
Abstract
Background and purpose
High blood urea nitrogen (BUN) is associated with an elevated risk of mortality in various diseases, such as heart failure and pneumonia. Heart failure and pneumonia are common comorbidities of acute exacerbation of chronic obstructive pulmonary disease (AECOPD). However, data on the relationship of BUN levels with mortality in patients with AECOPD are sparse. The purpose of this study was to evaluate the correlation between BUN level and in-hospital mortality in a cohort of patients with AECOPD who presented at the emergency department (ED).
Methods
A total of 842 patients with AECOPD were enrolled in the retrospective observational study from January 2018 to September 2020. The outcome was all-cause in-hospital mortality. Receiver operating characteristic (ROC) curve analysis and logistic regression models were performed to evaluate the association of BUN levels with in-hospital mortality in patients with AECOPD. Propensity score matching was used to assemble a cohort of patients with similar baseline characteristics, and logistic regression models were also performed in the propensity score matching cohort.
Results
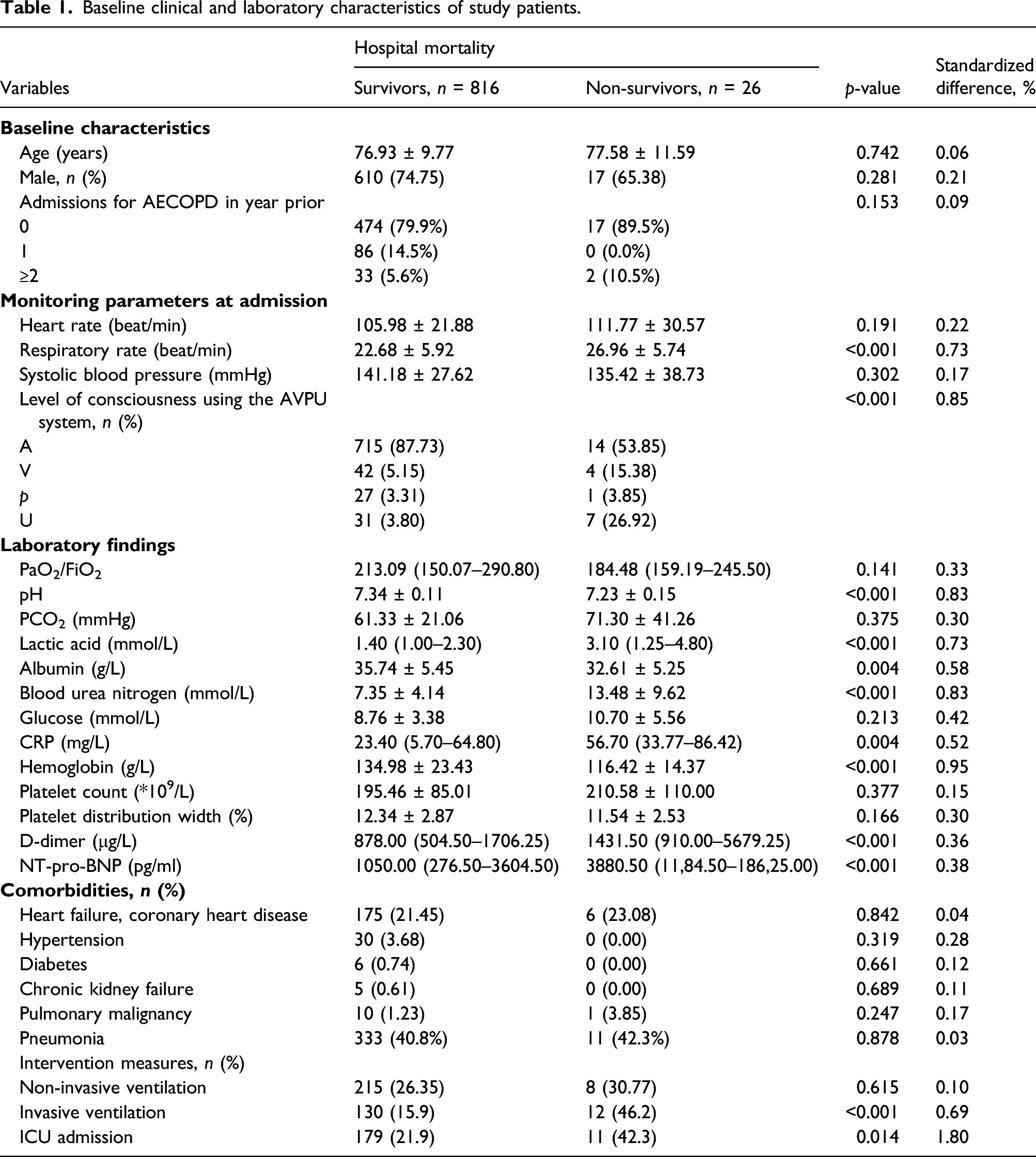
During hospitalization, 26 patients (3.09%) died from all causes, 142 patients (16.86%) needed invasive ventilation, and 190 patients (22.57%) were admitted to the ICU. The mean level of blood urea nitrogen was 7.5 ± 4.5 mmol/L. Patients in the hospital non-survivor group had higher BUN levels (13.48 ± 9.62 mmol/L vs. 7.35 ± 4.14 mmol/L, p < 0.001) than those in the survivor group. The area under the curve (AUC) was 0.76 (95% CI 0.73–0.79, p < 0.001), and the optimal BUN level cutoff was 7.63 mmol/L for hospital mortality. As a continuous variable, BUN level was associated with hospital mortality after adjusting respiratory rate, level of consciousness, pH, PCO2, lactic acid, albumin, glucose, CRP, hemoglobin, platelet distribution width, D-dimer, and pro-B-type natriuretic peptide (OR 1.10, 95% CI 1.03–1.17, p=0.005). The OR of hospital mortality was significantly higher in the BUN level ≥7.63 mmol/L group than in the BUN level <7.63 mmol/L group in adjusted model (OR 3.29, 95% CI 1.05–10.29, p=0.041). Similar results were found after multiple imputation and in the propensity score matching cohort.
Conclusions
Increased BUN level at ED admission is associated with hospital mortality in patients with AECOPD who present at the ED. The level of 7.63 mmol/L can be used as a cutoff value for critical stratification.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality worldwide. 1 It has a chronic and progressive course that is often punctuated by “exacerbations,” which are driven by respiratory infections, and multiple functional impairments and comorbidities.2–4 The aims of acute exacerbation of chronic obstructive pulmonary disease (AECOPD) treatment are to minimize the negative impact of the current exacerbation and to prevent the development of subsequent events. 5 Patients with AECOPD can be managed in either the inpatient or outpatient setting depending on the severity of the exacerbation and/or the severity of the underlying disease. 3 Therefore, risk stratification is crucial to provide an optimal level of care and select appropriate medical and interventional treatments. 6
High blood urea nitrogen (BUN), which indicates impaired cardiorenal functions and unfavorable neurohormonal activation, 6 is generally considered to be an ominous sign in various diseases. For example, it is associated with poor prognosis in patients with heart failure, aortic dissection, peripheral artery disease, acute necrotizing pancreatitis, and hospital-acquired pneumonia. 7 Among critically ill patients, elevated BUN level is associated with increased mortality, independent of serum creatinine. 8 The BAP65 9 and CURB65, 10 which were originally used to predict the community-acquired pneumonia mortality risk, also performed well in patients with AECOPD. The BUN is one of the parameters in these two models.
Patients with AECOPD often experience hypoxia, carbon dioxide retention, and systemic inflammation, 11 which may affect cardiorenal functions and neurohumoural regulation. Moreover, heart failure and pneumonia are common comorbidities of AECOPD, so high BUN levels are likely to be associated with poor prognosis of AECOPD. However, to date, no study has evaluated the relationship of BUN levels upon admission for AECOPD on the outcome of hospital survival. As it is a routine blood test, a detailed analysis of BUN levels’ relation to mortality seems worthwhile. Therefore, this study aimed to specifically investigate the association between BUN level and mortality in patients with AECOPD in an observational study.
Methods
Study design and participants
We conducted a retrospective, observational cohort study at the emergency department (ED) of Jinhua Municipal Central Hospital in Zhejiang Province, China. The clinical data of eligible patients who underwent treatment in the ED for AECOPD between January 2018 and September 2020 were included. Patients were initially identified on the basis of the ICD-10 (International Statistical Classification of Diseases and Related Health Problems) (2014) codes for “AECOPD” (J44.1) and “respiratory failure” (J96) in the hospital electronic database.
The inclusion criteria were as follows: patients with a primary diagnosis of AECOPD or respiratory failure and a secondary diagnosis of AECOPD. AECOPD was defined as (1) a COPD history and (2) acute-onset sustained worsening in baseline dyspnea, cough, and/or sputum that warranted a change in regular medication. The exclusion criteria were as follows: (1) patients requiring immediate cardiopulmonary resuscitation; (2) patients who had been admitted to the neurology and cardiology wards for other acute diseases, including cerebral hemorrhage, myocardial infarction, poisoning, etc.; (3) patients who complicated with other respiratory diseases, such as pneumothorax, pleural effusion and pulmonary embolism, etc.; and (4) patients with gastrointestinal bleeding.
A total of 1062 patients were potentially eligible for this analysis; among them, 842 patients remained after applying the exclusion criteria (Figure 1). This retrospective cohort study was approved by the Ethics Committee of Jinhua Municipal Central Hospital (No. 2020-254). The requirement for informed consent was waived since the data were anonymous.
Data collection and outcome assessment
Patient demographics, including age, sex, and comorbidities, with a special emphasis on cardiopulmonary disease, hypertension, diabetes, chronic renal failure, pulmonary malignancy, and pneumonia identified from the medical record review, were recorded. Clinical parameters were recorded at ED admission, such as vital signs (heart rate, respiratory rate, and systolic blood pressure) and consciousness (“alert,” “verbal,” “pain,” and “unresponsive”). We collected initial laboratory findings obtained within 1 h of the ED visit, including arterial blood gases (pH, PaO2/FiO2, PaO2, and lactic acid), routine chemical tests (BUN, albumin, and glucose), hematology tests (hemoglobin, platelet count, and platelet distribution width), C-reactive protein, D-dimer, and N-terminal pro-B-type natriuretic peptide (NT-pro-BNP). Comorbidities were confirmed by patient medical history or medication use. Pneumonia was identified by chest CT scan. The endpoint was all-cause in-hospital mortality. In-hospital mortality refers to death during hospitalization in this visit or death within 24 h of hospital discharge.
At the study site, the initial vital signs (heart rate, respiratory rate, blood pressure, and consciousness) were recorded in the emergency triage system, which is integrated with electronic medical records. Furthermore, patient demographics, comorbidities, laboratory tests, and clinical interventions could be accessed from the electronic medical records.
Statistical analysis
The patients’ baseline characteristics were summarized using descriptive statistics. Continuous variables are presented as the mean ± standard deviation or median (interquartile range). Between-group comparisons of normally and non-normally distributed continuous variables were performed using Student’s t-test and the Mann–Whitney U test, respectively. Categorical variables were expressed as absolute numbers with percentages and analyzed by chi-square or Fisher’s exact test, as appropriate.
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the association of BUN levels with outcomes. An optimal BUN level cutoff was calculated by means of the Youden Index. Multivariate adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for the study outcomes and BUN (1 unit, two groups categorized by the optimal BUN level cutoff) were calculated with logistic regression analysis. After checked for multicollinearity, covariates were selected as potential confounders if they changed the estimates of BUN level on outcomes by more than 10% or were significantly associated with outcomes.12,13 Supplementary Tables S1–S3 show the associations of each confounder with the outcomes of interest and changes in the effect estimate.
We used multiple imputation, based on five replications and a chained equation approach method in the R MI procedure, to account for missing data on covariates. We repeated all analyses with the complete data cohort for sensitivity analyses. Supplementary Tables S4 and S5 give additional details of the statistical analyses.
Given the differences in the baseline characteristics between survivor and non-survivor groups, propensity score matching was used to identify a cohort of patients with similar baseline characteristics (Supplementary Tables S6 and S7). We estimated the propensity score with the use of a non-parsimonious multivariable logistic regression model, with non-survivor as the dependent variable and confounders adjusted in model 2 as covariates. A 1:1 matching protocol was used for matching, with a caliper width equal to 0.01 of the standard deviation of the logit of the propensity score. Logistic regression analysis also performed in the matched cohort. Covariates were selected as potential confounders if they met both of the two conditions: associations with the outcomes of interest and a change in effect estimate of more than 10%.
All statistical analyses were conducted using EmpowerStats (www.empowerstats.com), R 3.5.1 (www.r-project.org), and MedCalc version 15 for Windows (MedCalc Software bvba). p-values < 0.05 were considered statistically significant.
Results
We evaluated 1062 consecutive patients admitted for AECOPD. BUN level results were missing in approximately 18% (191) of patients with AECOPD, and 842 were eligible for inclusion in the present study. The flowchart of the study participants is shown in Figure 1. The average age of study patients was 77.0 ± 9.8 years, and 627 (74.5%) patients were male. The mean level of BUN was 7.5 ± 4.5 mmol/L. The hospital mortality rate, invasive ventilation rate, and ICU admission rate were 3.09%, 16.86%, and 22.57%, respectively.
Baseline characteristics
Baseline clinical and laboratory characteristics of study patients.
BUN level and hospital mortality of AECOPD
To evaluate the relationship between BUN level and hospital mortality, we performed ROC curve analysis of BUN level against the outcomes (Figure 2). The AUC was 0.76 (95% CI 0.73–0.79, p < 0.001), and the optimal BUN level cutoff was 7.63 mmol/L for hospital mortality. The sensitivity and specificity was 76.92 and 66.54, respectively.
Logistic regression of blood urea nitrogen for mortality in all study groups.

Model one adjusted for sex and age.
Model two adjusted for respiratory rate, level of consciousness, pH, PCO2, lactic acid, albumin, glucose, CRP, hemoglobin, platelet distribution width, D-dimer, and NT-pro-BNP. BUN, blood urea nitrogen; OR, odds ratios; CI, confidence interval.
In addition, all participants were stratified into two groups (BUN level <7.63 mmol/L, ≥ 7.63 mmol/L). The OR of hospital mortality was significantly higher in the BUN level ≥7.63 mmol/L group than in the BUN level <7.63 mmol/L group in univariate, adjusted model one, and adjusted model two logistic regression analyses (p < 0.05). The results of logistic regression analysis after multiple imputation were consistent with those of the original data analysis (Supplementary Tables S5). So was in the matched cohort (Supplementary Tables S7).
Discussion
To the best of our knowledge, based on the available literature, this is the first study to explore the association of BUN level, a widely available and rapidly measured biomarker, with all-cause hospital mortality in patients with AECOPD who present to the ED. In the present study, the serum BUN level at ED admission showed a significant association with inpatient mortality following multivariable adjustments, including respiratory rate, level of consciousness, pH, PCO2, lactic acid, albumin, glucose, CRP, hemoglobin, platelet distribution width, D-dimer, and NT-pro-BNP. The optimal BUN level cutoff was 7.63 mmol/L for hospital mortality.
AECOPD is a common presentation in the ED that is associated with a mortality rate of 1.8%–8%.14–17 A number of studies have explored the risk factors associated with mortality in patients with AECOPD so far, and it is known that albumin, respiratory rate, blood gas analysis (PCO2, hemoglobin, lactic acid, etc.), inflammation-related indicators, etc. are important prognostic factors for mortality in these patients,18–23 which is in line with our findings.
As a biomarker of heart failure, the concentrations of NT-pro-BNP on admission of AECOPD provide independent prognostic information about mortality. 24 In our cohort, however, there was no significant association between heart disease and in-hospital mortality in patients with AECOPD. This might be because that cardiovascular disease is prevalent and frequently unrecognized in patients with COPD. 24 Patients with AECOPD have local or systemic inflammation, and inflammation can lead to increased levels of coagulation markers. 25 At the same time, venous thromboembolism is a common problem in COPD patients hospitalized with an exacerbation, leading to an increased risk of death. 26 Thus, an increase in D-dimer is associated with adverse outcomes, and it is an independent risk factor for in-hospital and 1-year death in patients with AECOPD. 27 Our study showed that the level of D-dimer of the hospital non-survivor group was higher than that of the hospital survivor group.
BUN level is associated with mortality in various cardiovascular diseases. Studies have demonstrated that in patients with acute decompensated heart failure, BUN levels maintained an independent and significant positive correlation with all-cause mortality.28–30 A high BUN level could be a useful predictor of in-hospital mortality in acute myocardial infarction patients. 31 In patients with pulmonary disease, BUN level has also been shown to be associated with poor prognosis. In a retrospective study of acute pulmonary embolism patients treated with tissue-plasminogen activator, in-hospital mortality rates were significantly higher in the elevated BUN level group than in the lower BUN level group. 32 In both patients with aspiration pneumonia and community-acquired pneumonia, significant differences were observed in BUN levels between the survivor and non-survivor groups.33,34 BUN level was also identified as a primary risk factor for COVID-19 mortality.35,36 BUN level has also been shown to be associated with adverse outcomes in older emergency patients and critically ill patients.37,38 The risk prediction models BAP65 and CURB65, which include BUN levels, have recently been shown to have a good predictive effect on AECOPD mortality.10,11 All these findings of above study, combined with clinical practice, have led to the hypothesis that BUN levels may be associated with in-hospital mortality in AECOPD.
However, the relationship of BUN levels and in-hospital mortality in patients with AECOPD is unclear since no relevant study has focused on the association between them. The present study investigated the relationship between BUN level and hospital mortality in patients with AECOPD who presented to the ED. We found that BUN level was significantly associated with mortality in AECOPD. These associations were independent of potential lung function, nutritional status, and inflammation confounders.
In addition, to reduce bias and the likelihood of overestimating the association, we adjusted for a wide range of potential confounding factors. 13 Meanwhile, we performed sensitivity analysis for the missing data with multiple interpolations, and the results are similar to the original data analysis. This means that the potential effects of selection bias in our study were likely limited. 13 The correlation between BUN and in-hospital mortality in AECOPD was further confirmed by the analysis in the matched cohort. An admission BUN of 7.63 mmol/L was identified through an ROC analysis as an optimal cutoff value to predict the in-hospital mortality. The results from this study are helpful for ED staff. They can select appropriate medical and interventional treatments according to BUN level upon emergency admission.
The precise mechanisms underlying the association between elevated BUN levels and AECOPD mortality remain unclear. Potential explanations for this might be as follows: BUN level is considered to be a marker of neurohumoural activity, cardiorenal functions, and catabolic conditions.38,39 Although frequently unrecognized, cardiovascular disease is prevalent in patients with COPD, 24 which can activate the SNS and RAS and then decrease eGFR and increase tubular urea reabsorption. 40 Respiratory infections are the main reason for “exacerbations” in patients with COPD. Patients with pneumonia often have hydration status resulting in increasing reabsorption of urea by the kidneys, and elevation of BUN levels is frequently observed. 41 “Exacerbations” and the use of glucocorticoids enhance catabolism, 42 which increases the source of BUN. 43 However, the impact of these mechanisms should be evaluated with further studies.
Limitations
This study has potential limitations. First, this was a single-center study. Thus, although great attention was given to including all consecutive patients with AECOPD to avoid selection bias, selection bias was still possible. Another limitation of the study originates from the retrospective design. We were not able to obtain all baseline characteristics and follow-up parameters. We were unable to evaluate how the excluded patients affected the study results. Furthermore, given the limitations in the ED, we did not collect other factors associated with AECOPD mortality, including history of smoking or long-term oxygen treatment, lung function (such as FEV1), and BMI. We also did not collect data on the use of diuretics, which may affect BUN level. Therefore, we could not determine the correlation between these factors and death. However, we collected other relevant data that can partially substitute for these parameters, such as blood gas analysis, which can reflect a patient’s lung function, and albumin, which reflects a patient’s nutritional status. They were adjusted as covariates in logistic regression analysis, and BUN level was still significantly related to adverse outcomes in patients with AECOPD. Moreover, BUN level was measured only at admission, as studies have reported that there is a strong association between the extent of BUN level rise during the first 24 h and mortality. 16 The intervention during the time patients were hospitalized was also not considered, which was associated with patient outcomes. Finally, the results of this study cannot represent all patients with AECOPD because it only targeted patients who presented in the ED. The cutoff of this study needs to be validated in an independent sample.
Conclusions
BUN level at admission was associated with increased all-cause in-hospital mortality in patients with AECOPD who presented at the ED. Therefore, as an inexpensive and easy-to-perform parameter, an elevated admission of BUN level should be a risk signal to alert physicians to perform early intervention efforts.
Supplemental Material
sj-pdf-1-crd-10.1177_14799731211060051 – Supplemental Material for The association of blood urea nitrogen levels upon emergency admission with mortality in acute exacerbation of chronic obstructive pulmonary disease
Supplemental Material, sj-pdf-1-crd-10.1177_14799731211060051 for The association of blood urea nitrogen levels upon emergency admission with mortality in acute exacerbation of chronic obstructive pulmonary disease by Lan Chen, Lijun Chen, Han Zheng, Sunying Wu and Saibin Wang in Chronic Respiratory Disease
Footnotes
Author contributions
LC and SBW jointly designed the study. LJC, HZ and SYW collected the data. LC and SBW performed the statistical analyses. LC drafted the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of Jinhua Municipal Central Hospital (No. 2020-254).
Informed consent
The data were anonymous, and the requirement for informed consent was therefore waived.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplementary Material
Supplementary Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.