
Abstract
Exertional dyspnea (ED) and impaired exercise performance (EP) are mainly caused by dynamic hyperinflation (DH) in chronic obstructive pulmonary disease (COPD) patients by constraining tidal volume expansion at peak exercise (VTpeak). As VTpeak is the product of inspiratory time (TIpeak) and flow (VT/TIpeak), it was hypothesized that VTpeak and VTpeak/total lung capacity (VTpeak/TLC) may be affected by TIpeak and VT/TIpeak. Hence, the study investigated the (1) effect of TIpeak and VT/TIpeak on VTpeak expansion, (2) factors associated with TIpeak, expiratory time (TEpeak), VT/TIpeak, and VTpeak/TLC, and (3) relationships between VT/TIpeak and VTpeak/TLC with ED and EP in COPD patients and controls. The study enrolled 126 male stable COPD patients and 33 sex-matched controls. At peak exercise, TIpeak was similar in all subjects (COPD versus controls, mean ± SD: 0.78 ± 0.17 s versus 0.81 ± 0.20 s, p = NS), whereas the COPD group had lower VT/TIpeak (1.71 ± 0.49 L/s versus 2.58 ± 0.69 L/s, p < .0001) and thus the COPD group had smaller VTpeak (1.31 ± 0.34 L versus 2.01 ± 0.45 L,p < .0001) and VTpeak/TLC (0.22 ± 0.06 vs 0.33 ± 0.05, p < .0001). TIpeak, TEpeak, and VT/TIpeak were mainly affected by exercise effort, whereas VTpeak/TLC was not. TEpeak, VT/TIpeak, and VTpeak/TLC were inversely changed by impaired lung function. TIpeak was not affected by lung function. Dynamic hyperinflation did not occur in the controls, however, VTpeak/TLC was strongly inversely related to DH (r = −0.79) and moderately to strongly related to lung function, ED, and EP in the COPD group. There was a slightly stronger correlation between VTpeak/TLC with ED and EP than VT/TIpeak in the COPD group (|r| = 0.55–0.56 vs 0.38–0.43). In summary, TIpeak was similar in both groups and the key to understanding how flow affects lung expansion. However, the DH volume effect was more important than the flow effect on ED and EP in the COPD group.
Keywords
Key points
1. Inspiratory time at peak exercise (TIpeak) was related to exercise effort in both the COPD and control groups. TIpeak was not affected by lung function and was similar in all subjects. Thus, tidal volume expansion was flow dependent. TIpeak is the key to understanding that flow is also involved in lung expansion. 2. Expiratory time at peak exercise (TEpeak) and mean tidal inspiratory flow (VT/TIpeak) were also related to exercise effort in the two groups. However, the relationships were reduced by impaired lung function. 3. Tidal volume at peak exercise and total lung capacity ratio (VTpeak/TLC), an inverse marker of dynamic hyperinflation (end-expiratory lung volume/TLC), occurred only in the COPD group and was related to exercise effort. There was a slightly stronger correlation between VTpeak/TLC with exertional dyspnea and exercise performance than VT/TIpeak in the COPD group.
Introduction
Exertional dyspnea (ED) and exercise intolerance in patients with chronic obstructive pulmonary disease (COPD) can be caused by many factors, however it is most likely to be caused by dynamic lung hyperinflation (DH). 1 This has been attributed to the volume effect of DH in constraining the expansion of inspiratory capacity and inspiratory reserve volume (IRV), 2 in which it cannot be overcome by forced expiratory effort. 3 Hence, tidal volume (VT) cannot expand normally. As VT is a product of inspiratory time (TI) and flow (or ventilation) (VT/TI), VT may be affected accordingly.
Inspiratory muscles of COPD patients are usually weak as shown by maximal inspiratory pressure, and they need to make a similar effort to healthy individuals at peak exercise3,4 to meet a given VT. This effort has to be completed within a shortened TI due to a conversely prolonged expiratory time (TE) caused by expiratory flow limitation. In this context, power of the weak inspiratory muscles must be escalated to facilitate tidal inspiratory flow, 5 or a given level of VT cannot be achieved. This scenario is detrimental, as inspiration is more energy consuming than expiration. 6 Therefore, getting air in rather than out too slowly is usually a problem in patients with COPD. In addition, different time constants (τ) of alveolar units due to heterogeneous distribution are critical to ventilation, as they cause a reduction in ventilation even though the static lung volumes are the same. 7 Thus, in addition to the effect of DH on ventilation and symptoms in patients with COPD, TI and VT/TI may also be important factors.
However, TI and TE values have seldom or even not been reported, even though time ratios such as TI and total breathing cycle time ratio (i.e. inspiratory duty cycle, IDC) and TI and TE ratio (I: E) have been reported.2–4,8–14 Given that the ratios at rest and peak exercise are quite different between normal and COPD subjects,2,5,8 they do not reveal TI, and so changes in VT/TI cannot be deduced from these reports.4,8,9,12,14 Nevertheless, most variables of interest have been reported during the expiratory phase, such as τs for alveolar units, spirometry, and expiratory flow limitation during exercise.13,15,16
TIpeak has been shown to have clinical value in patients with COPD before and after lung transplantation. 5 We hypothesized that reduced VT/TIpeak with normal TIpeak in patients with COPD compared to healthy individuals may partially explain the reduced expansion of VTpeak and decreased VTpeak/total lung capacity (VTpeak/TLC). To test this hypothesis, we investigated differences between healthy individuals and patients with COPD at peak exercise in (1) VTpeak expansion affected by TIpeak (time effect) and/or VT/TIpeak (flow effect), and (2) the factors associated with TIpeak, TEpeak, VT/TIpeak, and VTpeak/TLC, and compared (3) the relationships between VT/TIpeak and VTpeak/TLC with ED and exercise performance (EP).
Methods
Study design
This was an observational cross-sectional comparative study. Lung function testing and cardiopulmonary exercise testing were performed. Signed informed consent was obtained from each participant, and the local Institutional Review Board (CS2-21018) approved this study.
Subjects
The study enrolled healthy and COPD subjects from this institution. The inclusion criteria were: (1) age 40–80 years; (2) body mass index 18–30 kg/m2; and (3) male sex. Only male subjects were enrolled because few females have COPD in Taiwan.
Participants with COPD had respiratory symptoms, risk factors and a post-bronchodilator forced expired volume in one second (FEV1)/forced vital capacity (FVC) of < 0.7 and no significant post-bronchodilator effect (increase in FEV1 >12% and 200 mL from baseline) in accordance with the Global Initiative for Chronic Obstructive Lung Disease criteria. 17 All patients were clinically stable for 1 month prior to undergoing the tests. Patients were excluded if they had significant comorbidities including electrolyte imbalance, congestive heart failure, diabetes mellitus or significant chronic diseases or had participated in any physical training program before entry of this study.
Healthy subjects were recruited among the hospital staff and the local community through personal contacts. They were free of known significant acute and chronic diseases and were excluded if they had abnormal lung function, complete blood cell and biochemical tests, chest radiography, or electrocardiography during the screening phase of study.
Protocols and measurements
Pulmonary function testing
FEV1, total lung capacity (TLC), and residual volume (RV) were measured by spirometry and body plethysmography. The best of three technically satisfactory readings was used, where it included acceptable back-extrapolated volume, a sharp peak of expiratory curve which occurred close to the start of expiration, acceptable end of forced expiration (i.e. expiratory time ≥ 6 s or a plateau of expiration curve reached), and reproducibility of the expiratory curve. 18 All lung function data were obtained after inhaling 400 μg of fenoterol HCl. Diffusing capacity of lung for carbon monoxide (DLCO) was measured by the single-breath technique. Maximum inspiratory and expiratory pressures (MIP and MEP) were both performed on three occasions. The best result was recorded for analysis.
Cardiopulmonary exercise testing
After 3-min rest period, each patient began a 3-min period of unloaded cycling followed by a ramp-pattern exercise test to the limit of their tolerance. Work rate was selected at a slope of 5–20 W/min according to pre-determined fitness.
Twelve-lead electrocardiography, heart rate, oxyhemoglobin saturation (SPO2), oxygen uptake (V’O2, ml/min), carbon dioxide output (ml/min), V’E (L/min), breathing frequency (Bf, breath/min), and TI and TE in seconds were measured. The modified Borg scores were obtained every 2 minutes during the loaded exercise. Borg measured at peak exercise was divided by peak V’O2% predicted to scale dyspnea. 19
Maximum exercise is considered achieved by either one of the following: (1) heart rate reserve is 15% or 15 beats/min of predicted maximal heart rate or less; predicted maximum heart rate = 220 – age; (2) respiratory exchange ratio is 1.09 or greater.20,21 Breathing reserve (BR) of < 30%, where BR = 1−V’E/MVV (maximum voluntary ventilation) 22 and a decrease in SPO2 by ≥3% from unloading to peak exercise 23 were also considered to indicate maximal effort, as these criteria indicate that physiological limitations had been reached by the COPD subjects. For comparisons between two groups of subjects during exercise, exercise stage was set at the same level. Thus, the exercise stages were at rest, unloaded, AT if determinate, and peak exercise. Exercise effort was defined as to what extent the level of maximum exercise was achieved at symptom-limited peak exercise, i.e. the higher the exercise effort, the more the maximum exercise criteria or the higher the exercise intensity achieved.
Dynamic inspiratory capacity measurement. 24
Dynamic inspiratory capacity (IC) was measured at the end of a steady-state resting baseline, unloaded cycling, the middle of loaded exercise, and the end of peak exercise. End-expiratory lung volume (EELV) was calculated as TLC minus dynamic IC.
Statistical analysis
The raw data as the file “Supplement data” was uploaded. Data was summarized as mean ± standard deviation. Unpaired-t test or Wilcoxon rank-sum test was used to compare the means or medians of the two sets of data of two patient groups when appropriate. Bivariate relationships were described by Pearson’s correlation coefficients. All statistical analyses were performed using NCSS statistical software. Statistical significance was set at a two-sided p ≤ 0.05.
Results
A total of 126 participants with COPD and 33 normal controls were enrolled after excluding 50 subjects with reasons shown in Figure 1. The COPD group was older and more symptomatic and had poorer lung function (Table 1) and exercise capacity than the controls as expected (Table 2). Flow chart. A total of 209 subjects were assessed for eligibility. 126 subjects with chronic obstructive pulmonary disease (COPD) and 33 healthy subjects were enrolled. All of the participants with COPD had respiratory symptoms, risk factors and a post-bronchodilator forced expired volume in one second (FEV1)/forced vital capacity (FVC) of < 0.7 without a significant post-bronchodilator effect. Healthy subjects were recruited among the hospital staff and the local community through personal contacts. They were free of known significant diseases. A total of 50 subjects were excluded due to the reasons shown. For details about the inclusion and exclusion criteria of the participants, please refer to the text. Demographic, lung function, blood tests, and peak exercise data in the subjects with COPD and normal controls. Abbreviations: CAT, COPD assessment test; DLCO, diffusing capacity of lung for carbon monoxide; EELV: end-expiratory lung volume; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; FRC: functional residual capacity; hs-CRP, high-sensitivity C reactive protein; IC, inspiratory capacity; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; mMRC, modified Medical Research Council; PEFR, peak expiratory flow rate; RV: residual volume; TLC, total lung capacity. Comparison between groups, §using Mann-Whitney U test. NA: not applicable. ‖COPD GOLD 1, n = 10 (7.9%), GOLD 2, n = 71 (56.3%), GOLD 3–4, n = 45 (35.7%). Peak exercise data in the COPD subjects and normal controls. Abbreviations: Bf: breathing frequency; Borg: Borg score; BR: breathing reserve; Δ: change between at peak exercise and baseline; EELV: end-expiratory lung volume; IC, inspiratory capacity; IDC: inspiratory duty cycle; RSBI: rapid shallow breathing index; TI: inspiratory time; TE: expiratory time; TLC, total lung capacity; TTOT: breathing cycle time; V’E: minute ventilation; V’O2, oxygen uptake; VT, tidal volume. Borg/V’O2% indicating Borg measured at peak exercise divided by peak V’O2% predicted; BR indicating 1 – V’E/MVV; EELV/TLC indicating end-expiratory lung volume at peak exercise and TLC ratio; E:I indicating TE and TI ratio; IDC indicating TI and TTOT ratio; VT/TI indicating mean tidal inspiratory flow; VT/TLC indicating tidal volume at peak exercise and TLC ratio.


Comparisons of the COPD group and control group at peak exercise showed that TI was similar (p = NS), TE was greater (p = .01), VT/TI was slower (p < .0001), VT and VT/TLC were smaller (both p < .0001), and EELV/TLC was greater (p < .0001) (Table 2 and Figure 2). When the COPD group was separated into subjects with a resting IC % predicted < 80% and those with a resting IC % predicted ≥ 80%, the former group had higher EELV/TLC (p < .01) and lower VT/TLC (p < .01) and VT/TI (p < .01) at peak exercise (Table 3). Mean values of expiratory time (TE), inspiratory time (TI), tidal volume (VT), tidal inspiratory flow, VT and total lung capacity ratio (VT/TLC), and tidal inspiratory flow (VT/TI) in the healthy individuals (open circles) and subjects with chronic obstructive pulmonary disease (solid circles) in response to incremental exercise at rest, unloaded, anaerobic threshold, and peak exercise. The AT was indeterminate in 29 (23%) COPD subjects. Bars indicate standard deviations. No symbol, p = NS,* ≤0.05, + ≤0.01, # ≤0.001, $ ≤0.0001 for group comparison. The effects of resting inspiratory capacity (IC) on lung expandability and tidal inspiratory flow at peak exercise in the subjects with chronic obstructive pulmonary disease. Abbreviations: EELV/TLC, end-expiratory lung volume at peak exercise and total lung capacity ratio; VT/TLC, tidal volume and TLC ratio; VT/TI, tidal volume and inspiratory time ratio indicating mean tidal inspiratory flow.

Correlation coefficients (r) of inspiratory time (TIpeak) and expiratory time (TEpeak) in seconds at peak exercise with lung function and exercise dyspnea and effort in subjects with COPD and normal controls.

Abbreviations: Bf: breathing frequency; Borg: Borg score; BR: breathing reserve; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; RSBI: rapid shallow breathing index; V’E: minute ventilation; V’O2, oxygen uptake; peak: @ peak exercise; PEFR, peak expiratory flow rate; RBSI: rapid shallow breathing index; VT, tidal volume. % pred: %predicted. r without a symbol alongside indicates that the p value was not significant; || change (Δ) in r compared the normal group to the COPD group; ↓ decrease; ↑ increase; empty: no change; p .05 < ¶ ≤ 0.1, ∗≤0.05, +≤0.01, †≤0.001, ‡ < 0.0001.
Correlation coefficients (r) of mean tidal inspiratory flow at peak exercise (VT/TIpeak) with lung function, exertional dyspnea and exercise effort in subjects with COPD and normal controls.

Abbreviations: Bf: breathing frequency; DLCO: diffusing capacity of lung for carbon monoxide; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; peak: @ peak exercise; PEFR, peak expiratory flow rate; RSBI: rapid shallow breathing index; VT, tidal volume; TI, inspiratory time; V’E: minute ventilation; V’O2, oxygen uptake; % pred: %predicted; VT/TE: tidal expiratory flow. ||: change in r compared the normal group to the COPD group. r without a symbol alongside indicates that the p value was not significant, p .05 < ¶ ≤0.1, ∗≤0.05, +≤0.01, †≤0.001, ‡≤0.0001. VT/TE correlated with VE in the COPD group and the control group, r = 0.97 and 0.98, respectively.
Correlation coefficients (r) of tidal volume at peak exercise and total lung capacity ratio (VTpeak/TLC) — inverse dynamic hyperinflation with the variables of interest in subjects with COPD and normal controls.
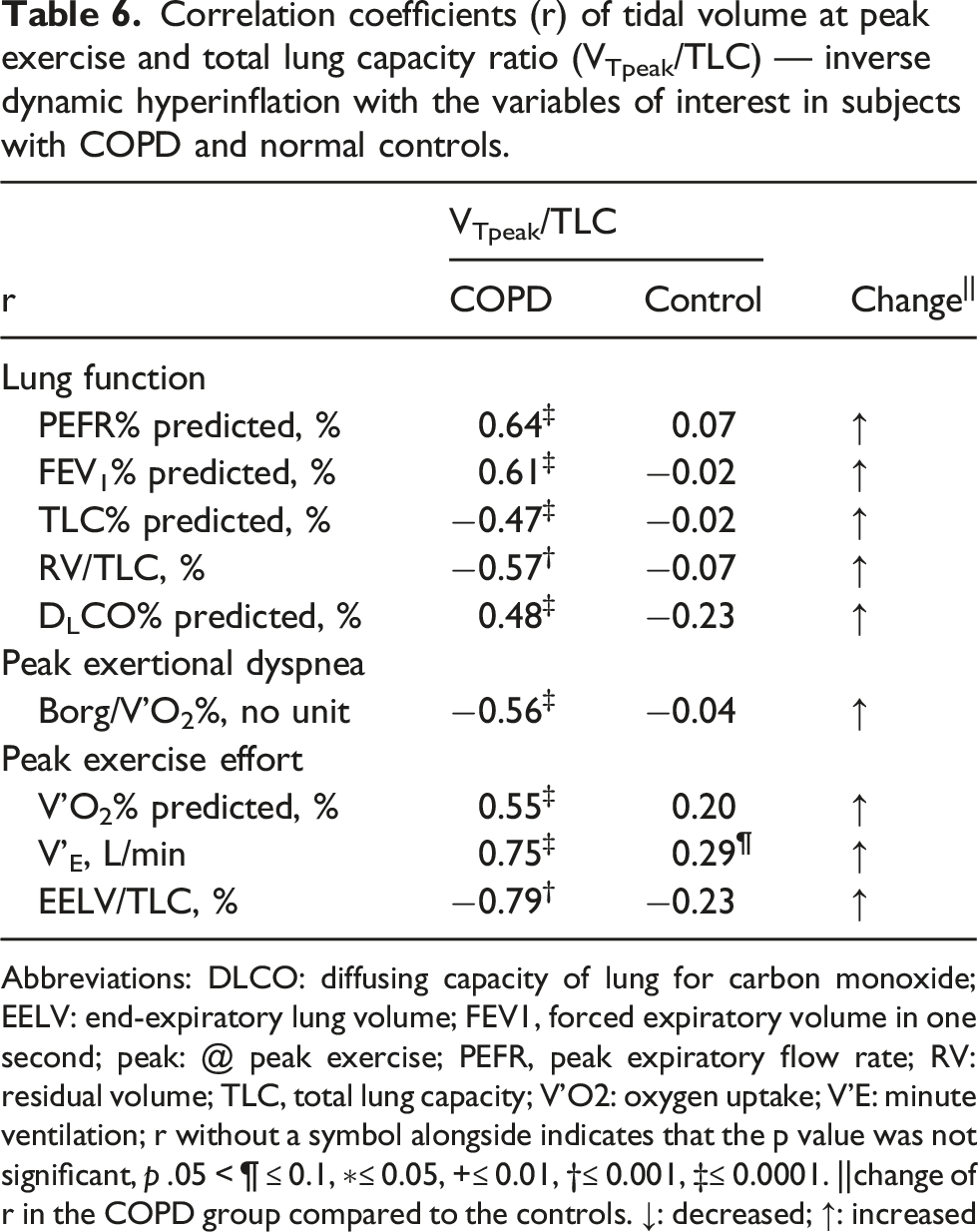
Abbreviations: DLCO: diffusing capacity of lung for carbon monoxide; EELV: end-expiratory lung volume; FEV1, forced expiratory volume in one second; peak: @ peak exercise; PEFR, peak expiratory flow rate; RV: residual volume; TLC, total lung capacity; V’O2: oxygen uptake; V’E: minute ventilation; r without a symbol alongside indicates that the p value was not significant, p .05 < ¶ ≤ 0.1, ∗≤ 0.05, +≤ 0.01, †≤ 0.001, ‡≤ 0.0001. ||change of r in the COPD group compared to the controls. ↓: decreased; ↑: increased
Discussion
The study found that TIpeak was similar in the COPD and control groups, whereas VTpeak and VTpeak/TLC were larger in the control group, suggesting that VT/TIpeak plays a role in lung expansion during exercise (flow effect). Nevertheless, VTpeak/TLC decreased in the COPD group as EELVpeak/TLC increased (volume effect of DH) only in the COPD group. TEpeak, VT/TIpeak and VTpeak/TLC were related to ED and exercise capacity in the COPD group, whereas the associations with VTpeak/TLC were stronger (Tables 4−6). In the control group, VTpeak/TLC was not related to ED or exercise capacity because they did not have DH. The associations of TEpeak, VT/TIpeak, and VTpeak/TLC with lung function were stronger in those whose lung function was impaired. TI, TE, V’O2, V’E, VT/TI, Bf, RSBI, BR%, and VT at peak exercise were exercise effort-related variables in the controls (Tables 4−5); however, the associations were weaker in those whose lung function was impaired.
Volume expansion at peak exercise was related to TI in all subjects, however the correlation was stronger in the controls, in whom VT expandability was not influenced by a reduced flow or DH effect as the healthy individuals were assumed to have normal lung volumes and flow. In contrast, it was more related to flow than TIpeak in the COPD group (Tables 4 and 5, VTpeak correlated with TIpeak, r = 0.27 versus VTpeak/TLC correlated with VT/TIpeak, r = 0.60) due to the deranged lung pathophysiology − the flow effect. All subjects had a similar TIpeak (approximately 0.8 s − the time effect), and thus VT and VTpeak/TLC were smaller in the COPD group (Figure 2). Nevertheless, VTpeak/TLC in the COPD group was also constrained by the elevated EELV/TLC, resulting in a smaller VTpeak/TLC − the volume effect (Table 6, r = −0.79).
Although the prolonged TE caused by expiratory flow limitation may have shortened TI in the COPD group, 5 TI was similar to and Bf was lower than the values in the controls (Figure 2 and Table 2). This is in contrast to a previous study which reported that TI was shorter and Bf was similar. 2 This discrepancy may be because the COPD patients in the previous study had lower FEV1% (37% versus 56.5%) and Bf at peak exercise (30.7 vs 36.4 breaths/min), and because the normal control group contained female participants (40% versus 0%). 2 However, regardless of the difference in TIpeak in the COPD patients between these two studies, VT/TIpeak was even lower, and thus VTpeak was also lower. 2 However, in another study comparing 11 patients with mild COPD and 11 matched normal subjects, TI and VT/TI at peak exercise were similar between the two groups, whereas VT was different. 25 The paradoxical relationships across the three factors raises concerns about a type II error. Therefore, TIpeak and VT/TIpeak can provide additional information to DH with regards to constraining VTpeak expandability in COPD patients, especially for those with moderate to severe COPD. Elevated VD/VT plays a role in patients with mild COPD, as VT/TIpeak can increase and VTpeak compensates to allow normal expansion. 25
Despite the value of TI in pulmonary mechanics, breathing-related times i.e. Bf, TI, TE, total cycle time, I:E ratio, and IDC have seldom been reported together in one study,2–4,8–14 and therefore the underpinning pathophysiology may be overlooked. Hyperoxia improves ED not only by decreasing ventilatory demand and DH, 8 but also by decreasing Bf.8,14 The decrease in Bf may prolong TI, and thus VT would be enlarged even with no change in VT/TI. Other studies on tiotropium and salmeterol have reported that improved VTpeak expansion was attributed to ameliorating DH.9,12,14 However, improvement in VT/TIpeak may also be involved, as Bf was unchanged and hence TIpeak was also probably unchanged, and thus VTpeak was increased.9,12 Another study of patients with severe COPD reported that tiotropium prolonged TI and did not change VT at rest, thereby paradoxically reducing VT/TI. 26 However, during constant exercise, VT/TI was maintained and TI was expected to be prolonged as Bf was slowed, resulting in an expansion of VT. 26 Moreover, changes in ED were correlated with a change in Bf (r = 0.70) but not with a change in IDC (r = 0). 27 As the intensity of exercise increases near heavy exercise (i.e. ≥70% of peak exercise capacity), VT expansion flattens and critical minimal IRV is reached. However, these effects do not stop exercise immediately, and exercise can continue for a few minutes. 28 This has been reported to result in an “alinear” relationship between minimal IRV and ED. At this moment, increasing Bf shortens TI and together with a plateaued VT abruptly increases VT/TI. This indicates that an accelerated VT/TIpeak at the start of minimal IRV underpins the mechanisms of ED. In other studies on breathing patterns in normal male and female subjects with different ages, VT/TI was quite different at different stages of ventilatory stress, however, IDC was not. 29 The standard deviation of IDC was very small (±0.01) in the previous studies of normal subjects and patients with chronic obstructive airway disease.7,26,29 These results echo the value of VT/TI in the mechanisms of ED but not that of IDC (r = 0). 27 In summary, the mechanisms of VT/TIpeak were different in the healthy individuals and COPD subjects. VT/TIpeak was an exercise effort marker in the healthy individuals, whereas VT/TIpeak was a marker of exercise effort, airflow patency, lung expandability, and less dyspnea in the COPD patients. In addition, non-invasive ventilation during exercise had some benefits in the patients with COPD, including unloading work of breathing and overcoming auto-positive end-expiratory pressure. 30 Thus, VT/TIpeak may play a role when assessing the effects of bronchodilators9,12,26 and using non-invasive ventilation.
Volume expansion at peak exercise/TLC has been reported to be an inverse marker of DH, i.e. EELVpeak/TLC in patients with COPD (r = −0.83, p < .0001), 31 which is consistent with our results (Table 6, r = −0.79, p < .0001). However, they were not related in the normal controls because DH did not develop, 31 so that VTpeak/TLC did not play a role in either EP or ED. However, this marker played a role in the COPD group, which is consistent with previous studies.1,2,25 Volume expansion at peak exercise/TLC is a beneficial marker for lung expansion, and thus it was moderately to strongly and positively related to FEV1%, DLCO%, and VT/TIpeak and moderately to strongly and negatively related to TLC%, RV/TLC%, EELVpeak/TLC in this study. Volume expansion at peak exercise/TLC is much easier to obtain than EELV/TLC, which requires IC maneuvers for EELV. However, one concern is that TLC may be underestimated in patients with COPD if dilution and washout techniques are used to assess functional residual capacity (FRC). 32 In this study, FRC was measured with body plethysmography, so that TLC would not be underestimated or overestimated when the subjects panted at a rate < 60/min. 32
Lastly, resting IC < 80% predicted may be a marker of lower lung expandability, tidal inspiratory flow, and higher dynamic hyperinflation (DH) (Table 3).
Study limitations
The number of cases was still small in this study despite being larger than those in previous studies. In addition, female subjects were excluded from this study, and further studies are warranted to investigate any sex-related differences. The inclusion criterion for age was 40–80 years. Because of the wide range of ages, the age of the study group was higher than the controls. In addition, although MIP and MEP were not measured in the normal controls, they may be considered to be normal. 4 The criteria of maximum exercise used in the current study 20 are different from previous reports. 33 We used a BR value of < 30% in the current study, whereas previous reports have used a value < 15%. In addition, we used an respiratory exchange ratio value of ≥ 1.09 compared to ≥ 1.05 in previous reports and a heart rate ≥ 85% compared to 100% in previous reports. However, there is currently no gold standard to define maximal effort. 33
Conclusion
In addition to the volume effect of DH on tidal volume expandability in the COPD group, the similar TIpeak in the normal and COPD groups is key to understanding the pathophysiology that tidal inspiratory flow is another mechanism of lung expandability. Although the mechanisms of lung expandability are not clear in healthy individuals (probably exercise effort related), breathing time and flow in relation to exercise effort in healthy individuals may be weakened by impaired lung function. Tidal volume expandability was mildly higher than tidal inspiratory flow in relation to ED and EP in the COPD group.
Supplemental Material
Supplemental Material - Tidal volume expandability affected by flow, dynamic hyperinflation, and quasi-fixed inspiratory time in patients with COPD and healthy individuals
Supplemental Material for Tidal volume expandability affected by flow, dynamic hyperinflation, and quasi-fixed inspiratory time in patients with COPD and healthy individuals by Ming-Lung Chuang in Chronic Respiratory Disease
Footnotes
Authors' contributions
M.L.C. wrote the main manuscript text and prepared figures 1–2. All authors reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received grants from Chung Shan Medical University Hospital (CSH-2021-C-041). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript. None funding support was declared within the funding program Open Access Publishing.
Ethics approval and consent to participate
All methods were carried out in accordance with the local guidelines and regulations. The studies involving human participants were reviewed and approved by the local ethics committee at the Chung Shan Medical University of Taiwan (CS2-21018). The patients/participants provided their written informed consent to participate in this study.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental Material
Supplemental material for this article is available online
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.