
Abstract
Background
Dyspnoea and pain are symptoms of chronic obstructive pulmonary disease (COPD). This review focused upon pain and dyspnoea during hospital admissions for acute exacerbations of COPD (AECOPD), with the aim of examining prevalence, assessment, clinical associations, and researcher-reported implications of these symptoms.
Methods
Four electronic databases were searched from inception to 31 May 2021. Full text versions of studies were assessed for methodological quality and data were extracted independently by two reviewers. Where data permitted, pooled prevalence of pain and dyspnoea were calculated by meta-analysis.
Results
Four studies were included. The pooled prevalence of pain and dyspnoea was 44% (95% confidence interval (CI) 35%–52%) and 91% (95% CI 87%–94%) respectively. An array of instruments with varying focal periods were reported (pain: six tools, dyspnoea: four tools). Associations and clinical implications between the two symptoms at the time of hospital admission were rarely reported.
Conclusions
Few studies reported prevalence of pain and dyspnoea during an AECOPD. A greater understanding into the prevalence, intensity and associations of these symptoms during AECOPD could be furthered by use of standardised assessment tools with clearly defined focal periods.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive disease characterised by acute exacerbations. An exacerbation of COPD is an acute worsening of respiratory symptoms 1 and is characterised by changes in an individual’s baseline dyspnoea, cough and/or sputum beyond day-to-day variations, which may require a change in medication and/or admission to hospital. 2
While dyspnoea is recognised as the most characteristic feature of COPD with a reported prevalence of up to 93%, 3 pain has also been identified as a symptom affecting between 21% and 85% of people in a stable state.4–6 In people with stable COPD, pain exhibits a negative impact on mood and contributes to increased fatigue, heightened anxiety and depression, difficulty clearing secretions, fear-avoidance behaviour and poorer quality of life.7–10 Sensations of pain and dyspnoea are known to originate in afferent nervous systems, through which threat to the body is detected. 11 The sensory input generated by dyspnoea and pain have been found to be processed in similar regions of the brain, specifically the insula, dorsal anterior cingulate cortex, amygdala and medial thalamus. These regions are known to be involved in the processing of fear and anxiety, amongst other emotions. 12 These similarities in neural pathways and central structures explain why pain and dyspnoea are both described as unpleasant sensory and emotional experiences which are associated with sensory and affective dimensions.12–15
In stable COPD, a positive correlation between the presence of pain and dyspnoea has been demonstrated, both of which were found to negatively impact quality of life, 16 with individuals experiencing pain reporting higher dyspnoea scores compared to those without pain. 10 Current knowledge concerning the interaction between pain and dyspnoea has focused on people in the stable state of COPD. However, the clinical management of COPD varies between stable state and acute exacerbations, in response to changes in presenting symptoms. 2 These presenting symptoms commonly include an increase in dyspnoea, a known characteristic feature of acute exacerbations and a higher pain intensity and differing pain locations, compared to a stable condition. 17 These features have the potential to inform treatment decisions and subsequently influence recovery. However, the prevalence of both dyspnoea and pain in the same individual in this clinical state is comparatively underexplored. In light of the symmetry in neurophysiology and sensory and affective dimensions of each symptom, further understanding of the interactions between pain and dyspnoea and their clinical implications in those with an acute exacerbation of COPD is required. This review is the first step towards understanding the relationship between both symptoms in this population, with the potential to inform their co-influence on treatment efficacy and on other clinical outcomes, including duration of recovery.
Pain and dyspnoea in COPD are recognised as complex and aversive symptoms. To capture the complexity of each symptom, a number of tools have been developed to assess severity, impact and behaviour of these symptoms. However, it is not clear which instruments have been used to assess pain and dyspnoea in those with an acute exacerbation.
The primary aim of this review was to investigate the prevalence of pain and dyspnoea in people admitted to hospital with an acute exacerbation of COPD. The secondary aims were to (1) identify the tools and corresponding focal periods applied to assess pain and dyspnoea in acute exacerbations of COPD, and (2) to identify the clinical associations and researcher-reported implications of pain and dyspnoea, including the interaction between both symptoms in this clinical state.
Method
The protocol for this systematic review was registered with Prospero (CRD42020182386). The process for this systematic review was undertaken in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18
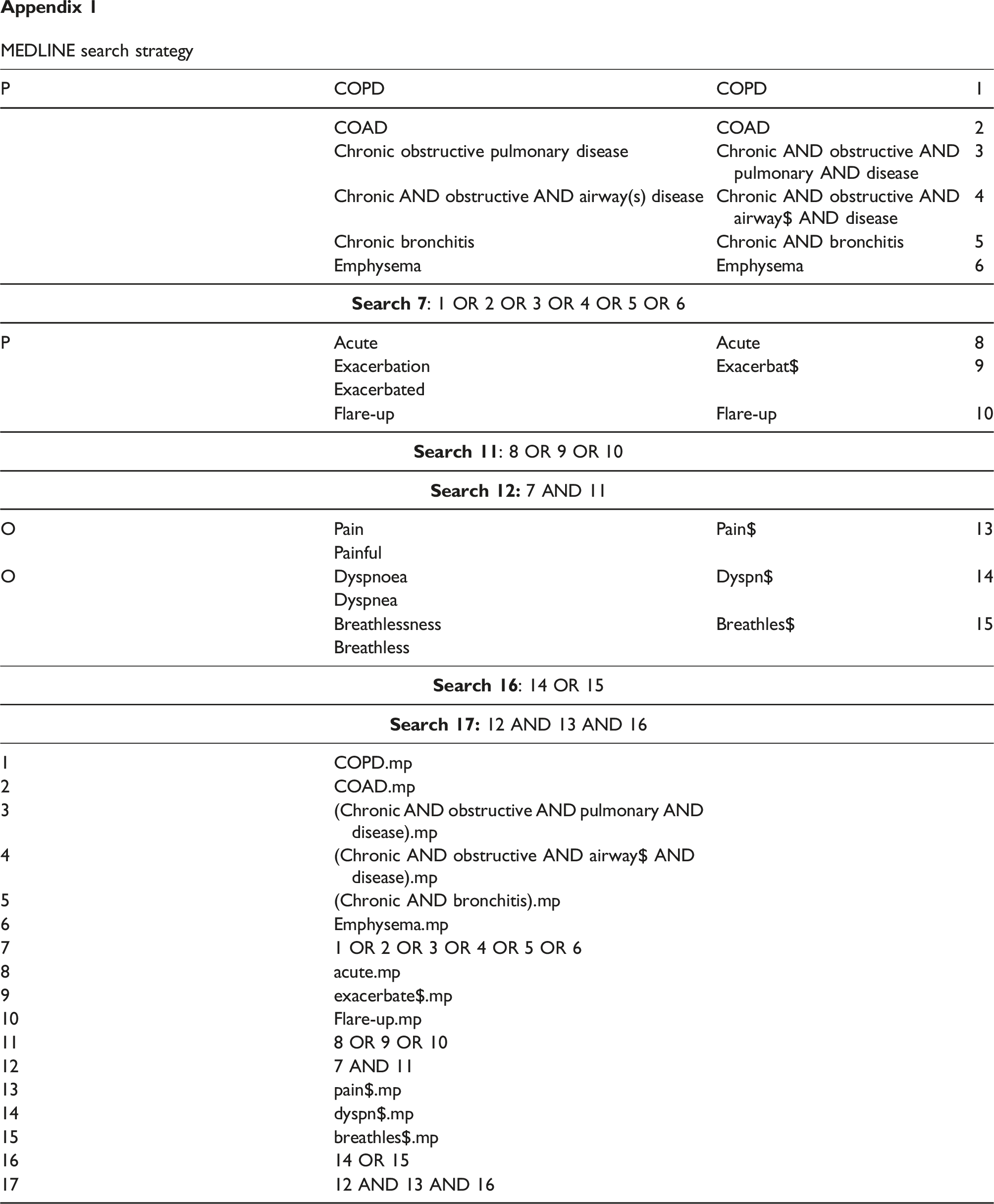
A systematic search of four databases (EMBASE, MEDLINE, Cochrane Library, CINAHL) was undertaken by one reviewer (S.Y.C). The search strategy for MEDLINE is referenced in Appendix 1 and was adapted for other databases. Searches were conducted from database inception to 31 May 2021. The years of inception for EMBASE, MEDLINE, Cochrane Library and CINAHL were 1974, 1966, 1993 and 1961 respectively.
Study inclusion criteria.

Data extraction was completed by reviewer S.Y.C., collated in Microsoft Excel and independently checked by reviewer A.L.L. Extracted data included study and patient demographics, prevalence of pain and dyspnoea, as well as instruments used, focal periods for symptom presence and clinical associations and implications reported for both pain and dyspnoea. The definition or nature of pain was not restricted, as it is recognised that pain may arise from different sources. 6 For this reason, pain may have been acute or chronic in nature, with a mix of possible aetiologies. This approach was adopted based on current knowledge of types and possible causes of pain in those in a stable clinical state, with a mix of pain experienced. 20 The focal period was identified as the period of time over which the assessment of each symptom was measured. For example, the Brief Pain Inventory (BPI) asks participants to rate their pain intensity as recalled over the past week. 21 Therefore, the focal period for the BPI is one week. Researcher-reported implications were defined as the clinical implications stated by authors within the publication.
All included studies were appraised using the risk of bias assessment tool described by Hoy et al., 22 which is specific to the assessment of prevalence studies. The tool assesses the risk of bias across four areas; selection bias, non-response bias, measurement bias and bias related to analysis. This was completed independently by two reviewers (S.Y.C and A.L.L), with any disagreements resolved during a consensus meeting.
Where data permitted, pooled prevalence of pain and dyspnoea were calculated using MetaXL 1.3 in Microsoft Excel (EpiGear International Pty LTD). The data were first transformed using the variance stabilising double arcsine transformation. 23 Using a quality effects model, the prevalence and 95% confidence interval for both pain and dyspnoea were calculated. This model was selected over the fixed or random effects model to explicitly address heterogeneity in pooled proportions caused by differences in study quality and distribution, with greater weighting given to studies of higher methodological quality. 24 Heterogeneity was assessed using the Q and I2 measures calculated by MetaXL 1.3. Study findings that were not able to be pooled were reported narratively.
Deviations to published protocol
The Downs and Black tool was originally selected to assess the risk of bias of included studies, prior to the identification of studies meeting the inclusion criteria. Based on the types of included studies, the tool by Hoy et al. was utilised as it is specific to the assessment of risk of bias in prevalence studies.
Results
Study selection
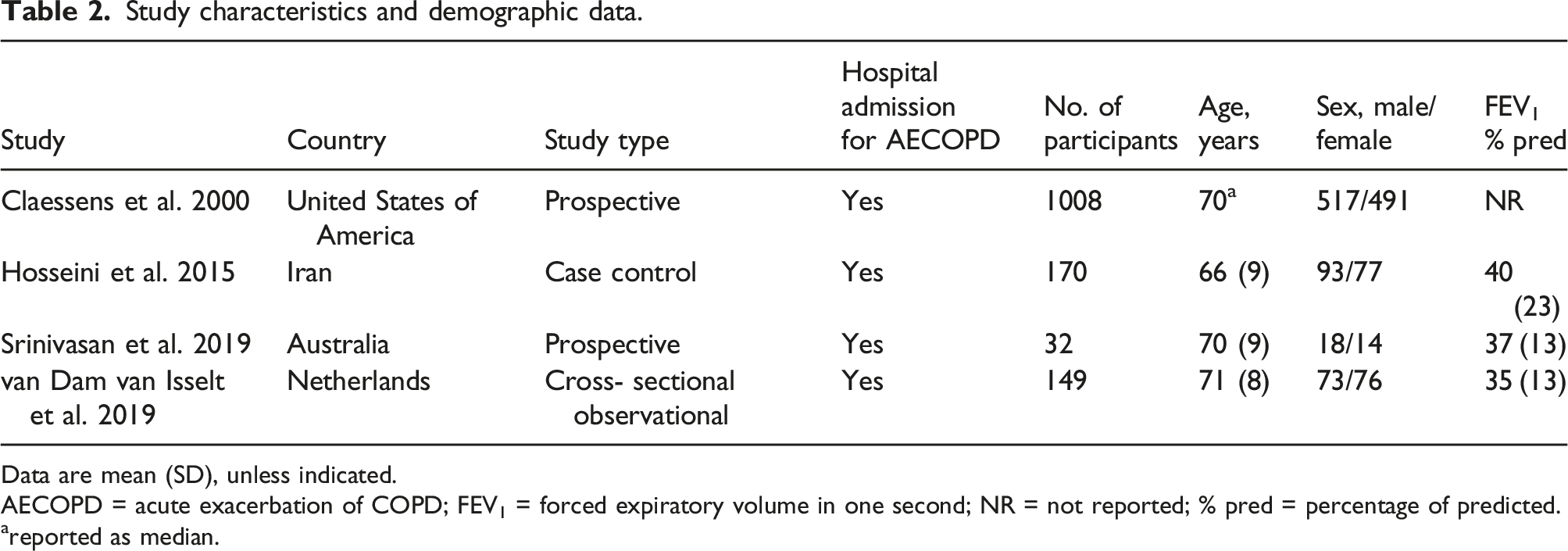
A total of 1300 potentially eligible articles published before 31 May 2021 were identified. Following removal of 144 duplicates, 1156 titles and abstracts were screened, from which 34 full-text articles were further evaluated against the inclusion criteria (Table 1). Four studies published between 2000 and 2019 were eligible for inclusion within this review (Figure 1). These included two prospective studies, one case-control study and one cross-sectional observational study. The number of participants in the included studies ranged from 32 to 1008. Disease severity of participants was reported in three studies25-27 with measures of forced expiratory volume in one second indicating participants had severe airflow limitation (Forced expiratory volume in one second (FEV1) mean ranging from 35 to 40% of predicted value).
1
Study characteristics and demographic data are presented in Table 2. Study flow diagram from identification of records to inclusion of studies. CINAHL: Cumulative Index to Nursing and Allied Health Literature; EMBASE: Excerpta Medica Database. Study characteristics and demographic data. Data are mean (SD), unless indicated. AECOPD = acute exacerbation of COPD; FEV1 = forced expiratory volume in one second; NR = not reported; % pred = percentage of predicted. areported as median.
Risk of methodological bias assessment
Assessment of risk of bias of included studies.

Key to scoring (14): Yes = yes (low risk), No = no or insufficient information to permit a judgment (high risk).
Measurement tools and focal periods of assessment for pain
Measures and scales used in included studies.

COPD = chronic obstructive pulmonary disease; QOL = quality of life.
arecording change in symptoms over last 48 h.
b5-point Likert scale.
Prevalence of pain
Prevalence, scales, focal periods, characteristics and associations of pain.

# = n unable to be established from available data; * = significant difference (p ≤ 0.05); NR = Not reported; SD = standard deviation.

Pooled prevalence of (a) pain reported in included studies; and (b) dyspnoea reported in included studies.
Characteristics and associations of pain
The nature of the pain experienced was not identified in any of the included studies. The characteristics of pain (intensity and/or location) during an acute exacerbation were reported in two studies.26,27 Average pain of 4.8 on an intensity scale from zero to 10 was reported in one study. 26 Similarly, Van Dam van Isselt et al. 27 reported a mean score of pain “right now” at 4.1 points as measured by the BPI pain intensity scale. Two studies reported on the location of pain,26,27 with commonly reported locations being chest, back and shoulders/arms (Table 5). According to van Dam van Isselt et al., 27 BPI derived pain interference scores were highest for interference with normal work, walking ability and general ability (Table 5).
One study comparing demographic data between those with and those without pain reported no difference in age, sex or disease characteristics (FEV1, comorbidity score, nutritional status and smoking status) between the two groups. 27 The percentage of participants with muscle pain was higher in those infected with a respiratory virus compared to uninfected participants. 25 Use of analgesia was reported in one study, 27 with paracetamol being the most commonly used analgesic.
Van Dam van Isselt et al. 27 examined the effect of pain on disease-specific quality of life; those with pain had significantly poorer disease-specific health status as measured by the Clinical COPD Questionnaire. In an analysis of subdomains, only the function subdomain was worse in patients with pain, compared to those without pain. 27 The prevalence and intensity of both anxiety and depression as well as fatigue, muscle weakness and anorexia were higher in those with pain compared to those without pain. 27 While there was no difference in the prevalence of insomnia between those with and those without pain, the intensity of insomnia was higher in those with pain. 27
Measurement tools and focal periods for assessment of dyspnoea
Prevalence, scales, focal periods, characteristics and associations of dyspnoea.

mMRC = modified medical research council; NR = not reported; NSD = no significant difference p ≥ 0.05.
an unable to be established from available data.
Only one study used a validated tool for people with COPD: the modified Medical Research Council (mMRC) Dyspnoea Scale. 27 The specific focal period for the mMRC was not specified, only that it was completed by participants during their admission with exacerbation. 27 Srinivasan et al. 26 assessed the presence of dyspnoea within 72 hours of admission using the CMSAS, which has a focal period of the past 7 days. Claessens et al. 28 included two questions about dyspnoea, but the precise focal period assessed was unclear. Hosseini et al. 25 used a diary card for monitoring of changes in symptoms, including dyspnoea, over the preceding 48 hours.
Prevalence of dyspnoea
Reported prevalence of dyspnoea ranged from 56% to 91% (Table 6). Of the four included studies, while one 28 reported on the prevalence of dyspnoea, the means by which the prevalence was calculated and the number of participants to whom this prevalence applied was not clear. Therefore, this study was excluded from the meta-analysis. The overall pooled prevalence was 91% (95% CI 87%–94%) (Figure 2(b)). Heterogeneity measures of Q = 0.08 and I2 = 0 indicate a low level of heterogeneity across studies.
Characteristics and associations of dyspnoea
No significant difference in dyspnoea prevalence or intensity was reported between those with and those without pain (Table 6). 27 Breathlessness (sic) was both the most prevalent and bothersome symptom reported on the CMSAS in one study. 26 An increase in dyspnoea was present both in participants infected with respiratory virus and those who were respiratory virus negative, but no statistical comparison was reported 25 (Table 6).
Clinical implications and interactions of pain and dyspnoea reported within studies
A single study 27 reported the implications of pain in exacerbations of COPD, stating that “Pain in this specific group of patients needs more attention, as our study suggests that pain treatment is suboptimal” and that “incorporation of standard pain assessment in stable COPD and during exacerbations and post-acute pulmonary rehabilitation is recommended”.
Discussion
This systematic review aimed to identify the prevalence of both pain and dyspnoea experienced concurrently in people admitted to hospital with an exacerbation of COPD. Using all available data, pooled prevalence of pain and dyspnoea was 44% and 91% respectively. An array of different outcomes measures with varying time frames were applied within the studies for pain (six tools) and dyspnoea (four tools) with limited synthesis of clinical characteristics at the time of a hospital admission. The reporting of clinical associations, implications of both symptoms and their interaction in acute exacerbations of COPD was rare. 27
Less than 10% of clinical practice guidelines for management of COPD make reference to pain as a symptom affecting this population. 29 In a recent systematic review of outcome measures used in the management of exacerbations of COPD, 30 pain was not identified as a symptom that is evaluated in this disease state. Of two studies to date which examined pain during an acute exacerbation of COPD independent of the presence of dyspnoea, the prevalence ranged from 31.3% to 96%.17, 31 The clinical priority in management of COPD exacerbations is aimed at resolving the underlying acute physiological problems including airflow limitation, mucus production, infection, hypoxia, hypercarbia and acidosis. 2 With the focus on addressing these potentially life-threatening problems, pain may be considered to be of comparatively lower clinical importance, resulting in it being less frequently considered as a feature of an exacerbation of COPD. The failure to recognise pain as a symptom of COPD and the limited investigation into the co-existence and interaction between pain and dyspnoea may account for the very small number of studies investigating the prevalence of both symptoms experienced concurrently in individuals with acute exacerbations of COPD.
In the small number of included studies, there was a wide range in the reported prevalence of pain. This variability may be attributable to variations in scales, different focal periods and diverse definitions to determine the presence of pain. Currently, there does not appear to be consensus for optimal tools to assess pain in people living with COPD (stable or exacerbated states). A systematic review investigating the tools used for assessment of pain in stable state COPD found the BPI (short form) was most commonly used, with numerical rating scales, McGill Pain Questionnaire and BPI (long form) also used to quantify pain intensity. 6 The focal periods in the studies in our review were commonly defined by the tools used, and varied from 48 hours, seven days or no defined time frame. While the choice of focal period may be dictated by the tool selected, this symptom is likely to vary in severity over the course of an acute exacerbation, with the potential for greater prevalence and severity early in an admission. This is illustrated by Maignan et al., 17 who reported a pain prevalence of 92%, with the measurement completed within six hours of admission for an acute exacerbation of COPD. The available information about the intensity and location of pain during exacerbations is drawn from two studies.26,27 While using different tools, both studies included assessment of pain intensity on a numerical rating scale and reported pain to be between 4 and 5 (from 0–10) during exacerbation. Common locations of pain included the chest, back and shoulders.26,27 This is consistent with the findings of Maignan et al., 17 who reported the chest as the predominant location of pain during exacerbations of COPD, together with the upper back and trunk. Further investigation into the experience of pain at various time points during exacerbation, using validated tools such as the BPI (short form) or McGill Pain Questionnaire would allow assessment of the presence and prevalence of pain within tightly defined focal periods, and would provide valuable insight into the characteristics and nature of pain throughout an exacerbation. This will further the understanding of the prevalence of pain and symptom behaviour in this disease state.
Similarly, the tools and associated focal periods used to assess dyspnoea varied between studies, with only one study assessing intensity. As dyspnoea is a key characteristic of exacerbations of COPD, 2 it is unsurprising that the prevalence of dyspnoea was consistently high in all studies. A greater understanding of the fluctuation in prevalence, intensity and nature of dyspnoea could be gained from the use of multidimensional dyspnoea instruments such as the Multidimensional Dyspnoea Profile to quantify and characterise the experience of dyspnoea during an exacerbation of COPD. A recent study 32 of dyspnoea during an inpatient hospital admission reported that patients with mixed diagnoses including respiratory disease who reported any level of dyspnoea were at increased risk of death during that admission, with the severity of dyspnoea proportional to the risk of mortality. This further emphasises the importance of exploring this symptom in this clinical state.
Little is known about whether pain experienced by people during exacerbations represents a new symptom or whether it is of a differing nature and intensity to that experienced during stable state. Maignan et al. 17 reported the prevalence and intensity of pain as significantly higher during exacerbations compared to stable state, with differing pain locations between the two disease states. Further exploration of differences in pain prevalence and experience between disease states would broaden our understanding of this symptom during exacerbations of COPD.
There is very little evidence about the clinical associations of pain during an exacerbation of COPD. Only one study 27 indicated that the prevalence and intensity of other symptoms such as fatigue, anxiety and weakness was higher in those with pain. While these preliminary findings align with reports of the clinical association between pain and other symptoms (including dyspnoea) in those in a stable disease state,5,6 the paucity of information about the clinical associations, impacts and benefits of treatment of pain during exacerbations, likely stems from the under-recognition of pain as a symptom in this disease state.
With such limited evidence about the prevalence and experience of co-occurring pain and dyspnoea during exacerbations of COPD, there have been limited clinical implications drawn from the available research. The recommendations by van Dam van Isselt et al. 27 highlight that for many people with COPD, pain is a relevant problem but is under-assessed, under-treated and not commonly factored into patient care during an acute exacerbation. For example, discharge care bundles are sets of evidence-based practices targeted at improving patient outcomes on discharge following exacerbations, and that have been shown to reduce readmission rates. 33 Discharge criteria from acute care following exacerbations are predominantly focused on resolution of dyspnoea, reduction in medication and oxygen requirements, return to baseline function and follow-up arrangements. 2 A systematic review of discharge care bundles explored the individual interventions included, but assessment and strategies for pain were not singled out, nor considered in conjunction with symptoms of dyspnoea and it is unclear if pain was considered within the education and care plans for self-management strategies. 33 While the current knowledge about the relationship between pain and quality of life, function and other symptoms 6 supports the recommendations for pain assessment to be included in clinical care of people with COPD, 5 a more robust understanding of these relationships specifically during exacerbations will give more strength to this recommendation.
Pain and dyspnoea have been identified as two of the most frequent and serious symptoms experienced by those requiring palliative care, with the need to control these symptoms recognised as an important part of reducing suffering. 34 In contrast, treatment of COPD exacerbations is directed at resolving the underlying physiological problems. 2 In those with severe COPD, a symptom-based management approach during exacerbation may increase the recognition of pain as a symptom affecting this patient cohort.
There are several limitations of this review. There were a very small number of studies eligible for inclusion that reported on the prevalence of both pain and dyspnoea. There was considerable variability in the sample size of the included studies, with only one study powered for the primary aim of investigating the prevalence of pain. There was little consistency between scales and focal periods used to assess pain and dyspnoea, making it challenging to synthesise information. Included studies were limited to those available in English, retrieved from four databases, but the impact of these limitations is unknown. Assessment of publication bias was not undertaken, as it is not recommended for a review of less than 10 studies. 35 Selection bias is unlikely to have impacted the findings of the study. The risk of non-response bias was high in all studies. While all studies had specific inclusion criteria to select participants that were reflective of the intended population, the extent to which the results could be extrapolated to national populations was unclear, as the studies were conducted at either a single site, or small number of sites across a large geographical area. The use of non-validated tools and lack of clear definitions of pain in most studies may introduce a degree of measurement bias.
While there is limited published evidence surrounding the assessment of pain and dyspnoea in acute exacerbations of COPD using standardised assessment tools, this may not be representative of how these symptoms are considered in frontline clinical care. Exploration of the practices of a patient’s care team in assessing these symptoms during acute exacerbations of COPD opens an avenue for further research in this area. The impact of pain and dyspnoea on other clinical indicators such as hospital length of stay, and time to recovery from exacerbations of COPD require further exploration to understand the implications of these symptoms in this clinical state.
Within this review, the pooled prevalence of pain and dyspnoea in acute exacerbations of COPD was 44% and 91% respectively. Different outcomes measures were applied for pain and dyspnoea and the focal periods for assessment were defined by the assessment tool used. Despite the findings of this review demonstrating that pain and dyspnoea are experienced by a considerable proportion of people at the time of an acute exacerbation of COPD, the reporting of clinical associations and implications of both symptoms in this clinical state is minimal. In the treatment of an exacerbation of COPD, the management of pain is likely to be a lower clinical priority than correcting the underlying pathophysiological problems associated with the exacerbations. A greater understanding into the prevalence, intensity and associations of pain during exacerbations could be furthered by use of standardised assessment tools and clearly defined focal periods to capture the nature of pain and dyspnoea over the course of an exacerbation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
MEDLINE search strategy
| P | COPD | COPD | 1 |
|---|---|---|---|
| COAD | COAD | 2 | |
| Chronic obstructive pulmonary disease | Chronic AND obstructive AND pulmonary AND disease | 3 | |
| Chronic AND obstructive AND airway(s) disease | Chronic AND obstructive AND airway$ AND disease | 4 | |
| Chronic bronchitis | Chronic AND bronchitis | 5 | |
| Emphysema | Emphysema | 6 | |
| P | Acute | Acute | 8 |
| Exacerbation | Exacerbat$ | 9 | |
| Exacerbated | |||
| Flare-up | Flare-up | 10 | |
| O | Pain | Pain$ | 13 |
| Painful | |||
| O | Dyspnoea | Dyspn$ | 14 |
| Dyspnea | |||
| Breathlessness | Breathles$ | 15 | |
| Breathless | |||
| 1 | COPD.mp | ||
| 2 | COAD.mp | ||
| 3 | (Chronic AND obstructive AND pulmonary AND disease).mp | ||
| 4 | (Chronic AND obstructive AND airway$ AND disease).mp | ||
| 5 | (Chronic AND bronchitis).mp | ||
| 6 | Emphysema.mp | ||
| 7 | 1 OR 2 OR 3 OR 4 OR 5 OR 6 | ||
| 8 | acute.mp | ||
| 9 | exacerbate$.mp | ||
| 10 | Flare-up.mp | ||
| 11 | 8 OR 9 OR 10 | ||
| 12 | 7 AND 11 | ||
| 13 | pain$.mp | ||
| 14 | dyspn$.mp | ||
| 15 | breathles$.mp | ||
| 16 | 14 OR 15 | ||
| 17 | 12 AND 13 AND 16 |