
Abstract
Global Initiative for Chronic Obstructive Lung Disease guidelines support the prescription of fixed combination inhaled corticosteroids (ICS) and long-acting β-agonists in symptomatic COPD patients with frequent or severe exacerbations, with the aim of preventing them. ICS are frequently also prescribed to COPD patients with mild or moderate airflow limitation, outside guidelines, with the risk of unwanted effects. No investigation to date has addressed the views of these milder COPD patients on ICS withdrawal. The objective is to assess the views of COPD patients with mild or moderate airflow limitation on the staged withdrawal of ICS prescribed outside guidelines. One-to-one semi-structured qualitative interviews exploring COPD patients’ views about ICS use and their attitudes to proposed de-prescription were conducted. Interviews were audio-recorded and transcribed verbatim. Thematic analysis was completed. Seventeen eligible COPD patients were interviewed. Many participants were not aware they were using an ICS. None was aware that prevention of exacerbations was the indication for ICS therapy or the risk of associated side effects. Some were unconcerned by what they perceived as low individual risk. Others expressed fears of worsening symptoms on withdrawal. Most with mild or moderate airflow limitation would have been willing to attempt withdrawal or titration to a lower dosage of ICS if advised by their clinician, particularly if a reasoned explanation were offered. Attitudes in this study to discontinuing ICS use varied. Knowledge of the drug itself, the indications for its prescription in COPD and potential for side effects, was scant. The proposed withdrawal of ICS is likely to be challenging and requires detailed conversations between patients and respiratory healthcare professionals.
Introduction
International guidelines support the use of fixed combination inhaled corticosteroids (ICS) and long-acting β-agonists by symptomatic patients with chronic obstructive pulmonary disease (COPD) who experience, or are at risk of, frequent exacerbations. 1 Adherence by both primary and secondary care prescribers to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidance on the prescribing of ICS is variable. 2 –4 Patients with COPD with mild or moderate airflow limitation are frequently prescribed ICS outside guidelines. 5 Although the use of ICS reduces the frequency of exacerbations in selected groups of COPD patients, there is limited evidence of their effect in modifying long-term decline in lung function or mortality in these patients. 6,7 Long-term use of ICS in stable COPD is associated with an increased risk of unwanted effects including pneumonia, cataract and osteoporosis. 8 In addition, these drugs represent a large financial burden for health services 9 when used inappropriately. It has been acknowledged that ICS withdrawal should be considered in those patients with COPD who are unlikely to benefit. 10
The rising prevalence of polypharmacy has accompanied an increased focus on deprescribing of medication in routine clinical practice. 11 Patient enablers and barriers to drug deprescribing have been described, 12 but few assessments of patients’ experiences of, or views about, drug withdrawal have been conducted. Patient enablers when stopping drugs include unwanted effects and fear of them, 13,14 perceived lack of efficacy, 15 dislike of the drug, 16 greater awareness of the benefits of stopping 17 and adequate support by health professionals during withdrawal. 15 Barriers to stopping include psychological benefits of the drug, fear of stopping, 18 inadequate information from healthcare professionals about the drug 19 and inadequate healthcare support when withdrawing. 20 Successful deprescribing may be enhanced by recognition of the competing barriers and enablers which influence patients’ attitudes to the process.
The views, beliefs and attitudes of older adults towards deprescribing have been explored in focus groups. 21 Influences on older adults’ willingness to have medication withdrawn mirror the results of generic studies and include in particular the role of the GP and the prescriber–patient relationship. 22 –25
Older adults are willing to consider medication withdrawal, provided they understand why it has been suggested. 21 This willingness contrasts with a perception among prescribers, sometimes justified, 26 of a reluctance among their patients to stop medication. 27,28 To date, the perceptions and attitudes of COPD patients towards the proposed withdrawal of ICS have not been explored.
Aim
The aim of this study was to investigate the views of COPD patients with mild or moderate airflow limitation on the proposed withdrawal of ICS prescribed outside guidelines. Participants’ views were sought to inform a subsequent feasibility study of the staged withdrawal of ICS.
Methods
This qualitative interview study was the first stage of a feasibility study of the withdrawal of ICS in COPD patients with mild or moderate airflow limitation. A range of potential benefits of qualitative research to the development of trial design and completion have been identified. These include the assessment of the feasibility and acceptability of an intervention, providing insight into the contextual circumstances of the implementation and facilitating interpretation of the trial findings. 29 –31
Data were collected at semi-structured interviews, supported by a topic guide (Table 1). This study design was used to explore the experiences and views of participants using ICS including any concerns they may have when faced with the proposal to withdraw one of their regular inhalers and the acceptability of the proposed ICS withdrawal to patients. The methodology was chosen to provide more in-depth understanding, providing insights into participants’ opinions, thoughts and feelings that are difficult to capture in other methods of data collection including questionnaires. The topic guide was developed with the support of our COPD patient advisory group. Interviews were facilitated by one of the investigators (GG) who has a background in physiotherapy and is an experienced qualitative researcher.
Qualitative interview topic guide.
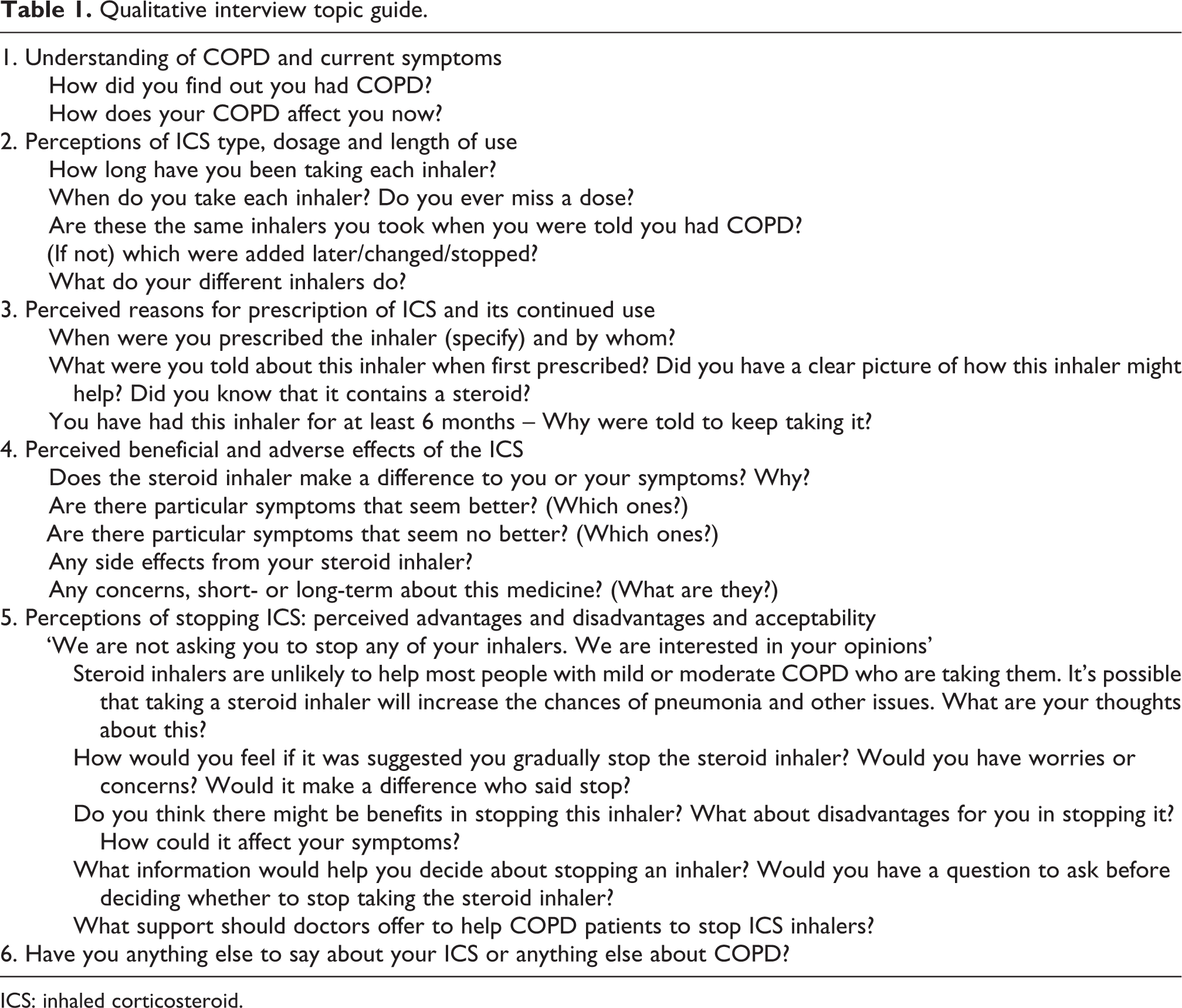
ICS: inhaled corticosteroid.
Study participants
Potential participants were identified by computer search of electronic records in participating general practices in north and south London and sent a postal invitation to take part by the practice. Non-responders were followed up by postal reminder and then telephone. Those who expressed an interest in participating were then telephoned by the research team and an appointment agreed to conduct the interview in their homes or in another preferred place such as their GP’s surgery. At the interview, the study was first explained, and spirometry carried out if the participant provided written informed consent. Inclusion criteria included diagnosis of COPD with mild or moderate airflow limitation (spirometry confirmed forced expiratory volume in 1 second (FEV1) >50% expected), age >45 years, currently taking ICS (defined as >400 mg beclometasone dipropionate or equivalent/day) in combination with a long-acting β-agonist, fewer than two moderate exacerbations (requiring oral antibiotics or corticosteroids) in the previous year where known, body mass index <35 and fluent in spoken English. Exclusion criteria included no recorded diagnosis of asthma, significant other physical or mental health problems that would interfere with participation, taking continuous oral corticosteroid, active lung cancer, breathlessness due to cardiac disease, alcohol dependency or dementia and not enrolled in the second stage of the feasibility study.
Ethical approval was provided by the National Research Ethics Service (NRES) Committee, London Bridge. Research Ethics Committee (REC) reference 16/LO/1696.
Data collection and analysis
Interviews were digitally recorded and transcribed verbatim. Follow-up questions and prompts were tailored to the individual participant’s responses with the purpose of clarifying and expanding on areas of importance to the participant or of relevance to the research objectives. The interview transcripts were analysed using a thematic content approach with themes derived primarily from topics in the interview guide (deductive analysis). 32 Two coders (GG and PW) checked a sample of seven transcripts for inter-coder verification. The agreed themes formed a coding index used as a means of coding each subsequent transcript. Coding of relevant sections and an iterative process of refining the thematic structure was completed through reading and rereading the data.
Results
Seventy potential participants were identified in eight general practices in the London boroughs of Camden, Croydon, Lambeth, Southwark, Sutton and Wandsworth. The recruitment process is shown in Figure 1. All the potential participants who expressed interest (n = 26) were followed up and interviewed if available during the study period. Two interviews that had been arranged did not take place because the patients were unwell. The recruitment period was extended beyond the initial, planned 6-month period. Limitations of time and resources prevented recruitment of additional participants beyond those completed during the 10-month recruitment period (October 2017 to July 2018). No new themes were identified in the transcripts of the final two interviews; however, further participants were not available to confirm data saturation had been reached. Participant demographic characteristics are presented in Table 2.
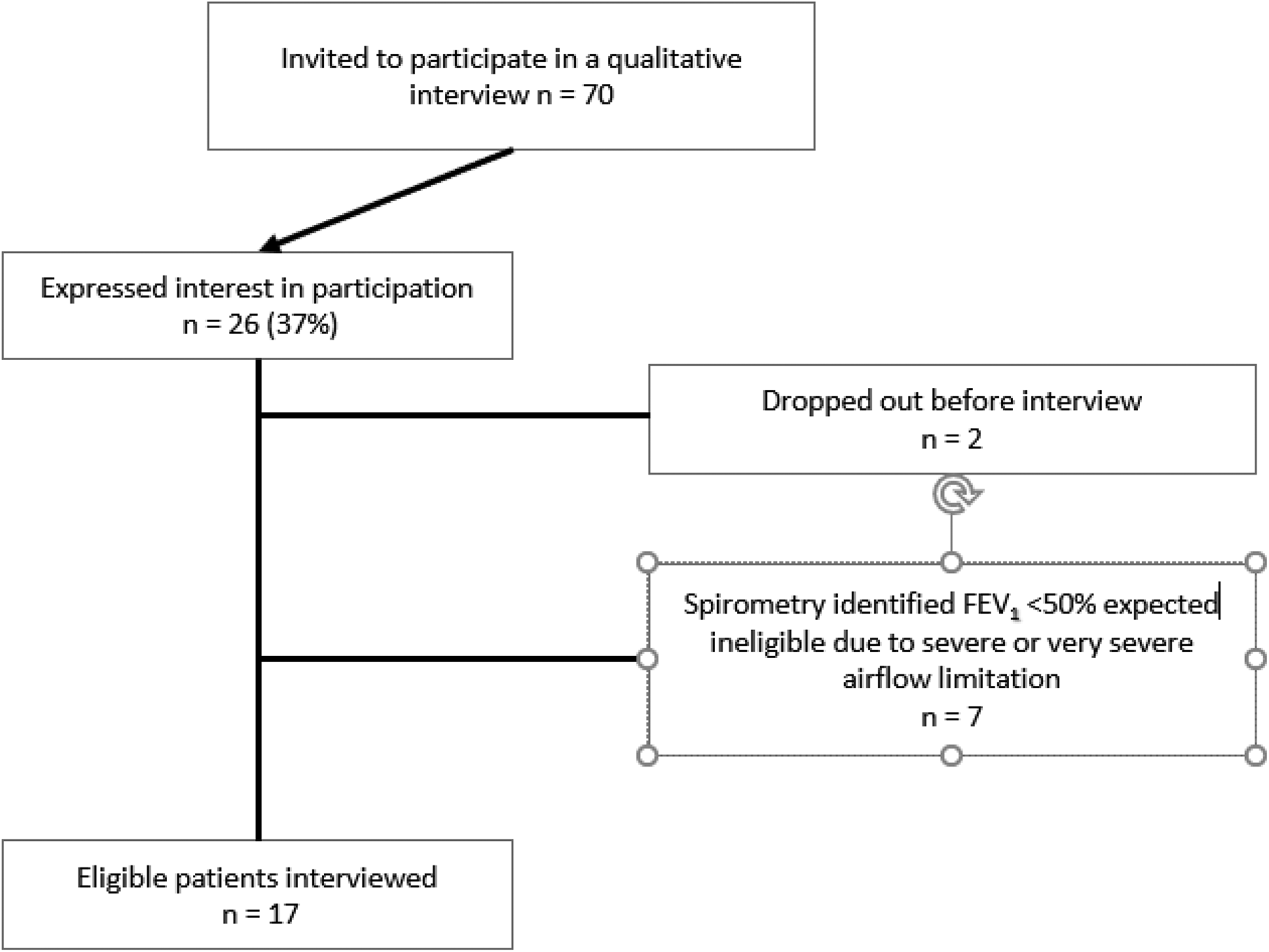
Recruitment flow diagram.
Characteristics of participants.

FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; IQR: interquartile range.
Interview length varied between 24 minutes and 40 minutes. The seven main themes identified (Table 3) stem from the topic guide compiled with our COPD patient advisory group. The opinions and reflections of the participants on the topics discussed in the interviews are presented in the “Results” section linking key quotes to the themes listed here.
Main themes from data.

ICS: inhaled corticosteroid.
1. Patients’ understanding of COPD
Participants generally understood that they had a chronic condition and that while deterioration might be minimized if they were able to reduce or stop smoking, there was no cure. There was some confusion over the term COPD: Interviewer: So, they told you that you had emphysema from looking at your X Ray. Did someone also use the term COPD? My doctor used the term COPD. My specialist – he used the term emphysema. (Pt 10) you can’t take a breath back in because you’re not emptying your lungs. (Pt 15) 2. Symptoms
Participants described the range of symptoms that might be expected related to their COPD including cough, breathlessness, particularly with physical activity and tiredness. They explained the variable nature of their symptoms and the impact on day-to-day and social activities which can lead to a feeling of isolation: my breathing’s it’s like good days and bad days. (Pt 18) now everybody overtakes me while I’m walking. But it’s that sort of thing that I noticed.…I have got a cough a lot of the time, but the way it really affects me is walking. (Pt 13) for instance, I wouldn’t be able to go to the theatre in the evening, because I know I’m likely to break into coughing and everybody will want to lynch me. So I don’t go.…I find the worst attacks are when I’m on the telephone…awful for them listening to me struggling and spluttering. So I tend not to make telephone calls.…It tends to cut me off from people. (Pt 10) 3. Exacerbations
The frequency of participants’ experience of ‘flare-ups’ of their symptoms varied. Some participants had first been diagnosed with airways limitation following an acute exacerbation (at times referred to as chest infections by patients). Some who had experienced a recent exacerbation described how frightening they can be: To be honest with you, I get frightened, because I have difficulty in breathing. And that’s – as you understand, that, that can be rather scary…(Pt 10) since I’ve had that [ICS] I haven’t had any chest infection at all. (Pt 15) 4. Inhalers
Many participants did not understand how their different inhalers work beyond knowing that their blue inhaler was a ‘reliever’ that could be used as needed if they experienced wheezing or a feeling of tightness in their chest. Some participants were confident their ICS helped their symptoms: they’ve [symptoms] been different in that they’ve been less frequent, much less frequent and much less severe.…I think this is good for me. (Pt 15) I didn’t know it was a steroid…I know I should have – but I didn’t…I think doctors will be, and nurses too – will be well advised to explain very, very fully what these medicines are supposed to do…I have been taking this for years, and I’ve never been quite sure what it’s supposed to do. (Pt 10) so the old symptoms came back.…This included extreme dryness – I tended to have more headaches, and also I had the strange.…I don’t know whether it’s connected or not, skin irritations. I started to itch and I thought this – this is no coincidence, surely? (Pt 10) 5. Attitude to taking the ICS
Some participants had a general perception that steroids are ‘bad’ or at the very least may be a ‘necessary evil’. One participant (Pt 04) repeated a number of times that she would prefer not to have to take medicines at all if she did not have to and steroids in particular.
When talking about steroids, some participants associated them with misuse in sport. I – think of dishonest athletes and footballers are on steroids and they’re doing – and so you have a dismal picture of it. Of steroids…obviously there’s a place for steroids. They’re very important in medicine. But, I’m sorry, I do have an unholy prejudice against the word steroid. (Pt 04) I’d forgotten my medications, and I thought never mind…and I found something quite amazing. When I was off the [named ICS] I actually felt better. I coughed less…I still had to use my Ventolin, but I did not feel that I suffered any loss while not having it. (Pt 10) 6. Thoughts/feelings if suggested that they could stop ICS
Some participants expressed fears of deteriorating symptoms should they withdraw their ICS treatment. Reservations about withdrawal were positively associated with a perception of benefit in symptoms from the ICS; some would simply follow instructions from their doctor. It would be very difficult to convince somebody to come off it…I don’t think I could do it, I don’t think anybody could do it, if it has been as effective as it has been to me. To come off it would be almost panic, nervous, taking a chance (Pt 03) Well if the doctor told me to do that, I do what the doctors tell me, I would – if he said ‘you’ve got to stop taking it’, I’d stop taking it.…I wouldn’t be worried about it. (Pt 20) obviously if the doctor advises it…if a doctor said come off it I’d come off it, but it would depend who was telling me, if it was a researcher you know, I wouldn’t, I would want to know more about what they’re qualifications are to say so. (Pt 16) I would pay more attention to my doctor or the nurse than a pharmacist. I would take their advice. But I don’t think I’d stop just on the advice of the pharmacist. (Pt 14) 7. Support people with COPD might need if they agreed to stop ICS
When thinking about the support people might need if they were to withdraw from their ICS, participants felt that there should be monitoring of symptoms. This could be done in a number of different ways, for example, either over the telephone or face-to-face with any healthcare professional including a doctor, nurse or pharmacist. It was important to participants that if they were asked to stop taking their ICS, they would have the option to resume it if symptoms deteriorated. obviously it’s got to be monitored hasn’t it?…say right, you come off it and we monitor you, I don’t know once a week, see how you are…and there’s any reaction, they go back on it. (Pt 18) I think doctors will be, and nurses too – will be well advised to explain very, very fully what these medicines are supposed to do. They – if they just took five minutes with each one, to say look this is what they’ll do, and explain it so that the, you know, the layman can understand it fully. (Pt 10)
Discussion
This qualitative interview study documents the knowledge and perceptions of participants with COPD with mild or moderate airflow limitation of the ICS therapy prescribed for them in a primary care setting. Many did not know that the inhalers contained corticosteroids. None knew that the prevention of moderate or severe exacerbations was the sole indication for the prescription of ICS in COPD. None knew of the documented unwanted effects of pneumonia, cataract and osteoporosis that have made the usage of these drugs in this situation the subject of controversy. The participants’ attitudes to the possible withdrawal of these drugs were informed by fear of deteriorating symptoms, confidence in the symptomatic benefits of using the drugs prescribed and scepticism about potential side effects once made aware of them. Additional influences included confidence in the ultimate expertise of the prescriber and a desire for adequate and detailed explanation of the basis for the advice given, embracing the evidence for the effectiveness of the drugs and their potential for harm. All these factors are recognized, empirical barriers or enablers in deprescribing, 12,21 so it is no surprise to find them in this study of withdrawal of ICS.
Among the lessons learnt with respect to COPD participants’ knowledge and perceptions of ICS was their poor understanding of the identity of the drug, why exactly it had been prescribed and its possible unwanted effects. These findings might be interpreted to suggest that patient information and education about their condition and its treatment was a low priority in their prescribers’ approach. It is well acknowledged, on the other hand, that understanding and knowledge may deteriorate with time, and therefore inappropriate to assume that these problems necessarily arose from poor assessment of understanding and provision of information at the initial prescribing consultation. Despite the evident important gaps in their knowledge, many participants had high regard for the authority and expertise of their healthcare professionals. Some would have taken advice to withdraw ICS at face value. Others wanted detailed information and explanation.
While research evidence suggests that ICS are largely ineffective in controlling symptoms in COPD, 1 some participants were confident that their ICS therapy was the cause of improved symptoms. These participants may have had evidence of responsiveness to ICS in reversibility of airway obstruction or eosinophilia. 33 On the other hand, the benefits in symptoms may have been due to the long-acting β-agonist component of the fixed combination inhaler.
This study is the first, to the best of our knowledge, addressing a qualitative examination of attitudes to withdrawal or deprescribing of ICS in patients with COPD with mild or moderate airflow limitation. Strengths of the study include its novelty, its contribution to the growing field of deprescribing, spirometry confirmation of the diagnosis and of the degree of airflow limitation and the exclusion of potential participants who had experienced two or more exacerbations in the previous year. Participants were recruited from seven different general practices in London. We make no claim for representativeness of the entire affected population, since this is a qualitative study, but we think it likely that recruiting from a range of general practices has increased the likelihood of uncovering a broad impression of experience of prescribing practice in our participants. Nevertheless, we cannot be certain that we captured a full range of views of people with COPD with mild or moderate airflow limitation from the relatively small number interviewed, in addition to the fact that the participants were self-selected. This is the principal, potential weakness of the study. A further potential limitation is that although no new themes were identified in the final two interviews, further participants were not available to confirm data saturation had been reached.
In conclusion, this research was conducted as the first stage of a feasibility study for a clinical trial of withdrawal of ICS in COPD patients with mild or moderate airflow limitation. It has shown the potential for difficulty in withdrawing inappropriately prescribed drugs in COPD when patients do not know the nature of the drug or its indication or side effects. This study has implications for the prescribing of ICS and their subsequent withdrawal when prescribed outside guidelines. Ensuring patients have a correct and suitable understanding and knowledge of drugs prescribed is a fundamental requirement of safe clinical practice. This understanding and knowledge may deteriorate with time. If such patients are approached to initiate appropriate withdrawal of ICS, the possibility that they are ignorant of essential information about the drug should be assumed in the clinician’s assessment.
Footnotes
Authors’ note
The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. TH is in receipt of an NIHR Doctoral Research Fellowship. GG and TH are joint first authors.
Acknowledgements
The authors would like to thank all the participants who gave their time and agreed to be interviewed. The authors would also like to acknowledge the contribution of our COPD patient advisory group throughout the study from the design stage to the writing up of the findings. The research team acknowledges the support of the National Institute for Health Research Clinical Research Network (NIHR CRN).
Author contributions
PW and TH conceptualized the study. GG and TH wrote the first draft of this article. GG was responsible for recruiting and consenting participants. TH and GG contributed equally to this article. GG and PW analysed the data. All authors contributed to data interpretation, drafting and revising the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the financial support for the research, authorship, and/or publication of this article: This article presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (grant reference no. PB-PG-0214-33060).