
Abstract
Pulmonary rehabilitation (PR) is an effective treatment for people with chronic obstructive pulmonary disease (COPD). However, uptake and adherence to rehabilitation is poor and non-adherence is associated with poorer clinical outcomes. This study investigated the factors that might predict an individual completing his/her PR programme. Demographic, physiological and psychological data were collected from routine assessment information. Non-completers (N = 213) who dropped out after initial assessment were compared with completers (N = 438) who attended all 6 weeks of PR programme. Regression analysis indicated that smoking status was the strongest predictor for completing PR programme, that is, ex-smokers were 2.6 times (95% confidence interval (CI) = 1.7–3.9) and those who had never smoked were 2.5 times (95% confidence interval (CI) = 1.1–5.7) more likely to complete in comparison with those who were current smokers. Scoring better on psychological well-being measures (odds ratio = 1.6; 95% CI = 1.2–1.9) was also a strong predictor. The findings suggest the areas that could be addressed to enhance adherence to rehabilitation, for example, targeted interventions for clients who continue to smoke and for those who require support for psychological distress.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is defined as ‘a chronic, slow progressive disorder characterised by airflow obstruction that does not change markedly over several months’. 1 An estimated 3 million people have COPD in the United Kingdom resulting in more than 25,000 deaths per year. 2 Pulmonary rehabilitation (PR) programmes have been shown to be an effective treatment for people with COPD. PR is delivered by multidisciplinary teams and consists of individualised exercise activities and education on how to manage the symptoms of the disease. National guidelines recommend that patients with COPD are invited to attend PR programmes. 2 –4
PR services need to be made as accessible as possible to patients to increase adherence to programme rates. Developing an understanding of why patients are not attending sessions will enable services to develop targeted interventions that encourage attendance and may reduce waiting times. This is of particular importance as approximately 100,000 people are living with COPD in Scotland, with a predicted optimise of 33% in the next 20 years; this will have increasing financial implications for the National Health Service (NHS) as COPD accounts for over 122,000 bed days and 4500 deaths every year, and it has been estimated that the direct cost of COPD to NHS Scotland to be around £100 million per annum. 5 Greater Glasgow and Clyde (GGC) has the largest PR service in Scotland, and this is the first study known to the authors looking at predicting adherence in this population.
Attendance has been found to be influenced by smoking status, degree of breathlessness, frequency of hospital admissions, length of programme and time to travel to the classes. 6 Those who did not participate in the PR programme were more likely to be socially isolated, lack specific social support for COPD, be smokers and be less compliant with other health-care providers. Previous emotional counselling and co-morbid clinical depression were also associated with non-adherence 7 as was perceived pulmonary impairment over actual pulmonary impairment. 8 Based on routinely gathered information from COPD patients, the present study investigated whether the sociodemographic, health and/or psychological profiles of patients who completed the PR programme were different from non-completers. In addition, further analysis was employed to explore whether we can identify factors that predict completion of the PR programme.
Methods
Participants
This was a retrospective analysis of consecutive case notes of patients who attended for an initial assessment with the GGC COPD PR team between August and December 2009. To be accepted for PR programme, participants were required to have a Medical Research Council (MRC) breathlessness grade of 3 or above to be on optimum drug therapy and to be motivated to attend. Exclusion criteria included those who had already completed PR in the previous 2 years; psychiatric, cognitive or locomotive problems that prevented participation in exercise or a group or decompensate heart failure.
PR programme
The PR programme lasts 6 weeks, and individuals are invited to attend two sessions per week lasting 1 hour 30 minutes at 1 of 17 venues across the GGC area.
Data collection
The data included routine information collected during the initial assessment appointment. The assessment process lasts for 1 hour and included three measures:
The Hospital Anxiety and Depression Scale (HADS), a 14-item self-report measure on symptoms of anxiety and depression, was specifically designed to consider issues relevant for use in somatic medical settings. 9
The Chronic Respiratory Questionnaire self-reported (CRQ-SR) is a self-reported measure of dyspnoea (breathlessness), emotional functioning, fatigue and levels of perceived mastery. 10
The Glasgow PR assessment interview provided demographic information, and the results from physical assessments taken from referral information and initial assessment included gender, age, referral source, number of COPD rehabilitation sessions attended, living alone/living with someone, smoking status, smoking pack-years (number of packs smoked per day multiplied by the number of years of smoking), MRC breathlessness grade, Borg score, ratio of forced expiratory volume per second to forced vital capacity (FEV1%; as reported by referring clinician) and lowest arterial oxygen saturation.
Ethics
Advice was sought from the West of Scotland Ethics Team who defined the study as falling within the remit of a service evaluation as it used routinely gathered clinical information and would inform service development. Therefore, it was not considered to require NHS Research Ethics Committee’s approval. The study was registered with GGC Clinical Governance. Permission was granted from the PR team to access and use the previously collected data.
Statistical analysis
Data analysis was performed using Statistical Package for Social Sciences (SPSS) software, Version 21 (v 21; IBM Corporation, Armonk, New York, USA). Comparisons were made between groups (completers versus non-completers) using unpaired Student’s t tests and Mann–Whitney tests on parametric and non-parametric data, respectively. The χ 2 test was used to test the differences in proportions between the two groups. A factor analysis was conducted to address multi-colinearity of potential predictors, and a logistic regression model was developed to independently predict completion of PR from the assessment variables. The value of p < 0.05 was regarded as statistically significant.
Missing data analysis
Due to the retrospective nature of data collection, a missing data analysis was completed. This revealed that large amounts of data were missing from the smoke pack-years (37.7%), FEV1% (29.9%) and the MRC (16.8%) variables. The smoke pack-year details were not rigorously recorded by the assessing clinician; while details for FEV1% and MRC were provided by the referring clinician and were not always available. In addition, the self-report data were missing for 10% of the CRQ and 8% of the HADS questionnaires. It was therefore deemed appropriate to take a multiple imputation approach to the group comparisons and the main regression analysis. Multiple imputations were completed in SPSS v 21 using Markov chain Monte Carlo method with Mersenne twister random number generation to generate five iterations constrained by the original minimum and maximum values of each variable. The pooled results are provided for the regression analysis.
Results
A total of 651 people were offered PR classes with 438 people completing PR and 213 dropping out of treatment after first assessment. Table 1 provides the demographic details collected at interview and recorded in the case notes. Data for all variables were not available for each individual; the number of valid cases for each comparison is therefore provided separately for each variable. Data were assessed for normality. A skewed distribution was evident and therefore non-parametric testing was applied. Three variables differed between the completers and non-completers. Completers were more likely to be older (Mann–Whitney U = 52,405, z = 4.69, p < 0.001); more likely to be referred from a secondary referral source (χ 2 = 6.42, df = 1, p < 0.02) and less likely to be a current smoker (χ 2 = 44.89, df = 2, p < 0.001) in comparison with non-completers. Multiple imputations for missing data found similar results for each comparison.
Sociodemographic variables by group (completers and non-completers).

df: degrees of freedom; U: Mann–Whitney test statistic; z: z score; IQR: interquartile range; χ 2: chi-squared test.
Baseline physical and physiological assessments for both completers and non-completers are shown in Table 2. Data were assessed for normality. A skewed distribution was found so Mann–Whitney comparisons were employed for all variables. No variables differed significantly at initial assessment between groups although there was a trend for the FEV1% score to be higher for the completers (U = 23,551, z = 1.92, p < 0.06). Multiple imputations found that the FEV1% scores were significantly higher in four out of five of the iterations.
Physiological and physical variables by group (completers and non-completers).
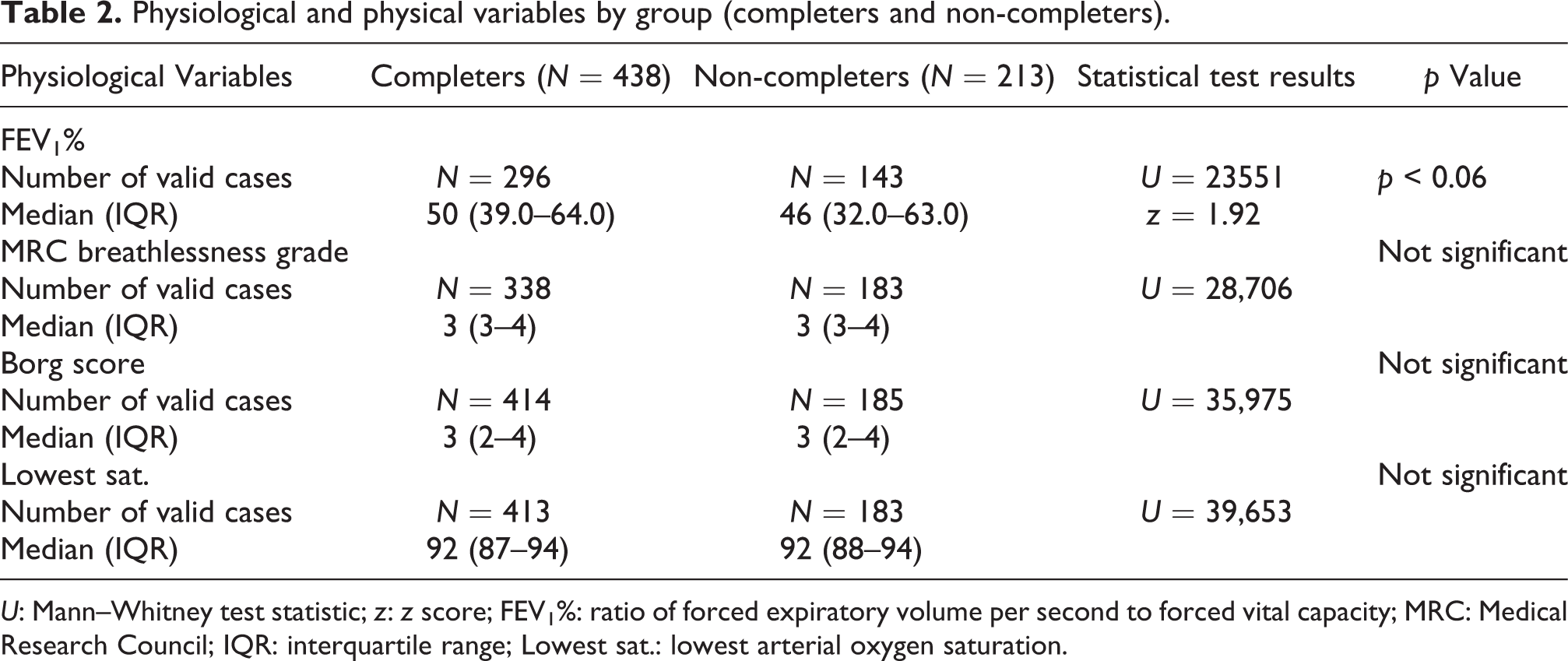
U: Mann–Whitney test statistic; z: z score; FEV1%: ratio of forced expiratory volume per second to forced vital capacity; MRC: Medical Research Council; IQR: interquartile range; Lowest sat.: lowest arterial oxygen saturation.
Scores for the self-report measures at assessment are given in Table 3. With the exception of CRQ emotion, other variables did not meet parametric assumptions. All self-report measures showed significant differences between completers and non-completers. Completers were more likely to have a higher functioning score for dyspnoea ( p < 0.004), fatigue ( p < 0.005), emotion ( p < 0.001) and mastery ( p < 0.001). Completers were also more likely to have lower scores for anxiety ( p < 0.001) and depression ( p < 0.001). Multiple imputations for missing data found similar results for each comparison.
Self-report variables by group (completers and non-completers).

U: Mann–Whitney test statistic; z: z score; t: t test score with degrees of freedom in parenthesis.
CRQ: Chronic Respiratory Questionnaire; HADS: Hospital Anxiety and Depression Scale; IQR: interquartile range; SD: standard deviation.
Predictors of outcome
The variables found to be significantly different between completers and non-completers (age, referral source, smoking status and all the self-report measures) were entered into a logistic regression to identify which of the variables predicted outcome. As several of these variables were found to be strongly correlated with each other, a factor analysis was first completed. All the predictor variables were entered into a principal components analysis with orthogonal rotation (varimax). The initial analysis had a Kaiser–Meyer–Olkin measure of 0.85 which indicates a ‘great’ sampling adequacy. 11 Following the procedure of repeating the analysis after removing all variables with loadings under 0.5 only one component was retained with an eigenvalue of >1 (3.44). The factor loadings after rotation for the five self-report variables that loaded onto this component were CRQ fatigue (0.743), CRQ emotion (0.911), CRQ mastery (0.841), HADS depression (−0.841) and HADS anxiety (−0.784). The factor was named ‘psychological well-being’.
A logistic regression was then completed entering six independent variables (the variables found to be significantly different were age, referral source, smoking status, CRQ dyspnoea and psychological well-being and the FEV1% variable). The pooled results from the missing data multiple imputation analysis are presented. The full model containing all predictors was significant (χ 2(7) = 86.16, n = 625, p < 0.001) indicating that the model was able to distinguish between patients who completed rehabilitation and patients who did not. The model as a whole explained between 13.1% and 18.2% of the variance in completion rates and correctly classified 70.6% of the cases.
Table 4 shows that several of the variables entered into the model were significant predictors of outcome. Smoking status was the strongest predictor: ex-smokers were 2.60 times (95% CI = 1.74–3.88) and those who have never smoked were 2.49 times (95% CI = 1.09–5.70) more likely to complete than those who were current smokers. Scoring better on the psychological well-being measures (odds ratio (OR) = 1.56; 95% CI = 1.24–1.95) was the next strongest predictor of whether an individual attended the PR classes. In addition, those referred from secondary care were more likely to complete than those referred from primary care (OR = 0.64, 95% CI = 0.43–0.96).
Variables predicting the likelihood of completion of the pulmonary rehabilitation programme.a

B: logistic coefficient; SE: standard error of B; Wald: Wald statistic; df: degrees of freedom; OR: odds ratio; FEV1%: ratio of forced expiratory volume per second to forced vital capacity; CRQ: Chronic Respiratory Questionnaire; CI: confidence interval.
aPooled results are shown for the five iterations of the results generated by the multiple imputation method.
bSmoking status: smoker, ex-smoker and never smoked.
Discussion
Analysis of sociodemographic variables showed that completers were more likely to be ex-smokers or to have never smoked, to have been referred from secondary care and to be older than non-completers. On self-report measures, completers recorded significantly higher functioning scores for dyspnoea, fatigue, emotion and mastery and lower scores for anxiety and depression than non-completers. Of the physical assessment measures, FEV1% scores were found to be higher in the completers at initial assessment. In terms of being able to predict adherence from initial assessment information, regression analysis showed that smoking status and psychological well-being were strong predictors of completing PR with referral source also contributing.
Our study reinforces previous research that highlights the role of smoking status in adherence to PR programmes. 8 It has been suggested that patients’ guilt at continuing with smoking or perceived pressure to stop may be contributing factors to non-adherence. 12 All PR programmes encourage smoking cessation, but in a potentially mixed group of smokers and non-smokers, there is little information on what support is actually provided and how PR programmes can meet the challenge of providing effective smoking cessation advice. Encouraging results in terms of quit rates have been achieved by the introduction of a ‘buddy led’ drop in smoking cessation clinic for PR patients immediately before their rehabilitation class. 13 Although this study does not comment specifically on the effect of the ‘buddy’ clinic on adherence to the PR programme, it suggests a way of addressing the specific needs of the COPD smoker and potentially influencing adherence by providing targeted smoking cessation to smokers engaging with PR, which may be more acceptable and motivating for them than general advice given either within the regular PR programme or through smoking cessation for ‘healthy’ smokers. It may be advantageous for existing programmes to consider the funding of specialists trained in health behaviour change to help develop similar clinics in order to prioritise and progress smoking cessation within PR.
The importance of the referring doctor’s attitude and knowledge of PR has been recognised as influencing engagement with PR. 14 Referrers in secondary care may be more knowledgeable in what PR has to offer and be enthusiastic about its potential benefits. Patients attending secondary care may have experienced more difficulty with their COPD symptoms and be more willing to engage in suggested treatments. Those seen within primary care may prefer to be treated by their own doctor or be anxious or unwilling to attend services out with their local surgery. Primary care staff may not feel adequately equipped to answer questions about the PR programme and potential benefits or may have insufficient time to individually assess patient’s health beliefs prior to referral.
Inviting patients to attend information opt-in sessions either led by professionals or with the addition of ‘expert’ patients has been found to be helpful in improving completion rates and reduce drop out by helping address negative beliefs and misconceptions about what PR is and the potential benefits of attending. 15 Patients have also reported a positive effect on self-efficacy and social validation of their condition when expert patients are involved which may merit further investigation within the primary care setting. 16
This study adds to the body of evidence suggesting that psychological well-being, which includes low mood, 17 is an important influence in adherence to PR. This is particularly important given the increased prevalence of depression and anxiety in the COPD population 18 and the link between poor mental health and increased mortality, decreased functional status and decreased quality of life in this population. 19,20 There is difficulty in the identification of anxiety and depression that overlap and are often perceived as solely symptoms of COPD. 21 PR services are still generally under-resourced in terms of being able to offer specialist screening, assessment and treatment of psychological disorders. 22 Previous studies have indicated the potential for a negative impact of generic COPD self-management advice in patients with anxiety and panic disorder; 23,24 therefore, it is important that these conditions are properly assessed and supported within the PR programme to prevent additional distress. Whilst PR programmes are recognised as having a positive impact on anxiety and depression, 25,26 there is a lack of evidence as to which components of PR may be most effective in contributing to this change and how best to address the complexity of psychological needs within PR. 27,28
This study is limited in that it does not examine the potential impact of socio-economic factors. Research has shown that low socio-economic status can negatively affect psychological well-being, 28 and as psychological status appears to be a predictive factor influencing attendance, it would be important to explore this further.
Non-completion and lack of engagement with PR programmes is widely recognised despite evidence supporting their efficacy. It is perhaps unrealistic to assume PR as it stands will effectively meet the needs of all individuals with COPD. In addition to the suggestion that different strategies are needed to enhance programme attendance, 12 and particularly, as certain groups of individuals appear less likely to fully engage with PR, it may be important that different and flexible programme approaches are developed and available to more effectively match diverse patient needs.
Footnotes
Acknowledgements
The authors will like to express their gratitude to Mr William Shankey, Medical Student, University of Glasgow, Scotland, for assistance with data collection.
Conflict of interest
The authors declared no conflicts of interests.
Funding
We would like to thank the NHS Education for Scotland and the Dr Mortimer and Theresa Sackler Foundation for financially supporting this project.