
Abstract
Background
Noninvasive mechanical ventilation (NIV) is recommended as the initial mode of ventilation to treat acute respiratory failure in patients with AECOPD. The Noninvasive Ventilation Outcomes (NIVO) score has been proposed to evaluate the prognosis in patients with AECOPD requiring assisted NIV. However, it is not validated in Chinese patients.
Methods
We used data from the MAGNET AECOPD Registry study, which is a prospective, noninterventional, multicenter, real-world study conducted between September 2017 and July 2021 in China. Data for the potential risk factors of mortality were collected and the NIVO score was calculated, and the in-hospital mortality was evaluated using the NIVO risk score.
Results
A total of 1164 patients were included in the study, and 57 patients (4.9%) died during their hospital stay. Multiple logistic regression analysis revealed that age ≥75 years, DBP <60 mmHg, Glasgow Coma Scale ≤14, anemia and BUN >7 mmol/L were independent predictors of in-hospital mortality. The in-hospital mortality was associated with an increase in the risk level of NIVO score and the difference was statistically significant (p < .001). The NIVO risk score showed an acceptable accuracy for predicting the in-hospital mortality in AECOPD requiring assisted NIV (AUC: 0.657, 95% CI: 0.584-0.729, p < .001).
Conclusion
Our findings identified predictors of mortality in patients with AECOPD receiving NIV, providing useful information to identify severe patients and guide the management of AECOPD. The NIVO score showed an acceptable predictive value for AECOPD receiving NIV in Chinese patients, and additional studies are needed to develop and validate predictive scores based on specific populations.
Keywords
Introduction
Acute exacerbations of COPD (AECOPD) is the third leading cause of death worldwide and brings significant economic and social burden. 1 Given that patients with AECOPD may experience hypoxia and hypercapnic respiratory failure, there is a strong need to provide respiratory support to improve oxygenation and acute respiratory acidosis. 2 Noninvasive mechanical ventilation (NIV) can decrease work of breathing and improve breathing co‐ordination, which is recommended as the initial mode of ventilation to treat acute respiratory failure in patients with AECOPD.3,4 Evidence clearly demonstrates that NIV is associated with lower risk of mortality, decreased risk of intubation, prolonged the time to readmission, and fewer complications.5–7
Several risk factors independently associated with in-hospital mortality have been identified in patients with AECOPD, including older age, comorbidities, cardiac dysfunction, blood eosinophils and blood urea nitrogen (BUN).8–12 However, few studies have specifically aimed at exploring the independent prognostic factors among inpatients with AECOPD requiring assisted NIV. In a multicenter study, extended Medical Research Council Dyspnoea (eMRCD) score, time from admission to acidaemia, pH, presence of atrial fibrillation, Glasgow coma scale and chest radiograph consolidation were found to be associated with in-hospital mortality, and a simple scoring system- Noninvasive Ventilation Outcomes (NIVO) score had been proposed to evaluate the poor prognosis in AECOPD requiring assisted NIV. 13 Although NIVO score allows for accurate risk stratification of patients admitted to hospital with AECOPD who required assisted NIV, it was conducted in non-Asian populations. Given the regional and ethnic differences, validation of the NIVO score in Chinese patients is warranted for clinical practice in China.
The specific objectives of the present study are to: (1) determine the risk factors affecting all cause in-hospital mortality in patients with AECOPD requiring assisted NIV, and (2) preliminarily assess the discriminate capacity of NIVO score in a prospective multicenter cohort study in China.
Methods
Study design and subjects
The MAGNET AECOPD (MAnaGement aNd advErse ouTcomes in inpatients with acute exacerbation of COPD) Registry study (ClinicalTrials.gov identifier: ChiCTR2100044625) was a prospective, noninterventional, multicenter cohort study enrolling consecutive inpatients with AECOPD among 10 tertiary hospitals in China between September 2017 and July 2021. The major aims of this registry study were to investigate the management and adverse outcomes of inpatients with AECOPD, and to establish and validate the early warning models of these adverse outcomes. The research results of the MAGNET AECOPD Registry study have been published previously.14–17 In the present study, inclusion criteria: (1) AECOPD as primary diagnosis; (2) pre-admission spirometry evidence of airflow obstruction (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) < 0.7); (3) acute hypercapnic respiratory failure (pH < 7.35 or partial pressure of carbon dioxide (PaCO2) > 45 mmHg) treated with assisted NIV. Exclusion criteria were patients without acute hypercapnic respiratory failure and data missed. No additional direct intervention was performed. The study protocol was approved by the institutional review boards of West China Hospital of Sichuan University (20191056). Written informed consent was obtained from all patients.
Data collection and NIVO score
A standardized case report form was completed for every enrolled patient, including demographic characteristics, comorbidities, vital signs, routine blood tests, biochemical tests, arterial blood gases and radiographic findings. Demographic characteristic included age, gender, body mass index (BMI) and smoking status. Comorbidities recorded were: hypertension, coronary heart disease (CHD) and chronic heart failure (CHF), atrial fibrillation, diabetes, chronic kidney disease, interstitial lung disease, pulmonary heart disease, and cancer. Details of comorbidities were obtained from the clinical records. Vital signs were recorded on admission: systolic blood pressure, diastolic blood pressure, heart rate, and Glasgow Coma Scale. We assessed the Medical Research Council dyspnoea scale (MRCD) instead of eMRCD for the COPD patients in stable condition, patients with MRCD 5 who require long-term bed rest were defined as eMRCD 5b and the rest were defined as eMRCD 5a. Blood tests included hemoglobin and white cell count, platelet count, eosinophil ratio (EOSR%), C reactive protein, albumin, D-dimers, N-terminal pro-brain natriuretic peptide (NT-pro BNP), BUN and uric acid. Arterial blood gas data and time to acidaemia were also recorded. Radiologic findings included consolidation and pleural effusion detected by chest radiograph or computed tomography (CT).
Six risk factors used to calculate the NIVO score were captured from the date of admission, and the individual scores of each risk factor were summed to generate a cumulative risk score that defined the patient’s risk level: low risk (score 0-2), medium risk (score 3–4), high risk (score 5–6), and very high risk (score 7-9). The NIVO score and risk category were calculated by two study operators who received in-depth training to ensure data reliability. The disagreements were resolved by consensus or by consultation with a third assessor.
Study outcomes
The primary outcome was all cause in-hospital mortality after receiving NIV. The secondary outcomes included invasive mechanical ventilation and ICU admission during hospital stay. All clinical outcomes were adjudicated by the independent clinical event committee composed of three experienced physicians.
Statistical analysis
Categorical variables are presented as frequencies and percentages, and continuous variables are expressed as mean ± standard deviation or median and interquartile range. The independent Student’s t test was used to assess differences between continuous variables and the Mann–Whitney U test was used for data that were not normally distributed. The chi-squared test was used to analyze categorical variables.
Logistic regression analysis was performed to identify the predictors of in-hospital mortality in patients with AECOPD requiring assisted NIV, and odds ratio (OR) with 95% confidence interval (95% CI) was calculated to assess the discriminatory power of these parameters. The in-hospital mortality in inpatients enrolled in the study with different risk levels by the NIVO score was compared using the chi-square test. We estimated the discriminative power of NIVO score in predicting the in-hospital overall mortality by calculating the area under the ROC curve (AUC) and 95% confidence intervals (CIs). All data were analyzed by using SPSS 25.0 (IBM, NY, USA), and p-values <0.05 were considered statistically significant.
Results
Study population
Between September 2017 and July 2021, a total of 14007 patients admitted for AECOPD were enrolled in the MAGNET AECOPD Registry study registration study. 2811 patients requiring assisted NIV were initially screened for inclusion in this study, of which 1647 patients were excluded because of the following reasons: (1) patients without acute hypercapnic respiratory failure (n = 1578); (2) data missed (n = 69). Ultimately, 1164 patients were enrolled in the final analysis, 57 patients (4.9%) died during their hospital stay, 23 patients (2.0%) discharged against medical advice, and 1084 patients (93.1%) were discharged after showing improvement (Figure 1). Flow chart of the study (Abbreviations: AECOPD = Acute exacerbation of chronic obstructive pulmonary disease).
Clinical characteristics of the study population
Characteristics of the AECOPD patients requiring assisted noninvasive ventilation.

Data are presented as the number of patients (%); mean ± standard deviation; median (interquartile range).
Abbreviations: AECOPD = acute exacerbation of chronic obstructive pulmonary disease; BMI = body mass index; eMRCD = extended Medical Research Council Dyspnoea; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate; Hb = hemoglobin; WBC = white blood cell; EOSR = eosinophil ratio; CRP = C-reactive protein; NT-pro BNP = N-terminal pro-brain natriuretic peptide; BUN = blood urea nitrogen; ICU = intensive care unit; LOS = length of stay.
Note: Anemia: hemoglobin is less than 12 g/L in females and hemoglobin is less than 13 g/L in males.
Independent risk factors for in-hospital mortality
Multivariate analysis for predictors of in-hospital mortality in AECOPD requiring assisted noninvasive ventilation.

Abbreviations: AECOPD = acute exacerbation of chronic obstructive pulmonary disease; DBP = diastolic blood pressure; BUN = blood urea nitrogen.
Note: Anemia: hemoglobin is less than 12 g/L in females and hemoglobin is less than 13 g/L in males.
Validation of the NIVO risk score
Risk factors of NIVO score in AECOPD patients.
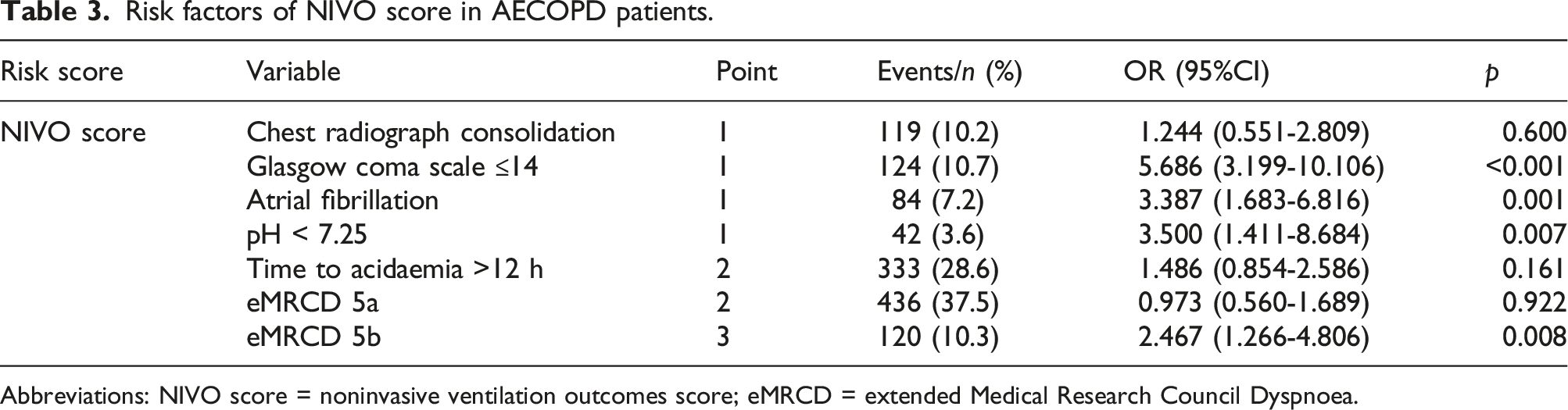
Abbreviations: NIVO score = noninvasive ventilation outcomes score; eMRCD = extended Medical Research Council Dyspnoea.
Association between in-hospital mortality of AECOPD and risk levels of NIVO score.

Abbreviations: AECOPD = acute exacerbation of chronic obstructive pulmonary disease; NIVO score = noninvasive ventilation outcomes score.

The in-hospital mortality by risk levels of NIVO score (Abbreviations: NIVO score = noninvasive ventilation outcomes score).
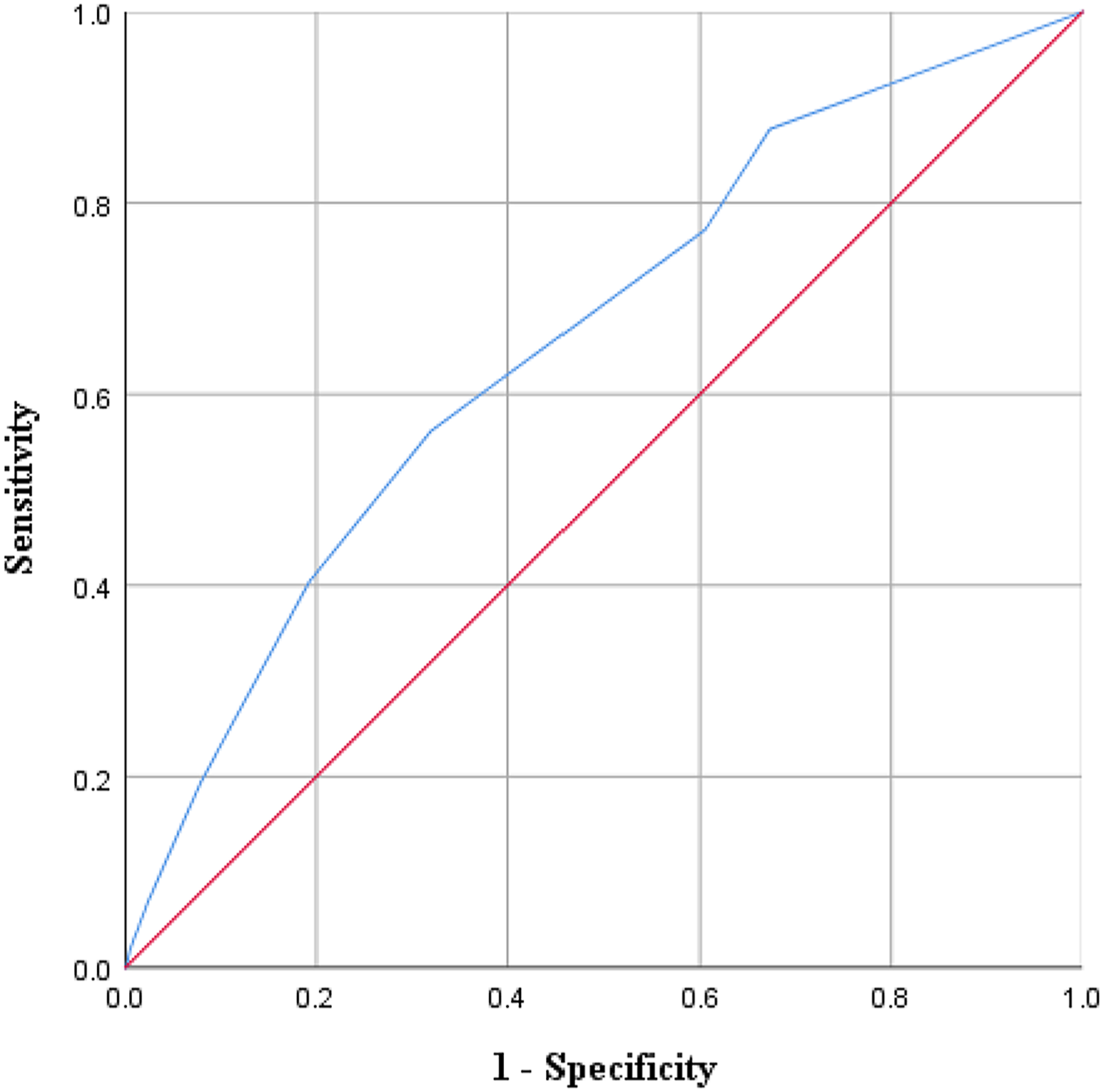
Receiver operating characteristic (ROC) curve of the NIVO score. (Abbreviations: NIVO score = noninvasive ventilation outcomes score).
Discussion
Acute hypercapnic respiratory failure is recognized as a very severe condition, with associated mortality as high as 20%–25% in AECOPD patients. 13 The use of NIV is preferred as the initial mode of ventilation to treat acute respiratory failure in patients hospitalized for AECOPD and showed a success rate of 80%–85%,18–20 However, which variables could predict poor outcomes in AECOPD patients after receiving NIV remained to be elucidated. In this study, we explored factors contributed to a higher in-hospital mortality in a prospective multicenter cohort of 1164 AECOPD patients requiring assisted NIV. The results showed age ≥75 years, DBP <60 mmHg, Glasgow Coma Scale ≤14, anemia and BUN >7 mmol/L were associated with higher odds of all cause in-hospital mortality.
Our findings suggest that five different factors can affect outcome in patients with AECOPD after requiring assisted NIV. The first factor is advanced age, possibly reflecting diminished functional reserve or immune system senescence, supporting the findings of a previous study in patients with AECOPD in Spain. 8 A meta-analysis including 189,772 study subjects also found that advanced age weas significantly associated with increased short-term mortality in patients with AECOPD. 21 The second factor, lower DBP, is an explicit and independent risk factor for the development of cardiovascular diseases.22,23 Myocardial hypoperfusion and damage could be caused by a lower DBP because of the fact that 85% of left ventricular perfusion occurs during diastole. 16 James et al. found that a ‘U-shaped’ relationship between DBP and all-cause mortality and cardiovascular events exists in patients with COPD and heightened cardiovascular risk, in which in reference to DBP within 80∼90 mmHg, lower or higher DBP were both significantly associated with a higher risk of death in the follow-up period. 24 The third factor, Glasgow Coma Scale ≤14, reflect physiological derangement and are frequently included in ICU-specific severity scores. 25 A low Glasgow Coma Scale score could exacerbate CO2 retention and oxygen deficiency, which has been associated with increased mortality in ICU-admitted AECOPD patients. 26 The fourth possible factor is anemia. Anemic COPD patients could increase hypoxic changes, and prolong systemic inflammatory response. 27 In a study by Martinez-Rivera et al, the prevalence of anemia was 33%, multivariate analysis showed that anemia was an independent predictor of mortality in patients hospitalized for AECOPD. 28 Putcha et al. showed that AECOPD with anemia had a significantly higher burden of cardiac and metabolic comorbidities, worse exercise capacity, greater dyspnea, and greater disease severity compared with those without anemia. 29 The results of the present study were consistent with previous studies. This finding is not surprising: typically, anemia should be used as an important variable in future scoring systems for AECOPD. BUN >7 mmol/L is the fifth risk factor for in-hospital mortality in patients AECOPD requiring assisted NIV. An association between BUN and increased mortality in AECOPD has been reported in several studies.17,30 The probable reasons for this association were activation of the sympathetic nerve systems and renal dysfunction. 17
In 2021, Hartley et al proposed a noninvasive ventilation outcomes risk score by incorporating a combination of eMRCD scale, atrial fibrillation, PH, time to acidaemia, Glasgow Coma Scale and chest radiograph consolidation, and verified its predictive value in a 10-centre western population of AECOPD patients requiring assisted ventilation. 13 However, it is not validated in an Asian cohort. In this study, we validate this risk score in a Chinese cohort of patients with AECOPD receiving NIV and confirmed its value in predicting adverse outcomes. In this very large cohort of prospectively enrolled patients with AECOPD having relatively high NIV occurrence, the increases in the risk level were accompanied by increases in the in-hospital mortality for NIVO score, which suggested that NIVO score can stratify the mortality risk in inpatients with AECOPD receiving NIV effectively. However, the NIVO Score in our study showed moderate discrimination (AUC 0.657, 95% CI: 0.584–0.729), comparable to that observed in the western multiple-center validation cohort (AUC 0.79, 95% CI 0.75–0.83). Male bias may be one of the reasons for the differences, the percentage of males in our study was 74.5%, much higher than that of Hartley et al. There are sex differences in clinical characteristics, treatments and outcomes of COPD, which may affect the predictive accuracy of NIVO score. In addition, we noted that the NIVO score, unlike our study, used the treating clinicians’ interpretation of the radiology findings, not the report of a radiologist. The treating clinician was the one who defined the treatment plan (not the radiologist), so their actions changed the outcome of the patient. Radiology reports were often time delayed and therefore not always available contemporaneously. Considering the only moderate performance of NIVO score, its clinical implementation may be of limited usefulness for the clinician. Further improvement is necessary, possibly by adding additional biomarkers such as diastolic blood pressure, anemia and blood urea nitrogen.
To our knowledge this is the first large-scale multicenter study that assessed risk factors for in-hospital mortality in patients with AECOPD receiving NIV and discriminated capacity of NIVO score in patients with AECOPD in China. The prospective and consecutive inclusion of unselected inpatients with AECOPD in our study ensured high data quality, and comprehensive information, including baseline demographics, comorbidities and laboratory tests, were probed into prognostic analysis. These results, therefore, reflect true associations in the real-world setting. Nevertheless, our study has several limitations. First, because patients with AECOPD generally have poor breathing status and cannot afford the pulmonary function test, and related data from stable stage were missing for many patients, thus, parameters of pulmonary function were not included into our analysis. Second, this is a post-hoc secondary analysis of data from the MAGNET AECOPD Registry study, the differences in the definition of eMRCD may affect the accuracy of NIVO score. So the results should be interpreted with caution and deserve to be verified in future prospective studies. Third, the lack of follow-up data prevented us from further evaluating the risk factors with long-term outcome of AECOPD patients receiving NIV. Fourth, we did not analyze the impact of coronavirus disease 2019 (COVID-19) pandemic on excess mortality in patients with AECOPD. COVID-19 has no large-scale epidemic in China under strict epidemic prevention and control measures during the study period. Additionally, COVID-19 patients were admitted to designated hospitals rather than research centers involved in this study. Therefore, the outbreak of COVID-19 has little impact on the outcomes of this study.
Conclusion
In this large cohort study, our findings identified predictors of in-hospital mortality in patients with AECOPD receiving NIV, providing useful information to improve understanding of disease severity and support the decision-making process. The NIVO score showed an acceptable predictive value for AECOPD receiving NIV in Chinese patients, additional studies aiming to develop and validate predictive scores based on specific populations is needed.
Footnotes
Author contributions
Jiarui Zhang: Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Qun Yi: Conceptualization; Funding acquisition; Supervision; Writing – review & editing
Chen Zhou: Data curation; Methodology; Writing – review & editing.
Yuanming Luo: Data curation; Methodology; Writing – review & editing.
Hailong Wei: Investigation; Resources; Writing – original draft.
Huiqing Ge: Investigation; Resources; Writing – original draft.
Huiguo Liu: Investigation; Software; Writing – original draft.
Jianchu Zhang: Resources; Writing – original draft.
Xianhua Li: Resources; Writing – original draft.
Pinhua Pan: Investigation; Writing – original draft.
Mengqiu Yi: Investigation; Writing – original draft.
Lina Cheng: Investigation; Writing – original draft.
Liang Liu: Investigation; Writing – original raft.
Adila Aili: Investigation; Writing – original draft.
Yu Liu: Investigation; Data curation; Writing – original draft.
Lige Peng: Investigation; Writing – original draft.
Jiaqi Pu: Investigation; Writing – original draft.
Haixia Zhou: Conceptualization; Funding acquisition; Supervision; Writing – original draft; Writing – review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the National Natural Science Foundation of China (82170013), the Sichuan Science and Technology Program (2022YFS0262) and the National Key Research Program of China (2016YFC1304202).
Ethical statement
Data availability statement
The data will be shared on reasonable request to the corresponding author.