score would need to be evaluated further by a clinical health-care provider to determine appropriateness of pre–post bronchodilator challenge spirometry. Also, any high-risk patients meeting the initial screening criteria (patients 40 years of age or older with a smoking history and no pulmonary disease history) who have a negative COPD Questionnaire score should be rescreened with the COPD Questionnaire yearly to increase the likelihood of detecting further changes in the patient’s pulmonary status.
The COPD Questionnaire, as part of a COPD case-finding program, is a robust and clinically useful tool that can detect high-risk patients requiring referral for confirmatory pre–post bronchodilator challenge spirometry to diagnose COPD. Implementing a COPD case-finding program holds potential to increase COPD diagnosis at earlier stages of the disease trajectory and initiate appropriate treatment interventions earlier to prevent progression of the disease. The COPD case-finding program addresses a disproportionate problem seen in urban and underserved populations seen in indigent care clinics.
DOIM-based recommendations
Components of the DOIM that were addressed in this project were system antecedents, system readiness, adopter characteristics, assimilation elements, implementation processes, linkages, resource system, knowledge purveyors, and change agency system. The LFMFC staff were both very receptive and positive about the COPD case-finding program; however, with only six full-time patient care staff, absorptive capacity to continue the program is limited due to staffing and space issues. Although the COPD case-finding program was a priority identified by the LFMFC administration, it was the frontline staff who have to implement the screening procedures, decreasing the probability of sustaining change. The elimination of on-site spirometry in favor of off-site spirometry via referrals to local pulmonary clinics would need to occur due to staffing, space limitations, and training requirements. Economic pressures forced the LFMFC to change its emphasis from the medical home model to doing the most good for the most patients. Hence, resources are scarce at the LFMFC and any continued implementation of the COPD case-finding program will need to be scaled back. In light of the new clinical milieu, the adopters, that is, staff, would likely resist change unless done incrementally over time. Therefore, the initial adoption of the COPD Questionnaire with off-site spirometry would probably be more readily adopted. Founded on best practices, the COPD case-finding program was also supported by marketing to the LFMFC staff and providing resource materials (i.e. education materials, posters, etc.) for both the staff and the patients. Electronic versions of these resources were provided to the LFMFC administration for future reference. The recommended implementation of the COPD Questionnaire and off-site spirometry (i.e. referrals) is the least resource intensive at about 55 minutes of staff time per referral. The LFMFC administration will need to reevaluate the clinical milieu over time to ascertain success or failure of the incremental adoption of the COPD case-finding program. At present, the LFMFC plan to reinstitute the COPD case-finding program in the next 6 months to 1 year.
Conclusion
In conclusion, a COPD case-finding program holds potential as an effective process to screen and diagnose high-risk patients in an indigent care clinic setting. The COPD Questionnaire is a highly reliable and valid tool that when coupled with pre–post bronchodilator challenge has robust specificity and acceptable sensitivity for COPD. Pharmacologic interventions may seem more favorable to health-care providers when diagnosing and managing COPD during the first few visits. However, the LFMFC culture is to ask about smoking habits and promote smoking cessation at each clinic visit. Using the DOIM as a guiding framework demonstrates the complexity of changing clinical practice in an ever changing clinical environment. Emphasis must be made on simple, incremental change that can adapt to the dynamic forces existing in the clinical environment.
Footnotes
Authors’ Note
This evidence-based quality improvement project was part of the requirements for the Doctor of Nursing Practice degree at Duke University School of Nursing for Dr Estes. The additional authors were capstone committee members, Drs Anne Boyle and Donna Bowser, and chair, Dr Nancy Short. Dr David Price, the creator of the COPD Questionnaire, was a consultant for the use of the COPD Questionnaire and reviewed this manuscript.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.