
Abstract
Instrumental activities of daily living (IADL) are significantly related to quality of life and mortality among individuals with heart disease. However, few reports have examined IADL in persons with chronic thromboembolic pulmonary hypertension (CTEPH). The aim of this study was to clarify factors related to IADL in persons with CTEPH. This retrospective, observational study enrolled 163 persons with CTEPH (mean ± standard deviation age = 65 ± 13 years; 68% female) admitted to the Department of Cardiology at Keio University Hospital between January 2015 and July 2019. The Frenchay Activities Index (FAI) was used to assess IADL. Age, sex, body mass index, World Health Organization functional class (WHO-FC), cardiac function (mean pulmonary arterial pressure, mean right atrial pressure, pulmonary capillary wedge pressure, and cardiac index), pulmonary function (percentage vital capacity, percentage forced expiratory volume in 1 s, diffusion capacity of carbon monoxide (DLCO)/alveolar volume (VA)), physical function (knee extension strength and walking speed), and 6-min walking distance (6MWD) were assessed. Multiple regression analysis was performed to identify factors significantly associated with FAI. Mean FAI was 25 ± 8. Univariate analysis showed that sex, WHO-FC, DLCO/VA, walking speed, and 6MWD were correlated with FAI. Multiple regression analysis showed that 6MWD (sβ = 0.338, 95% CI 0.014–0.034, p < .001), sex (sβ = 0.268, 95% CI 2.238–7.165, p < .001), and DLCO/VA (sβ = 0.257, 95% CI 1.011–3.528, p < .001) were significantly correlated with FAI (R2 = 0.261). IADL were associated with exercise tolerance, sex, and DLCO/VA in persons with CTEPH. In the future, more details of IADL are expected to be clarified by analyzing individual components of IADL and investigating social background characteristics, including living environment.
Keywords
Introduction
Pulmonary hypertension (PH) is a refractory syndrome defined as a mean pulmonary arterial pressure (mPAP) ≥ 25 mmHg measured during right-heart catheterization at rest. 1 Early symptoms include shortness of breath, chest pain, and fainting. When severe, PH leads to right-heart failure, ascites, lower-leg edema, and anorexia. This is a relatively rare disease with nonspecific subjective symptoms and physical findings, so diagnosis often takes time.
PH occurs in each of the basic diseases in Dana Point classification groups 2, 3, and 5, and priority is given to the treatment of each basic disease. However, Group 1 pulmonary arterial hypertension (PAH) and Group 4 chronic thromboembolic pulmonary hypertension (CTEPH) have unknown causes, so disease-specific treatment is prioritized. CTEPH is a rare disease in which organizing thrombi chronically occlude the pulmonary arteries, causing the pulmonary artery pressure to increase. The median age of persons with CTEPH is in the 60s, and more than 70% are women in Japan. 2 Each group shows a poor prognosis, but survival has been prolonged due to advances in treatment techniques.3–6
Among elderly individuals, a decrease in instrumental activities of daily living (IADL), which are defined as representing a higher level of complexity than basic ADL, 7 is considered an important predictor of mortality, 8 and it is also associated with decreased quality of life (QOL). 9 In persons with heart disease, impaired IADL has also been reported as an important outcome predicting survival10–12 and the incidence of heart failure. 10 However, very few reports have examined IADL in persons with PH. In a previous report on ADL involving 37 persons with PAH and seven persons with CTEPH, World Health Organization functional class (WHO-FC) III and IV patients had significantly lower IADL scores evaluated by the Nottingham expansion activity index 13 than class I and II patients. 14 Clarification of tendencies in ADL in a large cohort with CTEPH from the perspective of prognosis is important, as described above. In addition, knowing the ADL and IADL status of persons with CTEPH and exploration of related factors are indispensable for investigating the effects of therapeutic intervention and planning targeted rehabilitation. IADL have been reported to be related to motor functions such as muscle strength, balance, and walking speed in healthy individuals,15,16 but there is also a report that respiratory function was related to ADL in persons with respiratory diseases. 17 It is necessary to examine these factors in the IADL of persons with CTEPH.
The purpose of this study was to clarify whether factors of cardiac and respiratory function, as well as motor function, are related to the decline in IADL of Japanese persons with CTEPH.
Materials and methods
Participants
A total of 163 persons with CTEPH referred to the Department of Cardiology at Keio University Hospital between January 2015 and July 2019 for diagnosis of CTEPH and examination by balloon pulmonary angioplasty were enrolled. All patients were diagnosed using right-heart catheterization (mPAP ≥ 25 mmHg at rest and pulmonary artery wedge pressure (PAWP) ≤ 15 mmHg), pulmonary ventilation/perfusion scintigraphy, pulmonary angiography, and chest CT. Patients with a history of previous BPA treatment (n = 4), history of multiple fainting episodes (n = 2), or inability to walk (n = 2) were excluded.
Background information
Age, sex, body mass index, and WHO-FC were extracted from medical records. For WHO-FC, classes I and II were classified as mild and classes III and IV, as severe. 14
Cardiac status
To evaluate cardiac function, mPAP, mean right arterial pressure (mRA), PAWP, cardiac index (CI), and pulmonary vascular resistance (PVR) were collected.
Respiratory status
To evaluate respiratory function, percent vital capacity (%VC), percent forced expiratory volume in 1 s (% FEV1.0), and diffusion capacity of carbon monoxide (DLCO)/alveolar volume (VA) were used.
Physical functions
Muscle strength of the lower limbs and comfortable walking speed were assessed. Isometric knee extension muscle strength using a hand-held dynamometer (μ-Tas F-1, Anima Corp, Tokyo, Japan) was used as an index of muscle strength. Patients sat on a chair without a backrest, and seat height was adjusted so that the soles were off the floor. The knee joint was extended to reach maximum muscle strength in about 2 s, and isometric movement was maintained for about 4–5 s. 18 Measurements were taken twice on the left and right, and the weight ratio was calculated after averaging maximum values. In addition, as an evaluation of walking speed, a 10-m walking test was conducted. 19 Patients stood at the start line and were asked to walk to the goal point 10 m ahead after a signal from the examiner, and the measurement was completed when either leg reached the goal point. Two measurements were performed, and the fastest value was used. After measurement, the speed (meters per second) was calculated.
IADL
IADL are more applied and multifaceted than basic activities of daily living and represent an essential component of living independently in the community. 7 IADL include applied and multifaceted aspects including activities such as housework, social occasion, and gainful work, whereas basic activities of daily include eating, changing clothes, and walking. A decline in IADL has been reported to be not only associated with decreased QOL, 9 but also a predictor of mortality. 8 The Frenchay Activities Index (FAI) was used to evaluate IADL. The FAI was developed in 1983 by Holbrook and Skilbeck to follow up IADL before, immediately after, and 1 year after stroke onset. 20 This index consists of 15 items, scored out of a total of 45. Each item is scored from 0 to 3 to see how often it is practiced, with 0 being “I don’t do it at all” and 3 being “I do it almost every day or at least once a week.” Factor analysis has been conducted for the FAI, and its reliability and validity have been verified. 21 The Japanese edition was revised by Hachisuka et al. so that it could be easily completed in 1999, 22 and the revised version has also been examined for reliability and validity. Reference scores for each age have been reported for Japan and other countries.23,24
Exercise tolerance
The 6-min walking test was used to evaluate exercise tolerance. Referring to the measurement characteristics and test protocols given by the European Respiratory Society/American Thoracic guideline,25,26 patients walked up and down a 30-m flat corridor, and the walking distance after 6 min was calculated. Before starting this study, subjective symptoms were observed on the new Borg scale, and heart rate and percutaneous arterial oxygen saturation (SpO2) were measured using a pulse oximeter. Discontinuation criteria were the same as those described in the guidelines, 26 such as chest pain, unbearable shortness of breath, and leg cramps. In addition, referring to previous studies, 26 the examiner provided instructions to suspend the test for SpO2 < 85%, even in the absence of subjective symptoms. When SpO2 was improved, a restart instruction was issued to ensure safety.
Analyses
In examining factors related to FAI, the Spearman test was performed for continuous data, and the Mann–Whitney U test was performed for categorical data (sex and WHO-FC). After that, multiple regression analysis (stepwise method) was performed for items identified as significant independent variables on single regression analysis.
For statistical analysis, SPSS version 21 (IBM Corp, Armonk, NY, USA) was used, and the criterion for significance was < 5%.
Ethical considerations
This research was based on the ethical principles described in the Declaration of Helsinki and the basic principles of the Ministry of Health, Labour and Welfare’s “Ethical Guidelines for Human Medical Research.” All research was conducted to ensure respect for the life, health, and human rights of subjects. The Ethics Review Board of Keio University Hospital approved the study protocol. All included patients provided their written, informed consent to participate in the study.
Results
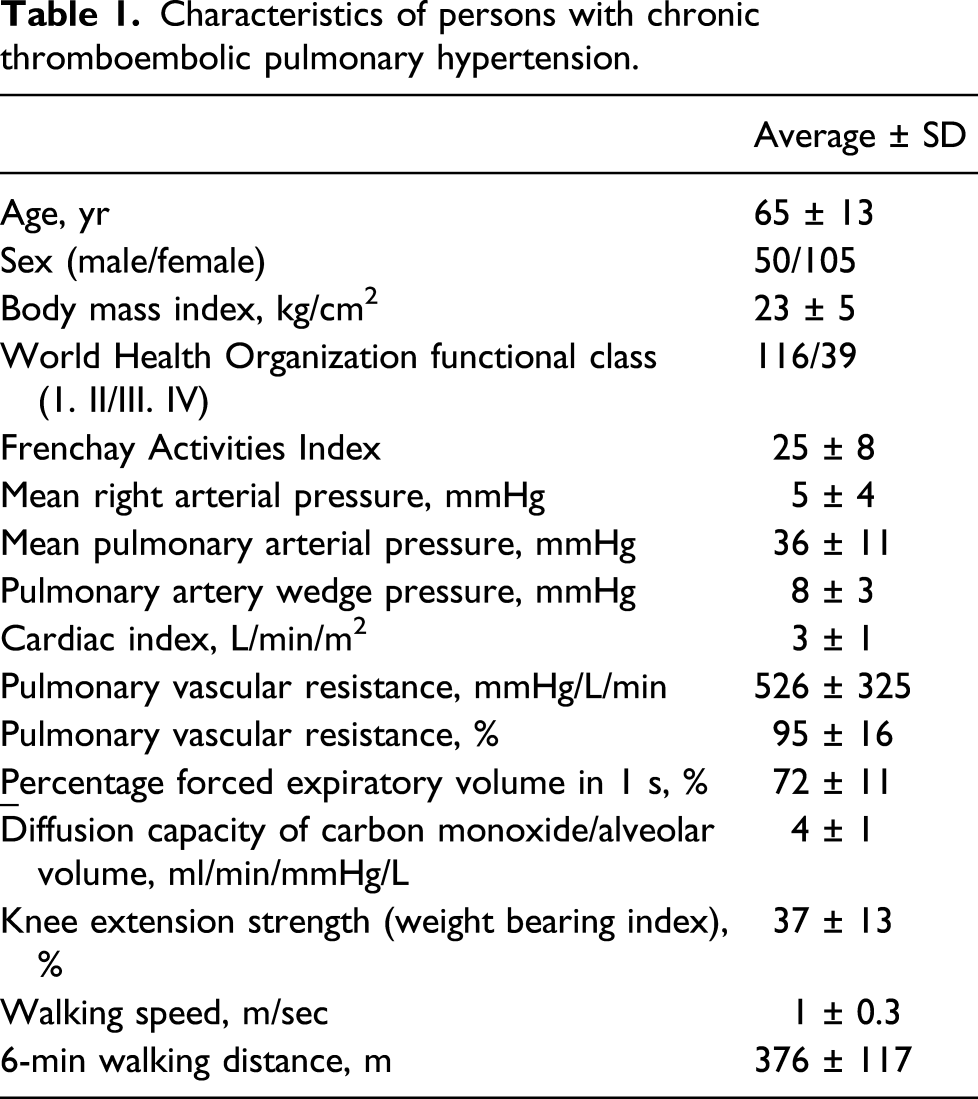
Characteristics of persons with chronic thromboembolic pulmonary hypertension.

Changes of FAI subscores (mean ± standard deviation). Scores tend to be higher for household affairs and items that can be performed outdoors with a light load, but lower for items with high physical load.
Spearman’s rank correlation coefficients between the Frenchay Activities Index and clinical variables.

Comparison of the Frenchay Activities Index (FAI) between groups and among categorized groups.

Multiple regression analysis of factors related to the Frenchay Activities Index.

R2 = 0.261.
Discussion
This is the first investigation of IADL in a relatively large sample of persons with CTEPH, representing possible candidates for balloon pulmonary angioplasty. Factors associated with IADL in persons with CTEPH were examined, and exercise tolerance, sex (female), and DLCO/VA were found to be significantly associated.
In Japan, patients in their 60s and 70s living at home had median FAI scores of 32 ± 6.5 and 30 ± 7.2. 24 By sex, in general middle-aged and elderly persons (mean age = 67.1±7.2 years), 22 the mean FAI score was 23.1 ± 8.5 for males and 29.4 ± 9.0 for females. The IADL score was thus lower in persons with CTEPH than in healthy individuals. Duration of physical activities > 3 METs is also known to be reduced in persons with PAH.27,28 A small number of persons with PAH and CTEPH, including previously treated patients, showed decreased physical activity at home, which reportedly shows a weak-to-moderate correlation with IADL. 14 Comparing the results between those of previous studies14,27,28 with our study, the IADL of persons with CTEPH may be reduced.
Among FAI subitems, travel, gardening, household maintenance, and gainful work showed low scores. In the assessment of IADL by FAI, if the score of an item is less than one, it means that the person being assessed performs that movement item very infrequently in daily life. The items that corresponded to housework were performed with a frequency comparable to that of healthy individuals, whereas the items for gardening, travel outings/car rides, and gainful work were found to be lower in persons with CTEPH (Supplemental Table 1). Because the exercise tolerance of persons with CTEPH is low compared to healthy adults,29,30 the frequency of performing these items may be decreased. Similar trends have been reported in patients with aortic stenosis, 31 and thus, they might represent a characteristic of heart disease. Strength might also contribute to the ability of these patients to remain physically active. Travel, household maintenance, and gainful work have the common feature of being systemic movements that not only involve moving long distances, but also include upper-limb movements. Gardening, on the other hand, is an activity that does not involve a lot of transfers, but is characterized by the posture and repeated standing and squatting when gardening. Previous studies have reported that maintaining an anterior trunk tilt posture increases residual volume 32 and increases abdominal pressure. 33 The squatting motion is considered to be burdensome for persons with CTEPH with decreased DLCO/VA and who are prone to respiratory distress.
On multivariate analysis, 6MWD, female sex, and DLCO/VA were associated with IADL. As in previous reports, 6MWD was lower in persons with CTEPH than in healthy individuals.29,30 This result may suggest a decrease in exercise tolerance in persons with CTEPH. A correlation between exercise tolerance assessed by 6MWD and ADL or IADL has been reported in various diseases, including persons with PAH and COPD.14,34 In persons with CTEPH, it was also reasonable that 6MWD was a determinant of IADL.
Next, sex was also identified as a related item, and the FAI was higher in women than in men. Regarding the relationship with sex, the FAI score in women has been shown to be as high as that in healthy adults22–24 and those with stroke. 35 Generally, among the various physical activities, women reportedly perform more household chores than men. 36 FAI includes more items related to housework, and women are reportedly more likely to do housework as healthy adults, 22 so persons with CTEPH are considered similar. Thus, sex differences in IADL may be substantially affected by differences in roles at home. On the other hand, female sex has been reported as a risk factor for decreased IADL in the general elderly population > 75 years old 37 and in elderly persons with heart failure. 38 Although the mean age of the study population was relatively young (65 years), the mean life expectancy of persons with CTEPH is increasing, and the age of persons with CTEPH is expected to continue to increase in the future. Sex differences in IADL will need to be examined in a sample that also includes older patients.
Finally, DLCO/VA was identified as a relevant factor reflecting respiratory function. In the PH guidelines, 39 evaluation of respiratory function is important for diagnosis and prognosis. DLCO/VA reflects lung diffusion function and is reportedly decreased in persons with COPD or PH.40,41 Factors that define DLCO/VA include (1) the alveolar capillary membrane, (2) the gas exchange area, (3) pulmonary capillary blood volume, (4) blood hemoglobin concentration, and (5) uneven ventilation/perfusion (V/Q) mismatching. In patients with PH, a decrease in V/Q mismatch inequality is a characteristic pathological condition that is associated with shortness of breath on exertion. 42 In patients with emphysema, exacerbation of DLCO/VA is considered to be associated with limited ADL, 17 and persons with CTEPH may also show impaired respiratory function.
The limitations of this study include its cross-sectional, single-center nature, and a lack of information on social background characteristics such as living environment and roles at home. In addition, prospective cohort studies are needed in the future. The existence and frequency of social participation are important factors in considering IADL. 43 Furthermore, subjective evaluations of health, decreased QOL, and presence of depression are also considered to be related to disordered IADL, 44 and information on home environment due to the presence of cohabitants, differences between urban and suburban households, and cultural sex-related issues such as gender roles must also be considered.
Despite these limitations, this study should be useful in understanding the structure of IADL, reflecting the actual situation of IADL among persons with CTEPH and relationships with cardiopulmonary and motor functions.
Conclusion
Persons with CTEPH may have reduced IADL, and IADL as assessed by the FAI were associated with exercise tolerance, sex, and DLCO/VA. These results are useful when considering interventions to improve IADL in patients.
Supplemental Material
sj-pdf-1-crd-10.1177_14799731211046634 – Supplemental Material for Factors related to instrumental activities of daily living in persons with chronic thromboembolic pulmonary hypertension
Supplemental Material, sj-pdf-1-crd-10.1177_14799731211046634 for Factors related to instrumental activities of daily living in persons with chronic thromboembolic pulmonary hypertension by Tatsuya Iwasawa, Shogo Fukui, Michiyuki Kawakami, Takashi Kawakami, Masaharu Kataoka, Shinsuke Yuasa, Keiichi Fukuda, Toshiyuki Fujiwara and Tetsuya Tsuji in Chronic Respiratory Disease
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.