
Abstract
To evaluate the impact of participant-selected music listening as an adjunct to pulmonary rehabilitation (PR) in people with COPD. Adults with COPD referred to PR were randomly assigned to participant-selected music listening (intervention group, [IG]) or usual care (control group [CG]) during an 8-weeks PR program. Prior to training, the IG completed an interview with a registered music therapist to identify music preferences. IG participants listened to an individualised playlist; CG participants had usual care. Primary outcomes included end-6-min walk test symptoms (dyspnoea and exertion) and dyspnoea (Multidimensional Dyspnoea Profile [MDP]), measured pre and post PR and 6-months follow-up. 58 participants, FEV1 52.4 (25.9)% pd) were recruited. There were no between-group differences following the intervention (p > .05 for all outcomes at all time points). Within-group differences following PR were significant for MDP sensory quality: IG mean difference [95% CI] −2.2 [−3.3 to −1.2]; CG −1.5 [−2.5 to −0.5] points; MDP emotional response: IG −3.2 [−4.2 to −2.3]; CG −2.2 [−3.2 to −1.3] points). Participant-selected music listening during PR offered no greater benefit to symptoms of dyspnoea or exertion compared to usual care. With the study limited by COVID-19 restrictions, the role of this adjunct remains to be clarified.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by dyspnoea, fatigue and reduced exercise tolerance. 1 Concomitant anxiety is often associated with exertional dyspnoea2–4 and is linked to reduced physical activity. 5 International guidelines for managing COPD includes pulmonary rehabilitation (PR).6,7 This recommendation is supported by compelling evidence that PR improves exercise capacity and reduces dyspnoea, fatigue and anxiety, all of which enhance health-related quality of life (HRQOL).6–8 However, not all people with COPD accrue symptom improvement from PR, with 46% classed as non-responders. 9 In addition, maintaining benefits following PR remains a challenge, 10 with decline in physical activity partially attributed to lower confidence and motivation. 11
One potential approach to desensitise individuals with COPD to dyspnoea and fatigue experienced during exercise is music listening.12,13 Listening to music during exercise alters symptom perception, switching the focus from concentration on symptoms to an external attention on music.14–16 Music listening during exercise is an adjunct which can be individualised to accommodate genre and artist preferences. 17 When applied during home-based, paced-walking interventions in COPD, improvements in exercise capacity, and reductions in physical symptoms have been observed18,19 However, these interventions do not align with all components of a PR program, with an absence of strength training and in one study, an extended training duration.18,20 While background music can accompany the warm-up and exercise components of PR programs, 21 guidance in music choice is lacking. Applying music listening during outpatient PR may be an adjunct which could enhance improvements in symptoms, exercise tolerance and HRQOL, but the effect of participant-selected music listening during this intervention in COPD is unknown.
This study aimed to determine the effect of participant-selected music listening on dyspnoea and end-6-min walk test (6MWT) symptoms in COPD. The secondary aims were to establish the effects of this adjunct on exercise capacity, HRQOL, fatigue, psychological symptoms and enjoyment of physical activity.
Methods
Study design and participants
The study design was a multi-centre, prospective, randomised controlled trial, with allocation concealment and masking of outcome assessors. Three sites were included: PR outpatient programs at West Park Healthcare Centre, Toronto, Canada; St Joseph’s Hospital, Thunder Bay, Canada; and Northern Health, Melbourne, Australia. The trial was registered prospectively (NCT02980575). The study was approved at local ethical committees and all participants provided written informed consent. Reporting procedures aligned with CONVERSE-CONSORT statement for trials interrupted by the COVID-19 pandemic. 22
Participants were eligible if they met the following criteria: 1) COPD diagnosis (physician diagnosis and spirometry, with forced expiratory ratio <70), smoking history >10 pack years, 1 and clinically stable (no exacerbations in the past 6 weeks). Potential participants were excluded on the basis of: predominant diagnosis of a respiratory condition other than COPD (bronchiectasis, interstitial lung disease); substantial hearing difficulties (due to potential inability to adequately hear music or use earbuds with hearing aids); already listening to participant-selected music during exercise/activity; or comorbidities which prevented the ability to safely exercise.
Participants were recruited from PR referrals at each of the sites by research team members. They were randomised to either participant-selected music listening (intervention group [IG]) or usual care (control group [CG]) (1:1 allocation) via computer-generated randomisation, with stratification for oxygen therapy use. The rationale was that oxygen tubing was considered a cumbersome physical attachment in addition to earbuds. Sequence generation was performed by an individual independent of the research team; randomisation occurred via sequentially numbered opaque envelopes. Following baseline assessment, participants were randomly allocated by a researcher not involved in participant recruitment or intervention delivery.
Intervention
All participants undertook an 8-weeks PR outpatient program, attending twice weekly for supervised and individualised exercise. The exercise prescription followed PR guidelines for chronic respiratory disease6,20 and are outlined in Supplemental File 1. Pulmonary rehabilitation completion was defined as attending at least 70% (11 of 16) of supervised sessions. 23 Once a participant had an established supervised regimen, an unsupervised home exercise program was prescribed; the goal being two to three additional exercise sessions per week. At the PR program’s conclusion, all participants were encouraged to continue with their exercise routine, four to five times per week.
Participants in the IG group completed the Short Test of Music Preference. This questionnaire assessed music genre preference. 24 The questionnaire findings were shared with a registered music therapist who used this information during a single online assessment via Zoom with each IG participant. The music therapist guided participants to select music they felt would promote physiological arousal while exercising.25,26 Participants selected a music playlist from the iTunes (Apple) online store with music at a minimum tempo of 90 beats/minute; this selection aligned with a PR maintenance study in which music at this tempo improved symptoms and exercise capacity. 27 During the interview, participants rated the motivational quality of their selection using the Brunel Music Rating Inventory-2, a scale with motivational quotients facilitating music selection during exercise. 28 Selected music was uploaded onto a portable music playing (mp3) device with earbud headphones, with 25 to 30 songs for each participant. Participants were instructed to choose music from this device during each PR exercise (endurance and resistance training) session, for sessions at home and following PR completion for 6 months.
Participants in the CG were exposed to usual care. Usual care included conversation between fellow participants or with clinicians, no music or clinician-selected background music. The choice (including use of music, its tempo and genre) and frequency of these options was at the discretion of the clinicians consistently. Participants in the CG were not permitted to listen to any participant-selected music listening during the study. This was monitored in-person by PR clinicians during the supervised program and remotely during follow-up. Participants in the IG and CG attended the PR program at the same time.
Outcome measures
Participants undertook the following measures at baseline (prior to randomisation and before commencement of PR), immediately following PR (9 weeks) and 6 months after PR conclusion by an assessor unaware of group allocation (Figure 1). Participant schedule. Legend: + = completed; − = not completed.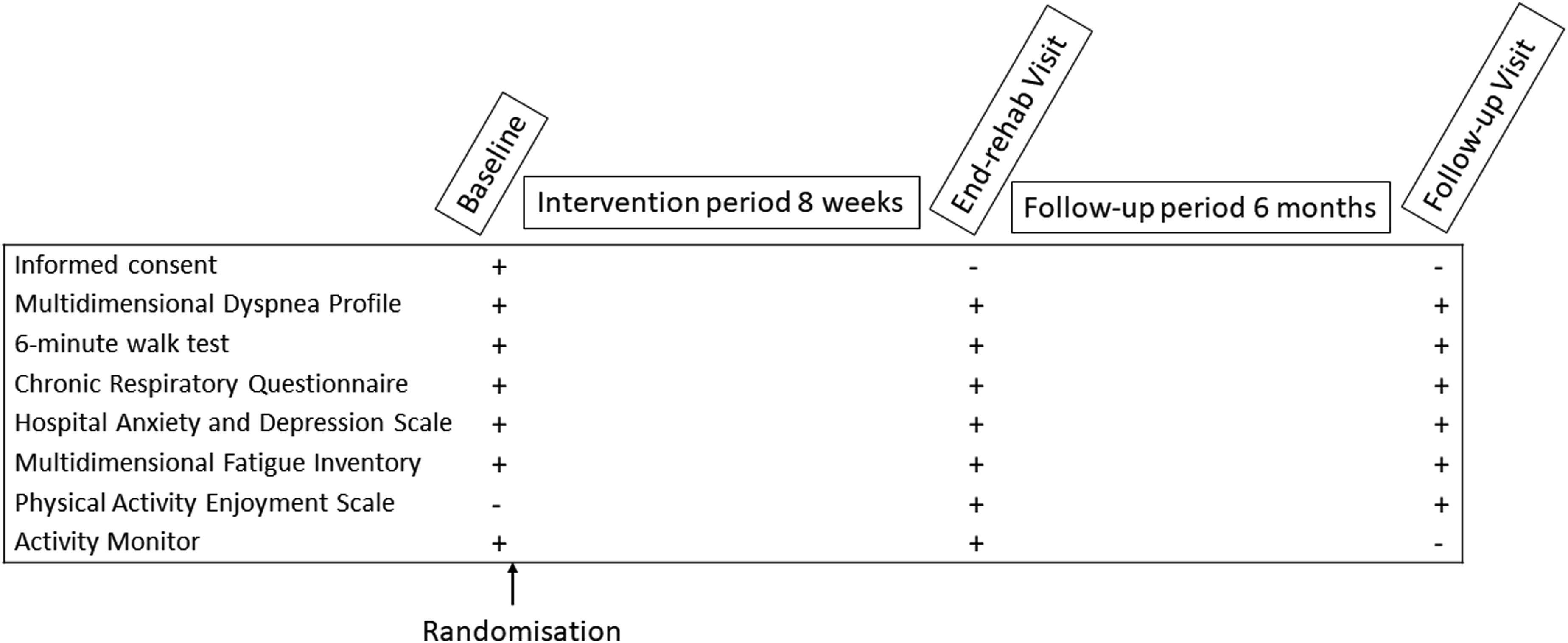
Primary outcomes
Functional exercise capacity was measured using the 6MWT, a validated test of functional exercise capacity in COPD. 29 The 6-min walk distance (6MWD) is responsive to change following PR.29,30 Two tests were completed at each assessment time; the best of two tests were recorded with conditions consistent with standardised guidelines. 29 Dyspnoea (modified Borg [0–10]) and leg fatigue (perceived exertion rating [6–20]) measurement were recorded at the beginning and conclusion of each test. 31 The primary outcome was the end-6MWT symptoms scores. This was selected to enable assessment of the impact of music listening immediately following exercise bouts on symptoms which are a common source of daily limitation experienced by people with COPD.
Secondary outcomes
Demographics of age, sex, baseline lung function (spirometry), baseline exertional dyspnoea (modified Medical Research Council dyspnoea scale), 42 and oxygen therapy and rollator use were also collated.
Sample size
Primary outcomes
To detect a difference greater than 1 point in the Borg dyspnoea scale (minimal important difference [MID]) 43 end-PR 6MWT, and assuming a standard deviation (SD) of 1 point, 44 with 80% power and an alpha of 0.05, 20 participants per group were required, accounting for 20% attrition. To detect a difference in the MDP sensory quality of 1.5 points 45 and a SD of 2 points, 33 accounting for 20% attrition, 35 participants per group were required.
Secondary outcomes
To detect a difference in 6MWD greater than 30 m (MID), 29 with a SD of 33 m, 46 with 80% power and an alpha of 0.05, 48 participants were required. To detect a difference in 10 points (total CRQ score MID), 34 assuming a SD of 10 points, 47 with 80% power and an alpha of 0.05, 43 participants per group were required.
Data analysis
Data were analysed according to intention-to-treat principles using Statistical Package for Social Sciences (SPSS v27.0, Chicago, Illinois). Baseline comparisons between groups were analysed using Chi-Square, Independent t-tests or Mann Whitney U tests, depending on data distribution. Between-group differences were evaluated using linear mixed models with three fixed effects: group (intervention or control), time (time-points of baseline, post-PR and 6-months after training completion), group x time interaction and random effects. The effect of treatment over time (interaction effect) constituted the principal endpoint of analysis, however, post hoc between-group comparisons at each relevant time-point were performed using least significant differences adjustment. Participants who completed their PR program (attending 70% or more of sessions) 23 were included in a per-protocol analysis using the same methods as the primary analysis. Alpha was set at <0.05.
Results
Between August 2016 and March 2020, 164 patients with COPD were screened and 58 were randomised, with 26 (45%) recruited at the Canadian sites and 32 (55%) at the Australian site. Twenty-eight participants were recruited to the IG and 30 to the CG (Figure 2). The CONSORT checklist is outlined in Supplemental File 2. With the declaration of the global COVID-19 pandemic, recruitment and provision of the centre-based intervention was interrupted, with the cessation of face-to-face PR programs and in-person assessment at all sites from 16th March 2020 for 2 years. These limitations, changes in referral frequency of potential participants and a pause in PR delivery due to staff leave at one site (in Australia) resulted in recruitment ceasing at 58 participants (Supplemental Figure 1). Thus, the overall sample size was not achieved for primary and secondary outcomes and 6MWT data collection was incomplete. This was interpreted as extenuating circumstances, which impacted interpretation of the study findings
22
and is reported in CONSERVE-CONSORT statement (Supplemental File 3). The mitigating strategies implemented are outlined in Supplemental File 4; their aims were to honour our commitment to enrolled participants, optimise cohort retention, minimise missing data and continue to conduct the trial where feasible and safe. Difficulties were also encountered in obtaining physical activity monitors in Australia. Data for this outcome was only collected at the Canadian sites for 17 participants at baseline and 12 participants post-PR; for this reason, the physical activity data are not reported. Flow of participants.
Demographic characteristics of participants.
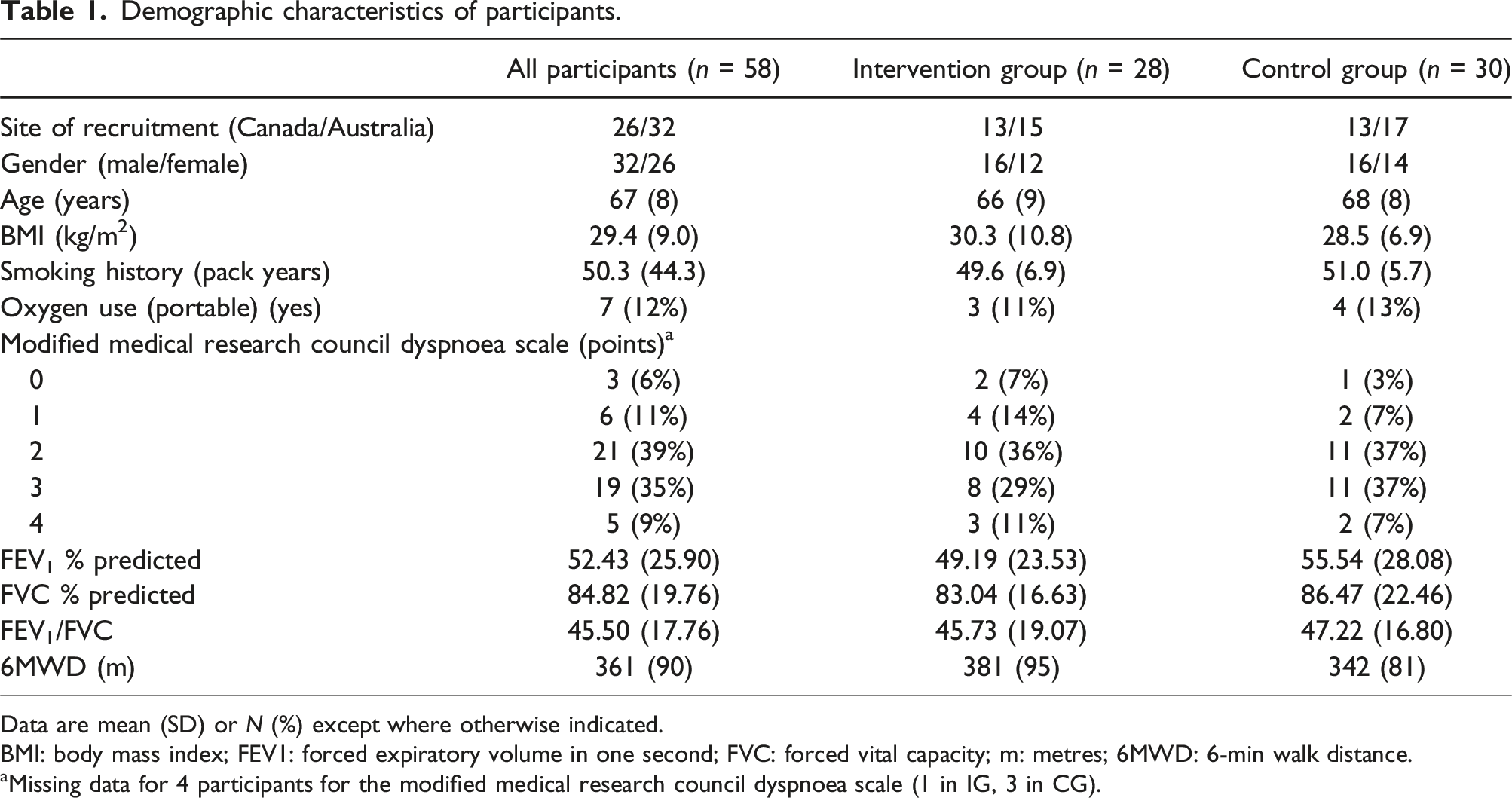
Data are mean (SD) or N (%) except where otherwise indicated.
BMI: body mass index; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; m: metres; 6MWD: 6-min walk distance.
aMissing data for 4 participants for the modified medical research council dyspnoea scale (1 in IG, 3 in CG).
Exercise capacity, health-related quality of life and symptom-related patient-reported outcomes at baseline, end-intervention and 6-months follow-up.
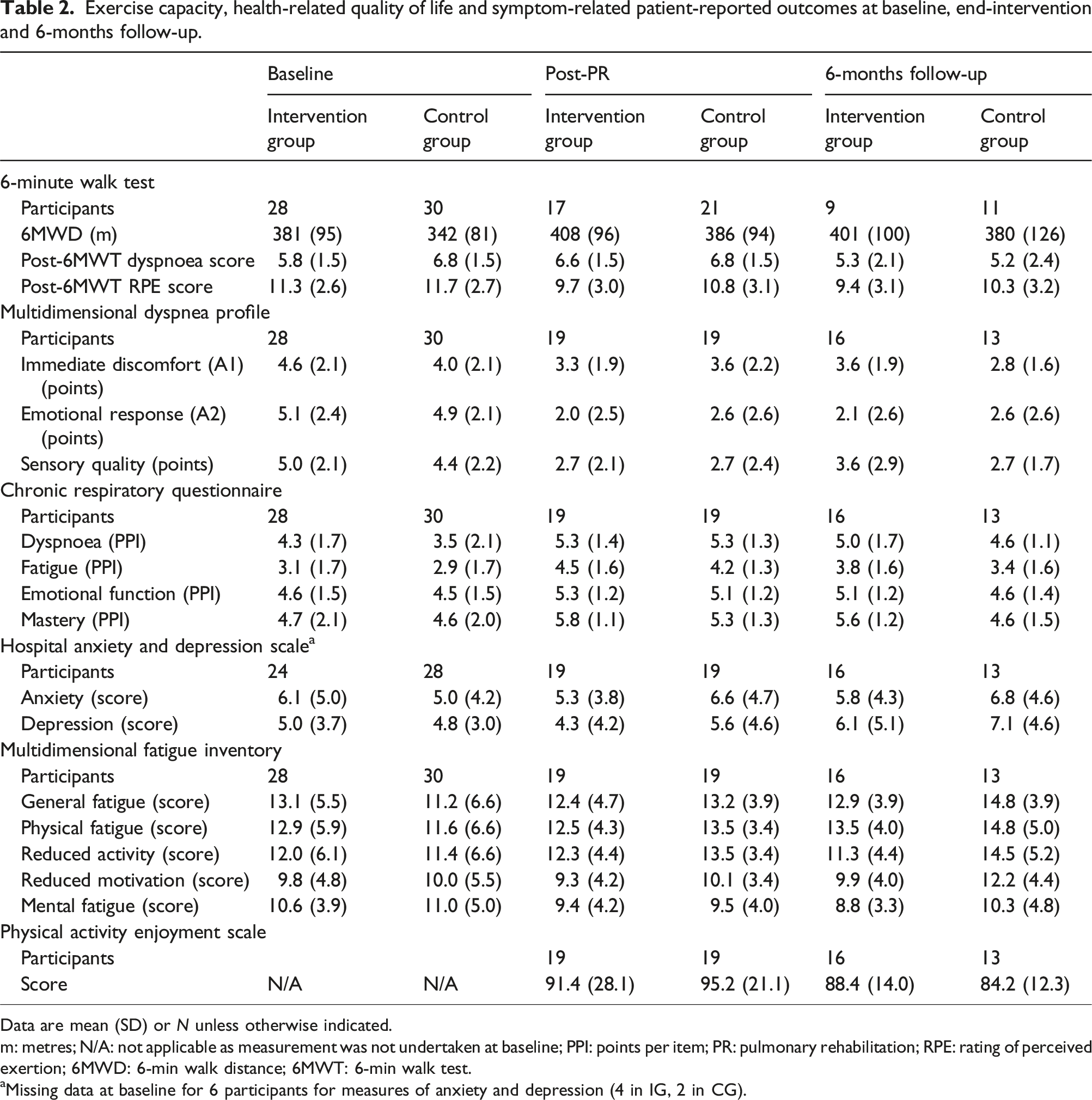
Data are mean (SD) or N unless otherwise indicated.
m: metres; N/A: not applicable as measurement was not undertaken at baseline; PPI: points per item; PR: pulmonary rehabilitation; RPE: rating of perceived exertion; 6MWD: 6-min walk distance; 6MWT: 6-min walk test.
aMissing data at baseline for 6 participants for measures of anxiety and depression (4 in IG, 2 in CG).
Primary outcomes
Within-group and between-group statistical analyses.

Data are presented as estimated marginal mean difference and 95% CI.
m: metres; N/A: not applicable as measurement was not undertaken at baseline; PPI: Points per item; PR: pulmonary rehabilitation; RPE: rating of perceived exertion; 6MWD: 6-min walk distance; 6MWT: 6-min walk test.
aSignificant within-group differences from baseline.
At 6-months follow-up, there was no between-group difference in the end-6MWT symptom scores or MDP dimensions (Table 3). Within-group analyses showed a significant reduction in dyspnoea scores in the CG. Within-group analyses of the MDP showed significant improvements in sensory quality and emotional response (A2) from baseline to 6-months follow-up in both groups (Table 3).
Secondary outcomes
There were no between-group differences in the change in 6MWD immediately following PR or at 6-months follow-up (Table 3). Within-group analyses following PR showed a significant improvement in both groups; this was only retained in the CG at follow-up. While there were no between-group differences in CRQ domains following PR or at 6 months, both groups demonstrated significant improvement in dyspnoea, fatigue and emotional function domains immediately following PR, with the IG also improving in mastery (Table 3). Only the dyspnoea domain improvement was retained in the CG at follow-up. No differences in anxiety or depression were observed between groups following PR or at 6 months. There were no between-group differences in fatigue measures following PR or at 6 months (Table 3). Within-group analysis showed the CG had less mental fatigue following PR, but more general, physical fatigue and reduced activity at 6 months, while the IG had less mental fatigue at 6 months. There was no between or within-group differences for physical activity enjoyment.
Per protocol analyses
Thirty-four participants (16 in IG, 18 in CG) met the inclusion criteria for per-protocol analyses (Supplemental Tables S1–S3). Similar to the intention-to-treat results, there were no between-group differences in changes from baseline in the primary or secondary outcomes at end-training or at 6-months follow-up. There were selected improvements within-groups for aspects of dyspnoea measurement and HRQOL domains, with some improvements retained at 6-months.
Discussion
This is the first study examining the effect of participant-selected music during an 8-weeks centre-based PR program on clinical outcomes. This intervention did not result in greater improvements in symptoms of dyspnoea or end-6MWT symptoms, compared to usual care in COPD. Nor were any benefits noted for functional exercise capacity, HRQOL, fatigue, psychological symptoms or enjoyment of physical activity. However, the extenuating circumstances of an interrupted and early study cessation due to the COVID-19 pandemic should be considered when interpreting these findings.
The planned sample size for this study was 70 participants for primary outcomes (MDP) and 96 for secondary outcomes. The COVID-19 restrictions (lockdowns and interrupted programs), 48 limited the ability to achieve our target sample for most outcomes. The restrictions also imposed limitations for outdoor exercise and usual physical activity. Recruitment challenges were further hampered by an inability to undertake the 6MWT to an acceptable standard 29 in the home environment. These restrictions limited our ability to detect statistical or clinically meaningful differences between groups. Furthermore, while not statistically significant, the baseline 6MWD difference (39 m) between groups is clinically meaningful; this may influence the ability to detect change in this outcome.
Our findings also contrast to other studies examining participant or clinician-selected music listening during exercise.18,19,27,49 Some studies noted improvements in dyspnoea, leg fatigue and exercise capacity,18,19 others reporting mixed effects on dyspnoea, with improvement during daily activities but not post-6MWT. 27 The training duration may be relevant with improvement in symptoms, exercise capacity and HRQOL noted for programs of at least 8 weeks.18,19,27 While the PR program in this study had an 8-weeks duration, compliance with exercise during the follow-up period was unknown; this may have influenced the results at the 6-months timepoint. We applied a minimum tempo of 90 beats/min, similar to a PR maintenance study which improved dyspnoea and exercise capacity, 27 but not purposely synchronised to each individual IG participants’ walking speed. Previous research has suggested that older persons with health conditions may be more motivated by music which has strong personal associations to promote positive intrinsic experiences during exercise rather than tempo. 50 Although not yet established, similar factors for participant-selected music listening may apply to those with COPD. Participants in the IG were given a maximum of 30 songs on their mp3 player, with no opportunity to update their playlist. Over the study duration, participant interest in their music selection may have diminished and potentially reduced the intervention’s efficacy.
The lack of impact on psychological symptoms was surprising, given improvement in anxiety was achieved with clinician-selected music during a single session of PR. 49 This may be attributed to low levels of anxiety and depression at baseline across all participants, which limited the scope for improvement. Despite the lack of between-group differences, the improvements in the MDP’s immediate distress (A1) and emotional response (A2) beyond their minimal important difference (0.82 points and 2.37 points respectively) 51 immediately following PR in the IG provides a preliminary indication that an 8-week outpatient PR with participant-selected music listening may be able to target affective qualities of dyspnoea. This mirrors similar improvements in affective and sensory qualities of dyspnoea noted in a retrospective review of 4-weeks PR programs. 52 However, the 8-week duration applied in this study aligns with global recommendations for PR6,7 and lends support for the role of this format of PR to address a mix of dyspnoea dimensions. The lack of effect on fatigue within-groups following PR is surprising, given previous reports of improvement in fatigue following PR. 53 Further research to clarify the effect of participant-selected music listening for these outcomes with adequate power is warranted.
Response to music is individualised and influenced by many factors including age, sex and intrinsic and extrinsic motivation. 54 A greater degree of enjoyment has been observed amongst healthy individuals and those with COPD when exercising with their preferred music.16,55,56 The lack of withdrawal from both IG and CG is indicative that participants were content with complying with study conditions, which lends support to the viability of this clinical adjunct in PR. Although our study findings did not illustrate benefits of participant-selected music listening on key clinical outcomes, the perceptions and experiences of IG participants may provide further insight into perceived advantages. One study in cardiac rehabilitation demonstrated that self-selected music listening which synchronised music tempo to walking speed improved participants’ physical activity 57 ; this would merit from future exploration in the context of PR. The control condition for this study was usual care, which included background music, no music and/or interactive conversations. A recent survey of a small number of Australian PR programs revealed that 88% of programs used background music. 21 This illustrates the need to further understand the impact of individual elements of the control condition applied in this study on these clinical outcomes independently, and in comparison to participant self-selected music listening.
In this randomised controlled trial, the exercise training program was representative of programs commonly provided in PR,6,20 reflected by within-group improvements in exercise capacity and HRQOL measures. However, PR program interruption and loss to follow-up due to COVID-19 was substantial. The focus on participants with COPD prevents the ability to generalise findings to other respiratory conditions. Although participants in the IG group used headphones, the earbuds were not noise cancelling, as participants were required to engage with clinicians to ensure safety during exercise. The lack of this feature indicates it is possible that background noise may have been noticed by IG participants.
In summary, participant-selected music did not impact upon symptoms and clinical outcomes compared to usual care. However, the study was limited by COVID-19 interruptions which inhibited the ability to reach an adequate sample size. Therefore, the potential role of participant-selected music listening as an adjunct to PR remains to be clarified.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial
Supplemental Material for Participant-selected music listening during pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A randomised controlled trial by Annemarie L Lee, Stacey J Butler, Peter Jung, Imogen N Clark, Jeanette Tamplin, Roger S Goldstein and Dina Brooks in Journal of Chronic Respiratory Disease.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of participants, registered music therapists Alice Cotton and Sophia Christopher for undertaking participant interviews, Tamara Araujo and Cindy Ellerton for assistance in data collection, Matthew Rhim for his assistance in preparing playlists for Canadian participants and Dr Tim Powers (Statistical Consultant, Monash Data Futures Institute, Monash University) who guided the statistical analysis of this trial.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Ontario Thoracic Society, Physiotherapy Research Foundation and La Trobe Sports, Exercise and Medicine grants.
Data availability statement
Data will be made available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.