
Abstract
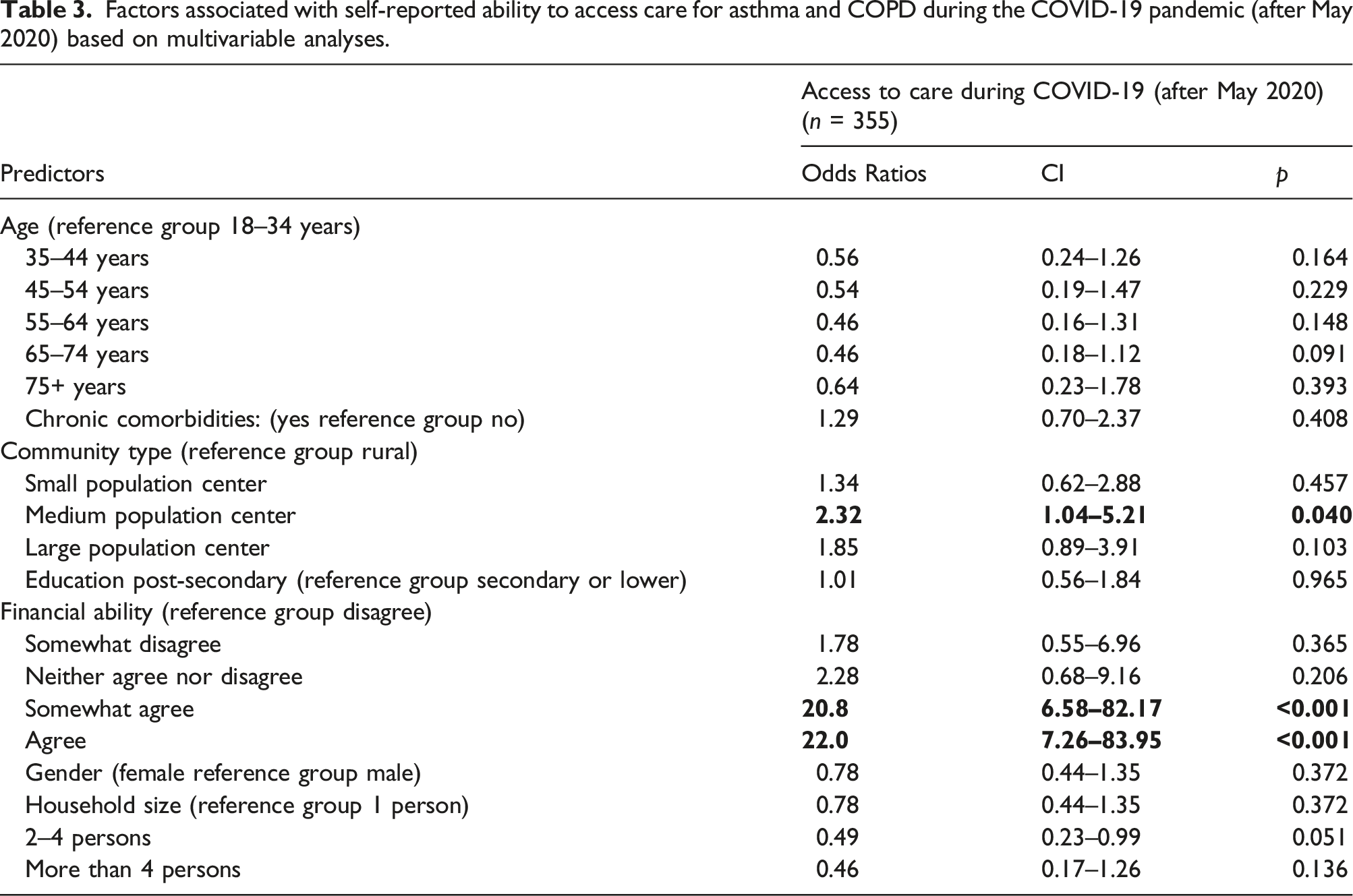
Patients’ perspectives on the impact of the COVID-19 pandemic on their access to asthma and COPD healthcare could inform better, more equitable care delivery. We demonstrate this topic using British Columbia (BC), Canada, where the impact of the pandemic has not been described. We co-designed a cross-sectional survey with patient partners and administered it to a convenience sample of people living with asthma and COPD in BC between September 2020 and March 2021. We aimed to understand how access to healthcare for these conditions was affected during the pandemic. The survey asked respondents to report their characteristics, access to healthcare for asthma and COPD, types of services they found disrupted and telehealth (telephone or video appointment) use during the pandemic. We analysed 433 responses and found that access to healthcare for asthma and COPD was lower during the pandemic than pre-pandemic (p < 0.001). Specialty care services were most frequently reported as disrupted, while primary care, home care and diagnostics were least disrupted. Multivariable logistic regression revealed that access during the pandemic was positively associated with self-assessed financial ability (OR = 22.0, 95% CI: 7.0 – 84.0, p < 0.001, reference is disagreeing with having financial ability) and living in medium-sized urban areas (OR = 2.3, 95% CI: 1.0 – 5.2, p = 0.04, reference is rural areas). These disparities in access should be validated post-pandemic to confirm whether they still persist. They also indicate the continued relevance of exploring approaches for more equitable healthcare.
Keywords
Introduction
Asthma and COPD are the most prevalent chronic respiratory diseases worldwide. They cause exacerbations (lung attacks) that sometimes require hospitalisation and can be fatal.1,2 With support from healthcare providers, patients can self-manage to minimize exacerbations;3,4 but the pandemic disrupted healthcare delivery worldwide. 5
In March 2020, routine care for asthma and COPD was suspended in British Columbia (BC), Canada, 6 where approximately one million people are living with asthma and COPD.7,8 Partial resumption of these services began in May 2020, 9 with telehealth delivery (phone and video) predominating to limit COVID-19 transmission. Such changes could contribute to inequitable access to asthma and COPD care.5,10
The Canada Health Act promotes health equity by legislating that Canadians have reasonable access to medically necessary services. 11 Despite this, access to healthcare varies by socio-demographic (e.g., age, sex, geographic location), socio-economic, and health characteristics,5,12–14 resulting in differential impacts on population subgroups. Patient perspectives on healthcare access can inform improvements towards better care. 15 Patient participation on research teams can elicit more meaningful and relevant results from research and quality improvement initiatives. 16 Still, few studies of how the pandemic impacted access to chronic disease care have included patient partners.
The impact of the COVID-19 pandemic on asthma and COPD care in most of the world, including BC, is currently undescribed. The population level distribution of asthma and COPD patients’ perception of their access to healthcare services when it was partially restored is unknown and it is unclear whether subgroups were disproportionately impacted. We engaged patient partners to co-design a survey about how access to care for these conditions was affected by the pandemic. The primary study objectives were to determine from the patient perspective: 1) whether their access to healthcare for asthma and COPD was reduced after May 2020 when outpatient services (that had briefly been suspended) were partially restored, 2) which specific healthcare services, were disrupted after May 2020, and 3) whether there was differential access to care for different population subgroups after May 2020. We also aimed to describe patient-reported use of asthma and COPD services delivered by telehealth and identify patient characteristics associated with the use of different telehealth modalities. These insights, from the perspective of those seeking care for airways disease, can be applied in healthcare service plans to mitigate negative impacts during future disruptions to care.
Methodology
Study design
We used a patient-oriented research approach to co-design a study that would be acceptable to people living with asthma and COPD and obtain information that could be of interest to patients as well as clinicians and health care decision makers. We used a cross-sectional survey design as described below to understand the distribution of patients’ perspectives on their access to care. The STROBE checklist was used for reporting this observational study. 17
Survey development and administration
A multidisciplinary team of five patient partners with asthma or COPD, three health care providers, and four researchers co-developed a survey to understand patients’ experiences of changes to asthma- and COPD-related care and support during the pandemic. We used guiding principles of inclusiveness, support, mutual respect, and co-building to guide patient engagement. 16 This included communicating individually with team members prior to working meetings to clarify objectives and determine specific supports they may need to meaningfully contribute to the meeting. Post-meeting debriefs were also done individually with each patient partner to confirm understanding, concerns and any further input. We accommodated the sharing of ideas both during the online meetings and afterwards by email or telephone. Where possible, we report patient partner roles using the GRIPP2 checklist for patient and public involvement. 18 We also report the details of the online survey using the CHERRIES checklist. 19 Patient partners led a brainstorming session that identified relevant themes: impacts to healthcare and support; mental and emotional well-being impacts; social impacts; impacts on income, work, education, and potential positive impacts. The study team co-developed questions within each theme. We piloted the survey with a COPD and asthma patient advisory group 20 to ensure clarity, relevance and usability. This group provided feedback during a virtual meeting led by patient partners or via email. The survey had 55 closed-ended questions, some using adaptive questioning. The first page outlined information on study aims and informed consent, which was provided by survey completion. The online version displayed one question per page over 55 screens. Respondents could return to previous sections to revise and complete responses. Where appropriate, “I’m not sure” or “I don’t know” options were provided. Responses were not mandatory with the exception of security questions and a question at the end asking if respondents wished to receive a $10 electronic gift card (determined by our budget) for completing the survey. PB led patient engagement and survey design. Here we report on questions about the impacts of the pandemic on changes to healthcare services and access.
We disseminated the survey through lung health support groups, 21 patient engagement sites,22,23 and respiratory therapists (RTs) at four regional health authorities in BC. To limit conflict of interest, there was no compensation for disseminating the survey. Surveys were completed anonymously online through The University of British Columbia (UBC)-licenced Qualtrics platform (Provo, UT; ubc.qualtrics.com) or via paper (returned in pre-addressed, postage-paid envelopes). We administered the survey from September 2020 to March 2021. We observed a high proportion of bot-completed responses to the online survey which had features enabled in Qualtrics to detect bots and limit multiple completion. We suspended the online survey from December to January to introduce additional security measures namely: enabling Qualtrics RelevantID to identify duplicates (the first entry identified as complete by Qualtrics was used) and fraudulent completion, adding ReCaptcha and items to select the correct month and year to the first page of the survey.
There are no prior measures of patients’ perspectives of their access to asthma and COPD care so sample size calculations were not done. We however aimed for a convenience sample of 500 participants since this was feasible based on our reach. Inclusion criteria were: 18 years of age or older, self-reported doctor-diagnosed asthma or COPD of any duration; currently residing in BC; and ability to communicate in written English. Data were stored on a password protected network and accessed with password protected laptops.
Measures
Survey questions reported here are presented in Table 1 and assessed: 1. Health, socio-demographic and socio-economic characteristics 2. Self-reported access to care before the pandemic (retrospectively ascertained), and following the partial resumption of non-emergent services after May 2020 3. Patient-reported disruptions to specific asthma and COPD healthcare services after May 2020 4. Self-reported use of telehealth for asthma and COPD after May 2020 Survey questions used to determine impact of the COVID-19 pandemic on asthma and COPD care.

Analysis
A description of the analysis of each variable is provided in Table 1. Data from both forms of survey administration were merged to create a single dataset after removing responses that did not meet filtering criteria (see Supplementary Figure 1). All “I don’t know” or “prefer not to answer” responses were treated as missing data and excluded from analyses. Missing data did not exceed 6% for any variable in this report (this rate was observed for self-reported chronic comorbidities only). No weighting techniques were used.
Analyses were performed using R version 4.1.3. Difference in ranks of self-reported access before and during the pandemic was tested using the Wilcoxon signed rank sum test. Bivariate relationships between outcome variables and health and sociodemographic characteristics were assessed using Chi-squared tests. Multivariable logistic regression was used to assess the relationship between covariates and outcome variables. Prior to regression analysis we assessed multicollinearity between independent variables by inspecting their correlation matrix and the variance inflation factor. Age, education, gender, and household size were included as covariates in all multivariable models due to their importance in prior healthcare access and telehealth research. Additional variables were included in multivariable models as covariates if they were significant at the bivariate level (p-value <0.1).
ACF led data analysis, communicated initial findings with the study team via email and led three virtual meetings where patient partners provided insights on emerging findings and suggested further data exploration. This study received Behavioural Research Ethics Board Approval from the University of British Columbia (Certificate no. H20-02287).
Results
Survey completion
12,237 responses were completed online and 49 completed by paper, but only 433 responses met the data cleaning and filtering criteria (Supplementary Figure 1). The average completion time for the survey was 1 h and 15 min.
Description of respondents
Asthma, COPD, and both asthma and COPD were reported by 47%, 33% and 20% of respondents, respectively (Table 1). Respondents lived in communities located in the five health regions of BC, namely Vancouver Coastal (25%), Vancouver Island (25%), Interior (21%), Fraser (18%) and Northern Health region (6%). Most respondents were 35 years and older (80%), attained postsecondary education (67%), lived in population centers 24 with at least 1000 residents or a population density of at least 400 persons per square kilometre (73%), lived in households of two or more people (76%), lived in Canada for over 5 years (80%), and experienced moderate to severe respiratory symptoms in the last 12 months (85%). About half of respondents identified as women (52%), reported no comorbidities (52%), and reported high financial ability during the pandemic (having enough money to meet expenses, 52%).
Change in access to healthcare after May 2020
Self-reported access to care was lower after May 2020, compared to pre-pandemic (p < 0.001). Before the pandemic began, 89% of respondents reported being able to get care for asthma and COPD while 4% reported they could not. After May 2020, 51% of respondents reported being able to get care for asthma and COPD while 30% reported they could not (Figure 1). Self-reported ability to access care for asthma and COPD before and during the COVID-19 pandemic (after May 2020).
Specific services disrupted after May 2020
Respondent characteristics and access to health care.

Differential access for subgroups after May 2020
Factors associated with self-reported ability to access care for asthma and COPD during the COVID-19 pandemic (after May 2020) based on multivariable analyses.
Telehealth after May 2020
Ninety-four percent (403/433) of respondents reported using telehealth services (90% used telephone and 64% used video) for asthma and COPD care during the pandemic. Telephone appointments were mostly used for primary care (75%), followed by specialist appointment (43%), exercise (40%), and education (33%). Video was most frequently reported for exercise (65%), education (52%), primary care (48%), and specialist appointments (40%).
Factors associated with self-reported telehealth use during the COVID-19 pandemic (after May 2020) based on multivariable analyses.

Discussion
Patients’ perspectives are increasingly being considered in healthcare decision-making. 15 This survey of people living with asthma and COPD was conducted during the second wave of the COVID-19 pandemic in BC, when non-emergent asthma and COPD care programs were partially restored with telehealth as the principal mode of delivery (after May 2020). We found that self-reported access to care for asthma and COPD was lower for this period of the pandemic than before, and specialty care services (specialist visits, exercise and education), which are essential to supporting self-management, were most frequently reported as disrupted. A strong disparity in self-reported access was observed after May 2020 in favor of respondents reporting higher self-assessed financial ability. Self-reported telephone use was more common among respondents with moderate to severe respiratory symptoms. Self-reported video use was more common for respondents living in households of >4 persons but was less common among respondents who reported higher financial ability and were older.
Lower self-reported access to healthcare for asthma and COPD during the pandemic is consistent with a high proportion (23%) of British Columbians reporting challenges accessing healthcare during this time 25 and likely reflects the disruptive effects of the pandemic on routine healthcare services. 9
Prior to the COVID-19 pandemic, socio-economic disparities in healthcare access that favored wealthier groups were described in many countries that have publicly funded healthcare,26–28 including in Canada 14 and also the province of BC. 13 These studies examined general healthcare trends rather than asthma and COPD specific healthcare trends, and used administrative data rather than patient perspectives. Our sample population overwhelmingly reported being able to access asthma and COPD care (89%) prior to pandemic and was not large enough to explore disparities in access prior to COVID-19. However when services were partially resumed, an overwhelming disparity in access in favor of respondents with self-assessed financial ability was seen in this same sample population from the user perspective. There are multiple routes by which the pandemic could have had contributed to this. An inability to afford costs associated with commuting to care sites and an inability to take time off work are socio-economic barriers to access to care, even when publicly funded healthcare is available. 29 With reduced earning opportunities during the pandemic, 9 these and other finance-related barriers that are yet to be identified may have become more prominent. With partial resumption of services, availability is more limited. An examination of the plans used to guide service resumption could help to better understand how these disparities emerged. These plans are not publicly available. The existence of the socio-economic-based disparity in access should be validated post-pandemic among a larger, more representative sample. If the disparity still exists, steps should be taken to mitigate against it to prevent it from becoming fixed within the system of care and interfering with the pursuit of health equity goals 30 and reducing health system efficiency.
The COVID-19 pandemic re-ignited calls for reducing health disparities through health equity approaches. These include identifying socio-demographic characteristics associated with disparities, implementing supports to address them, ensuring quality improvement efforts have a focus on equity,5,31 measuring disparities and incentivising their reduction. 32 This study has set the stage for advocating for health equity approaches to asthma and COPD healthcare services in BC, by indicating a potential erosion of equitable access to services based on financial ability during the pandemic and is a basis for more rigorous exploration post-pandemic. It also indicates the importance of assessing for disparities in access to health services for other chronic health conditions and in other jurisdictions, in the post-COVID-19 era.
Implications for telehealth in airways disease care
Our findings from patients’ self-reported use of the rapidly-implemented telehealth services during the pandemic (secondary objective) support previous findings of higher likelihood of telephone use among sicker individuals, 33 higher likelihood of video appointment use among patients living in larger households (4+ members in our study), 34 and lower likelihood of video appointment use among respondents above 64 years. 35 Equity-related observations from the rapid adaptation of telehealth during the COVID-19 pandemic is not extensively reported. It is encouraging that associations based on our patient perspectives is consistent with studies that are from other contexts, populations and that used more conventional data types. We found a previously unreported lower likelihood of video appointment use among respondents with highest financial ability, independent of age. Since financial ability was not associated with a lower need for care (milder symptoms), this finding raises the question of whether this demographic prefers other care modalities. Telehealth could help reduce some challenges with accessing asthma and COPD care services in BC, but guidelines and standards are lacking.36,37 Evaluation of the quality and uptake of the different modalities of telehealth for airways disease care during the pandemic could guide its effective adoption in routine care.
Strengths and limitations
Patient partners participated in all stages of this work. Their involvement ensured that survey questions were relevant and understandable, and also that data analysis and interpretation considered realities of their lived experience. We used self-assessed measures to focus on patient’s perception of their characteristics and abilities. This is exemplified in use of self-assessed ability to meet monthly expenses to measure perception of economic ability instead of self-reported income. Subjective ability to meet expenses has been proven as a valid indicator of economic status and financial ability.38,39
The survey design allowed us to acquire insights from patients across a wide geographic region while minimizing the burden on patients to contribute their insights during the stressful time of the COVID-19 pandemic. Interview or focus groups could be used in follow-up studies to understand specific ways in which financial ability during COVID-19 drove the observed disparity in access to asthma and COPD care in BC. Such an understanding could be useful for limiting inequitable service delivery in the future.
The average survey completion time was five times that anticipated based on our pilot and may be indicating that the patient advisory group that piloted the survey is not adequately representative of the target population. The administration of our survey through an anonymous link online prevented us from ascertaining the true response rate. Perhaps reflective of respiratory therapists informing patients about the survey, we had a convenience sample of mostly telehealth users that accessed care during the pandemic, with representation from communities within all health regions of BC. Sociodemographic-related patterns of healthcare access may not be representative of the asthma and COPD population in BC and are likely different among those who never accessed healthcare during the pandemic. This is a cross-sectional study so we do not know if the observed perception of access and the associated relationships persist beyond the study period. Respondent and recall bias may impact our findings since our study used a self-reported survey. Ascertainment bias might have influenced perceptions that specialist visit, exercise and education were more disrupted than diagnostic and home health services which are typically less widely used. Our sample size was relatively small with some estimates having a wide confidence interval. The strength and direction of the relationships identified herein should therefore be confirmed in a larger study. Caution is recommended before generalizing our findings, which are initial insights that may be more influential if validated by further study.
Conclusion
We sought to understand, from people living with asthma and COPD in BC, how their access to asthma and COPD care was impacted after services were partially restored during the COVID-19 pandemic. We found that during this time, patients self-reported lower access to care, which was associated with low self-assessed financial ability, and that specialty care services were seen as most disrupted. It is important to reassess whether this disparity still exists post-pandemic. If it does, consideration of patient characteristics in healthcare quality improvement, and addressing the pathways by which disparities arise, could be part of a health equity approach to restoring routine healthcare services for asthma and COPD in BC.
Supplemental Material
Supplemental Material - Disparities in self-reported healthcare access for airways disease in British Columbia, Canada, during the COVID-19 pandemic. Insights from a survey co-developed with people living with asthma and chronic obstructive pulmonary disease
Supplemental Material for Disparities in self-reported healthcare access for airways disease in British Columbia, Canada, During the COVID-19 pandemic. Insights from a survey Co-Developed with people living with asthma and COPD by Aneisha Collins-Fairclough, Prabjit Barn, AJ Hirsch-Allen, Karen Rideout, Erin M. Shellington, Winnie Lo, Tony Lanier, Jim Johnson, Adam Butcher, Sian-Hoe Cheong, Carmen Rempel, Nardia Strydom, Pat G. Camp, Chris Carlsten in Chronic Respiratory Disease
Footnotes
Author’s Note
Pat Camp is an Editorial Board Member Twitter summary: We asked people living with asthma and COPD in BC how the COVID-19 pandemic affected their access to healthcare services. Their responses told us that disparities in healthcare access emerged during that time and was associated with economic ability. People who reported having low ability to meet their monthly expenses were more likely to report lower access to asthma and COPD care when services were partially restored during the COVID-19 pandemic. It is important to reassess whether this disparity still exists post-pandemic to mitigate against this inequity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.