
Abstract
Objective
To determine availability and characteristics of pulmonary rehabilitation programs performed in 2019 in family health centers and hospitals from Chile.
Methodology:
A descriptive and retrospective study was designed, considering PR programs operated in 2019. A non-probability and convenience sample was obtained. Availability and characteristics of centers and PR were measured using a questionnaire translated, modified, validated, and sent by email.
Results
Out of 80 responses (22.8%), 60% of centers offered PR program, where the lack of time was the greatest barrier. The programs were mainly outpatient, non-personalized, with 10(IQR 4–11) participants, 12 (IQR 12–16) weeks of length, with 2.4 ± 0.6 session/week, and 1 (IQR 1–2) hours/session. Chronic Obstructive Pulmonary Disease (COPD) was the most frequent diagnostic. The programs were mainly comprised of strength training exercises of lower extremity, upper extremity, walking and education. Team was constituted of physiotherapist and physician, with completed training, and directed by a physiotherapist. Modified Borg, MRC dyspnea scale, six-minute walking test and oximetry were used in the assessments. Between 40-80% of patients completed PR, and the major barrier was patient relocated.
Conclusion
Increasing PR availability, homogenization of exercises and education, prioritization of assessments supported by scientific evidence, and inclusion of follow-up could be useful to improve the access, quality and results of the treatment, considering new models of PR that allow greater access and acceptability.
Introduction
PR is defined as a “comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include, but are not limited to, exercise training, education, and behavior change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors”. 1 This intervention represents a central component of therapeutic strategies in chronic respiratory diseases because it is clinically effective, and allows the intervention of pulmonary and systemic manifestations.2,3 In COPD, PR improves maximum and functional capacity of exercise, measured by incremental cycle ergometry test (Workmax (watt)) and six-minute walking test (6MWT), respectively, health status, anxiety and depression, function of peripheral muscles and quality of life related to health.2–4 Additionally, a reduction in percentage of hospital readmissions has been reported in COPD following PR. 5 In asthma, interstitial pulmonary disease and pulmonary transplant, PR improves quality of life and exercise capacity.6–9
In 2013, the American Thoracic Society (ATS) and the European Respiratory society (ERS) defined the increase in accessibility to PR as a challenge. 1 Additionally, PR programs should follow clinical guidelines based on evidence to ensure quality. 10 However, not all the centers offer a PR program,11–13 and the structure, components, team, resources and referrer to PR are heterogeneous among centers.1,10 In terms of program availability, two national studies conducted in the UK and Canada observed that a 40% of centers had PR program,11,13 and 23% of centers had a program in Ontario, Canada. 14 Regarding characteristics and components of programs, although the studies reported structured programs of exercises,11–13 not all the programs included education, reinforcement of adherence to healthy behavior or measurement of multi-dimensional variables,12,15 which are considered as criteria of quality in the programs. 10
In Chile, a previous study performed in only one region, Valparaiso, has characterized the PR programs. This study observed that 28% of centers had implemented a PR program. In addition, programs showed differences compared to other studies, for instance, education or measurement of multi-dimensional variables were not reported by all the centers, supporting the heterogeneity among centers. 16 However, percentage of centers that offer PR in the rest of the country, and characteristics of those programs, including barriers to implement and complete the program, and follow-up, have not been described. Therefore, we aimed to determine availability and characteristics of pulmonary rehabilitation programs implemented in 2019 in family health centers and hospitals from Chile.
Methods
Study design
A quantitative, observational, descriptive and retrospective study was designed following the STROBE guideline, which was approved by 1 year, since October 26, 2020, by Ethics Committee from Universidad de las Américas with the code CEC_FP_2,020,006. All the participants signed informed consent online.
Participants
PR programs from family health centers and hospitals in Chile. A total of 553 programs in Chile were considered, that included 371 centers of family health centers and 182 hospitals, 17 estimating 1 annual program of PR in each center. Inclusion criteria were to be a PR program from any region of Chile and have been started between January 2019 and December 2019, i.e. operated in 2019. Programs from high, medium and low complexity hospitals were considered. Programs of cardiopulmonary rehabilitation or physical activity were excluded.
A non-probability and convenience sample was obtained from a sample frame comprised of family health centers and hospitals, where email from the professional in charge of PR was available, according to definition and characteristics of a sample frame in the literature. 18 In addition, centers and hospitals with unavailable email of professionals but contacted through respiratory health coordinators from Health Services were considered. This strategy sought to increase diffusion and achieve a greater sample frame to reduce bias. To obtain a sample frame, a register with emails of professionals in charge of PR and respiratory health coordinators was made. These emails were acquired as part of this study, by inquiry in the web site of each Health Service, using the link “Solicitud de información, Ley de Transparencia.” This allows to have access to Chilean public data. In total, the sample frame was comprised of 295 contacts of professionals and 56 coordinators.
Recruitment
After obtaining authorization of Ethics Committee from Universidad de las Américas, professionals in charge of PR were contacted by email between March-April 2021 to inform about the study, details of inclusion and exclusion criteria, and to give an online informed consent. Coordinators were contacted also by email, attaching all the data about the study, and they were asked to spread this information among their professionals in charge of PR. Then, after revision of informed consent, a button “I accept” allowed to access to the instrument.
Variables
Variables of the study.

Instrument
Variables were measured using the “Pulmonary Rehabilitation Program” questionnaire, which is the translation, modification and adaptation of “Pulmonary Rehabilitation Program Survey”, 11 performed as part of the current study. The questionnaire was translated by one physiotherapist with experience in PR, native speaker of Spanish, whose second language is English. After that, the questionnaire was validated by six physiotherapists with experience in PR, using open-ended questions to determine its adaptation to Chilean context, comprehension and redaction. The questionnaire was modified according to suggestions from the validators, to obtain a final version. The questionnaire was comprised of 34 multiple choice questions, and it was digitalized using SurveyMonkey® platform, USA.
Data collection
Data was collected between March 2021-April 2021, by the researchers C.N y A.M, from the programs operated in 2019. The questionnaire was sent online, through a link, in two times, separated by 4 weeks. Data was downloaded from platform in xlsx format.
Statistical analysis
Sample size was obtained using a formula to calculate sample to estimate a proportion, with 95% level of confidence, 9% precision, 19 and a proportion of implementation of PR program of 23%. 14 Thus, 73 PR programs was considered as sample size.
Variables were analyzed using descriptive statistics. For quantitative variables, distribution of data was determined by Shapiro-Wilk Test. Parametric variables were descripted using mean and standard deviation, and non-parametric variables were descripted using median and interquartile range (IQR). Categorical variables were descripted by proportions. For all the variables, percentage of missing data was calculated. Software STATA 14.2 (StataCorp, USA) was used for all the analysis.
Results
Proportion of answers. Characteristics of centers and surveyed subjects
Characteristics of centers and surveyed subjects.

PR implementation and barriers for implementation
Forty-eight (60% of respondents and 13.7% of total sent questionnaires) centers had implemented a PR program versus 32 (40%) centers with no implementation. Barriers for PR implementation were lack of time in 14 centers (43.8%), lack of human resources in 11 centers (34.4%), lack of training in 11 centers (34.4%), lack of funding in 10 centers (31.3%), lack of interest of patients in 8 centers (25.0%), and other reason in 12 centers (37.5%).
Type and structure of PR programs
Type of program and personalization.

Percentages calculated for n = 48.
Structure of PR programs by type of program.
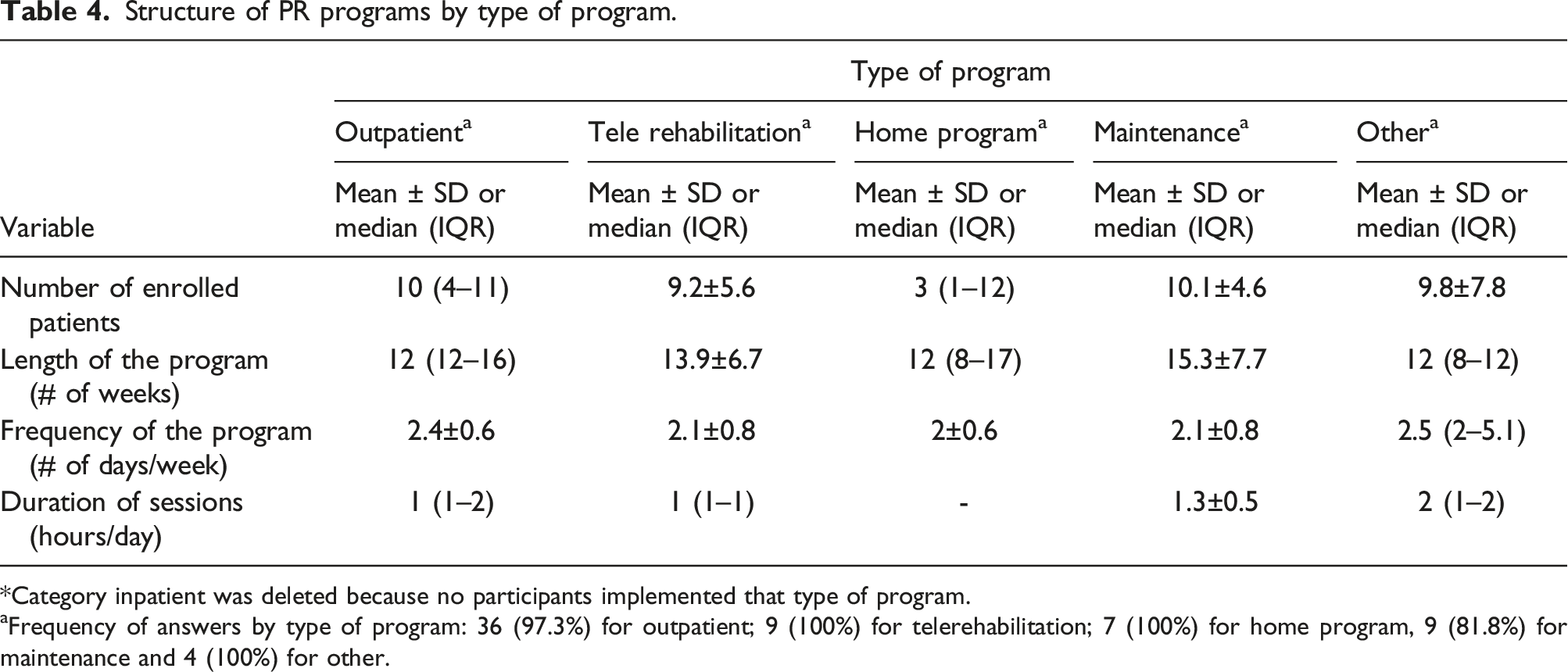
*Category inpatient was deleted because no participants implemented that type of program.
Frequency of answers by type of program: 36 (97.3%) for outpatient; 9 (100%) for telerehabilitation; 7 (100%) for home program, 9 (81.8%) for maintenance and 4 (100%) for other.
Type of patients
The most frequent diagnostic in outpatient, maintenance and other programs was COPD (59–95%). In telerehabilitation, the most frequent diagnostic was restrictive pulmonary disease (50%), and in home program was other (62.5%) (Table S1).
Half of the centers accepted smoker patients (50%). Most of the centers asked for participation in cessation program (66.7%) and monitored cessation of smoking (66.7%) (Table S2).
Components of program
Components of PR by type of program.
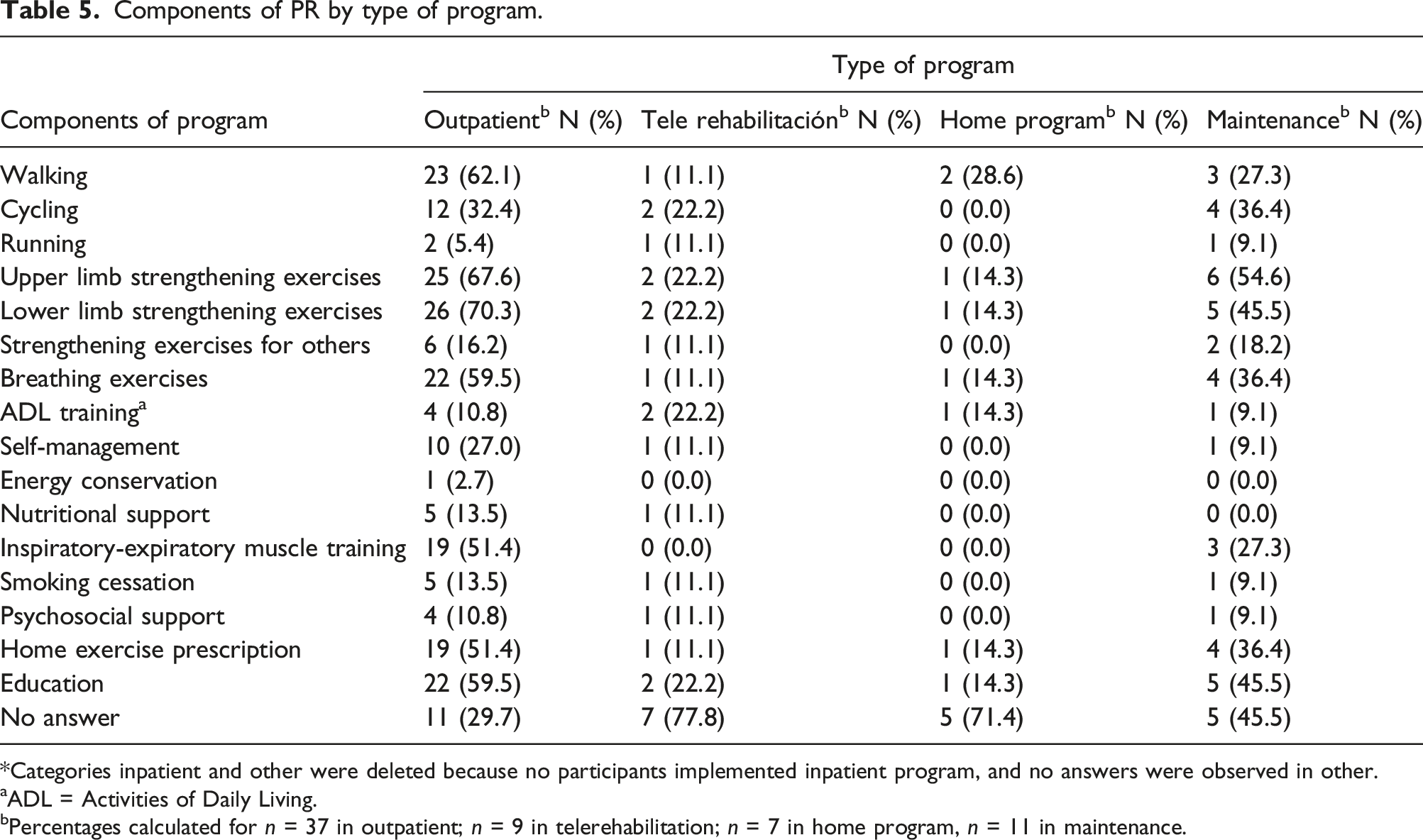
*Categories inpatient and other were deleted because no participants implemented inpatient program, and no answers were observed in other.
aADL = Activities of Daily Living.
bPercentages calculated for n = 37 in outpatient; n = 9 in telerehabilitation; n = 7 in home program, n = 11 in maintenance.
The mainly covered topics in educational sessions were use of inhalers (56.3%) and breathing exercises (52.1%) (Table S3). These educational sessions were mostly performed by group discussion, with 23 centers (47.9%), followed by individual education in 18 centers (37.5%), education using written information in 14 centers (29.2%), and other in 3 centers (6.3%).
Family members were mainly not included in the program, with 16 centers (33.3%), followed by 13 centers (27.1%) where family members were included in PR.
PR program team
The team was mainly constituted of physiotherapist and physician of respiratory diseases program, in outpatient (67.6% y 37.8%, respectively) and maintenance (63.6 years 45.5%, respectively) programs (Table S4).
Thirteen centers (27.1%) had one professional of PR program, at least, enrolled in a PR training, and 21 centers (43.8%) had a professional with completed training, versus 8 centers with no professional enrolled in PR training and 4 centers (8.3%) with no professional with completed training.
Director of PR program in most centers was a physiotherapist (56.3%) (Table S5). Patients were mainly referred by physician of respiratory diseases program, followed by self-referral (25.0%) (Table S5).
Assessments
The most used tests in pre-PR assessment were electrocardiogram (37.8%), spirometry with bronchodilator response (29.7%) and chest radiograph (21.6%) in outpatient program. Furthermore, the tests used in pre and post-PR assessment were modified Borg scale (59.5%), MRC dyspnea scale (59.5%), six-minute walking test (54.1%) and pulse oximetry during exercise (43.2%) in outpatient program (Table S6).
Follow-up
Follow-up was performed in most of centers (39.6%) (Table S7). Frequency of follow-up was mainly every 3 months (57.9%) (Table S7). The most frequent components were reassessment (66.7%) and phone support (44.4%) in outpatient program, and reassessment in maintenance program (60.0%) (Table S8). Barriers to follow-up were lack of time in 20 centers (41.7%), lack of human resources in 19 centers (39.6%), lack of funding in 18 centers (37.5%), lack of patient interest in 11 centers (22.9%), lack of training in follow-up in 5 centers (10.4%), and other in 6 centers (12.5%).
Completion of program
Percentage of patients who complete the program was predominantly between 40-80% (41.7%) (Table S9), and the main barriers to complete the program were transfer of the patient (41.7%), followed by transportation issues (35.4%) (Table S9).
Readmission and waiting list
Most of centers readmits patients once a 12–15-weeks PR program is completed (47.9%) (Table S10). Percentage of readmission is variable: 20–40% (30.4%) and 80–100% (30.4%) (Table S10).
Twenty-four centers (50.0%) reported that they did not have a waiting list to enroll patients in PR versus two centers (6.3%) with waiting list to enroll patients.
Discussion
This study is the first characterization of pre-Covid PR programs in Chile. Percentage of answers was higher than that previously reported, which is 18% in studies with online data collection. 20 Additionally, the answers came from centers located in different regions.
Availability of PR programs was higher than that previously reported (60% versus 40%)11,13,14 and higher than that observed in a previous study performed in a region of Chile (60% versus 28%). 16 In 2013, Chilean Ministry of Health designed a PR protocol for family health care, which could have influenced the offer of PR. Nonetheless, it is not possible to discard a bias, since the administration of the questionnaire was online and volunteer, thus, centers that participated in the study may have been those that fulfill the offer of program. In this regard, the proportion of centers that offered a PR program of total sent questionnaires was 13.7%, however the reasons for not answering the questionnaire are unknown. It is noteworthy that previous studies have used a similar method of data collection.11,13 Even so, there is an important percentage of centers that did not offer program. In this sense, barriers to offer a program in the current study are related to available and trained human resources. Therefore, these barriers require strategies of approach to increase the availability of PR.
Characteristics of PR programs observed in the current study show similarities, compared to published studies, where outpatient program is the most frequent type of program. 11 The structure of programs is also analogous to previous studies, where the intervention group size is 10 participants, the running time is 8–9 weeks, with frequency of 2 days/week, and 2 h/session.11–13 Consistency is observed about the most frequent diagnostic among studies, which is COPD.11,13,14 In addition, centers from published studies mostly accept smokers, 11 as the present study.
Exercise has been reported as the most frequent activity in programs, which is performed in up to 99% of centers.11,13 The most used exercises are endurance exercises, lower limb strengthening with treadmill or bicycle, breathing training and of upper limb strengthening. 11 This is analogous to that observed in the current study, although activities were heterogeneous among the centers. It is important to mention that equipment, such as treadmill or bicycle, is infrequent in Chile.
Programs from published studies are comprised of a multidisciplinary team,11,13 comparable to this study. Most of centers had one professional, at least, who was enrolled in a PR training or had completed training, similar to the evidence. 11 However, this contrasts with the fact that lack of training had been perceived as a barrier to conduct PR. A possible explanation is that, although most of professionals are trained, this is still insufficient. Thus, findings suggest that quality of training could not be sufficient to implement programs in the centers.
Director of program in the current study was mainly a physiotherapist, however, direction of programs varies in other studies. While in a study from the UK the physiotherapist is the coordinator of program, 13 director of program in Canada is a physician, specifically a pulmonologist. 11
PR improves exercise capacity, health status, anxiety and depression, muscle function and quality of life.2–4 In asthma and interstitial lung diseases, effectiveness in quality of life and exercise capacity has been demonstrated.6,7 Thus, studies report that most frequent instruments are 6MWT and quality of life questionnaires.11,13 However, the present study observed that the most commonly used pre and post-PR tests were dyspnea scales, 6MWT and pulse oximetry. Although 6MWT was used in the centers, this was not the most frequent test, and assessments related to health status, psychological variables, and quality of life were not widely used. Therefore, functional variables and assessments related to quality of life, with evidence of improvement in lung diseases, should be prioritized.
The current definition of PR is based on patient-tailored therapies, 1 however more than one third of programs offered non-personalized PR. In this regard, a key aspect to guide a personalized therapy is the comprehensive patient assessment. 21 The low frequency of centers using multidimensional evaluation could limit the design of personalized PR. Although these programs were non-personalized, there are scarce evidence to determine the best personalized model of PR, and a small number of alternative models. Therefore, programs in the current study should be considered PR, however multidimensional assessments, and search of suitable models for different patients are needed.
Promotion of long-term adherence to healthy behavior is included in the definition of PR. Additionally, development of strategies to extend the effects of rehabilitation has been indicated as an important goal. 1 In this sense, 70–82% of centers in published studies perform follow-up.11,13 This contrasts with the results of the current study, where the proportion of centers with follow-up after rehabilitation was 40%. Therefore, inclusion of follow-up strategies is needed, where the definition of strategies is an area for future research. This would contribute to adherence to healthy behavior and maintenance of the PR effects.
Percentage of completion of PR program currently observed is analogous to that previously reported.4,11,22 In addition, a quarter of the centers said that, at most, 60% of patients completed PR. Thus, an important percentage of patients could not be benefited with the started treatment. Barriers to complete the treatment are associated to transfer and transportation, which is analogous to previous studies where the barriers are related to travel and transport. 23 Therefore, considering the proportion of centers with implemendted PR, and the percentage of completion, the development and investigation of new models of PR to make rehabilitation more accessible and acceptable to patients is needed. 10
Limitations of the current study are related with data collection, that was online and volunteer, and may have biased the answers. Nonetheless, this strategy allowed to surveyed centers from different regions of the country. On the other hand, although the contrast between family health centers and hospitals would be interesting, this analysis could not be performed because the answers came predominantly from family health centers. In addition, it is not possible to discard memory bias, because this study considered programs operated in 2019.
In conclusion, this first descriptive study performed in different regions of Chile suggests that increasing PR availability, homogenization of PR components such as exercises and education, prioritization of assessments supported by scientific evidence, and inclusion of strategies of follow-up could be useful to improve the access, quality and results of the treatment. Future studies regarding maintenance programs would be needed, due to its particularities. A challenge to be considered is the development and investigation of new models of PR programs that allow greater access and acceptability.
Supplemental Material
Supplemental Material - Availability and characteristics of pulmonary rehabilitation programs in family health centers and hospitals from Chile: Descriptive, retrospective and multicentric study
Supplemental Material for Availability and characteristics of pulmonary rehabilitation programs in family health centers and hospitals from Chile: Descriptive, retrospective and multicentric study by Andrea Méndez, Carlos Nieto, Gonzalo Hidalgo, and Iván Rodríguez-Núñez in Chronic Respiratory Disease
Footnotes
Acknowledgements
We thank Dr. Dina Brooks for facilitating the questionnaire used in the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant PI202012 from Universidad de las Américas to AM.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.