
Abstract
The most important long-term complication of pulmonary thromboembolism is chronic thromboembolic pulmonary hypertension (CTEPH) that is associated with considerable morbidity and mortality. It is uncertain why some patients with acute pulmonary embolism (PE) develop CTEPH and others do not. Elevated red cell distribution width (RDW) has been associated with adverse outcomes of heart failure, PE, and idiopathic pulmonary hypertension. The aim of the present study was to investigate whether RDW might be a predictor of CTEPH in PE patients or not. This study is a retrospective cohort study. A total of 203 consecutive patients with acute PE were included. The RDW was higher in the CTEPH patients than the patients without CTEPH (17.04 ± 3.46, 14.64 ± 1.82, respectively, p = 0.015). RDW was also higher in the CTEPH patients at the time of diagnosis of CTEPH during follow-up compared with the baseline RDW level at the time of PE diagnosis (18.63 ± 3.58, 17.02 ± 3.59, respectively, p = 0.014). The optimal cutoff value of the RDW for predicting CTEPH was 14.65. The area under the curve of RDW for the prediction of CTEPH was 0.735 (95% confidence interval (CI): 0.600–0.869); in cases with RDW levels >14.65%, the specificity, sensitivity, and negative predictive value for CTEPH were 62% (95% CI: 0.55–0.69), 75% (95% CI: 0.47–0.92), and 96.7% (95% CI: 0.91–0.99), respectively. A multivariate regression analysis showed that RDW, hazard ratio: 1.58 (95% CI: 1.09–2.30), was a predictor of CTEPH (p = 0.016). High level of RDW was an independent predictor of CTEPH in PE patients. Therefore, RDW levels may provide a prediction for CTEPH in PE patients.
Keywords
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) has been known as a relatively rare complication of pulmonary embolism (PE) but has been reported to be associated with considerable morbidity and mortality. 1,2 Although the incidence of CTEPH is usually estimated to be <1% among patients with acute PE, 2 –4 several studies have proposed that this low incidence was an underestimation and showed approximately 4%, a relatively high incidence of CTEPH after PE. 5 –7 In addition, it has not been shown why some PE patients develop CTEPH and others do not. The observation that the majority of acute PE patients do not go on to develop CTEPH suggests that there are actually other factors that are important in the development CTEPH. 2 Therefore, it is important to determine the possible risk factors and/or predictors for the CTEPH in patients with PE in order to decrease the morbidity and mortality of CTEPH.
Red cell distribution width (RDW) has been measured as a part of the hemogram and quantifies the variability in the size of red blood cells. RDW has been shown to predict survival in patients with pulmonary hypertension of mixed etiologies 8 and in patients with idiopathic pulmonary hypertension. 9 It has also been recently reported to be associated with early mortality and prognosis in patients with acute PE. 10,11
The aim of the present study was to investigate whether RDW could be a possible predictor for CTEPH in patients with PE.
Materials and methods
Study design
The present study was a retrospective cohort study, and the investigation conforms to the principles outlined in the Declaration of Helsinki. The study was approved by the local ethics committee. The study was conducted at a university hospital, a tertiary care hospital that serves as a primary referral center for patients with suspected PE. The timescale of the present study was from January 2006 to November 2009 with retrospectively available computer-based database of the patients with suspected PE. Patients diagnosed with PE for the first time were included in the calculation of the frequency of CTEPH. PE patients with malignancies, anemia, or left heart failure (HF) were excluded from the study because these parameters have been known to increase the RDW. 12 The median follow-up period was 27 months (interquartile range: 12–44 months). RDW levels were collected at the first episode of the PE and during follow-up period at the time of CTEPH diagnosis.
Patients and settings
The patients’ demographic characteristics, clinical, and laboratory parameters were obtained from the hospital electronic database and chart reviews. The demographic characteristics of the PE patients and the laboratory findings were recorded to include all that were thought to be potential risk factors for CTEPH and PE. These included its localization and the spread of the thrombus, initial management techniques, systolic pulmonary arterial pressure on echocardiography and accompanying deep vein thrombosis during an acute event, comorbidities of the patients, and a previous history of venous thromboembolism (VTE).
Diagnosis of PE and CTEPH
All the consecutive cases were diagnosed with acute PE objectively and confirmed using computed tomography pulmonary angiography or high-probability pulmonary perfusion scintigraphy, or medium-probability perfusion scintigraphy in the presence of deep vein thrombosis by Doppler ultrasonography.
The diagnosis of CTEPH was established by chest x-ray, transthoracic echocardiography (ECHO), pulmonary function tests including arterial blood gas analysis and ventilation–perfusion scans of the lungs, and computed tomography pulmonary angiography scans were carried out during the follow-up period of symptomatic PE patients to check for CTEPH. ECHO examinations were performed with a two-dimensional, conventional, tissue Doppler ECHO on a Vivid 7 system (GE Vingmed Ultrasound, Horten, Norway) with a 3.4 MHz transducer probe. The value of systolic pulmonary arterial pressure (sPAP) >35 mm Hg at rest with Doppler ECHO was regarded as CTEPH condition. 13
Confirmation of CTEPH was made by the detection of an organized thrombus occluding the pulmonary arteries completely, and/or eccentrically and/or concentrically, and/or by the presence of a mosaic perfusion picture in the parenchyma with reduced vascular calibration in distal regions (variations in the size of lobe and segmental-level vessels) and dilatation of pulmonary artery at computed tomography pulmonary angiography scans. 14,15 Patients without any other pathology that might be a cause for the pulmonary hypertension were evaluated for CTEPH using a ventilation perfusion scan of the lungs. The diagnosis of CTEPH was excluded in the case of normal or low-probability perfusion scintigraphy that has been previously described. 13,16
Biochemical analysis
We used complete blood counts (CBCs) obtained at the time the PE patient was presented for the analysis. The baseline RDW was measured using a Beckman Coulter Automated CBC Analyzer (Beckman Coulter Inc., Fullerton, Miami, Florida, USA). The normal reference value for RDW in our laboratory was between 11.6 and 16.5%.
Statistical analysis
The Kolmogorov–Smirnov test was used to test for normal distribution of continuous variables. Data characterized by a normal distribution were expressed as mean values followed by standard deviation. Parameters without such a distribution were expressed as a median with range. Student’s t test (normal distribution) or Mann–Whitney test (nonnormal distribution) was used to compare the two groups. The investigation for a diagnostic cutoff value was based on receiver-operating characteristic curves. Multivariate regression analysis was used in a stepwise descending method from prognostic factors with significance <0.1 at univariable analysis. Results are given as odds ratios (95% confidence interval (CI)), and p < 0.05 was considered statistically significant. Data were analyzed using Statistical Package for the Social Sciences (SPSS; Version 13.01, serial number 9069728, SPSS Inc., Chicago, Illinois, USA).
Results
A total of 203 patients with PE were included in the study (Figure 1 for consort diagram). Of the total study population (n = 203), 100 patients with PE were examined using ECHO performed in an emergency setting within 24 hours of admission. Then, 138 patients with unresolved or partially resolved breathlessness were evaluated with follow-up ECHO for possible CTEPH. All the patients were evaluated for the deep vein thrombosis clinically, and 96 patients of them were evaluated for deep vein thrombosis with ultrasonography. There were 16 patients with CTEPH. Patient demographics and clinical characteristics at study entry were reported in Table 1. Individual data for each CTEPH patient were shown in Table 2. The means RDW was higher in CTEPH patients than in patients without CTEPH (17.04 ± 3.46%, 14.64 ± 1.82%; p = 0.015). The optimal cutoff value of RDW for predicting CTEPH was 14.65. The area under the curve of RDW for prediction of CTEPH was 0.735 (95% CI: 0.600–0.869) (Figure 2). In cases with RDW levels >14.65, the specificity and sensitivity of CTEPH were 62% (95% CI: 0.55–0.69) and 75% (95% CI: 0.47–0.92), respectively. The negative predictive value of RDW at cutoff 14.65 for CTEPH was 96.7% (95% CI: 0.91–0.99), and the positive predictive value of RDW at cutoff 14.65 for CTEPH was 14.4% (95% CI: 0.08–0.24). RDW was also higher in the CTEPH patients at the time of diagnosis of CTEPH during follow-up compared with the baseline RDW level of CTEPH patients at the time of initial PE diagnosis (18.63 ± 3.58, 17.02 ± 3.59, respectively; p = 0.014; Figure 3). Cumulative incidence of CTEPH in our cohort was higher in PE patients stratified by the RDW level at cutoff level of 14.65 (14.5%, n = 12 vs. 3.3%, n = 4; Figure 4).

Consort diagram showing flow of participants in the study.
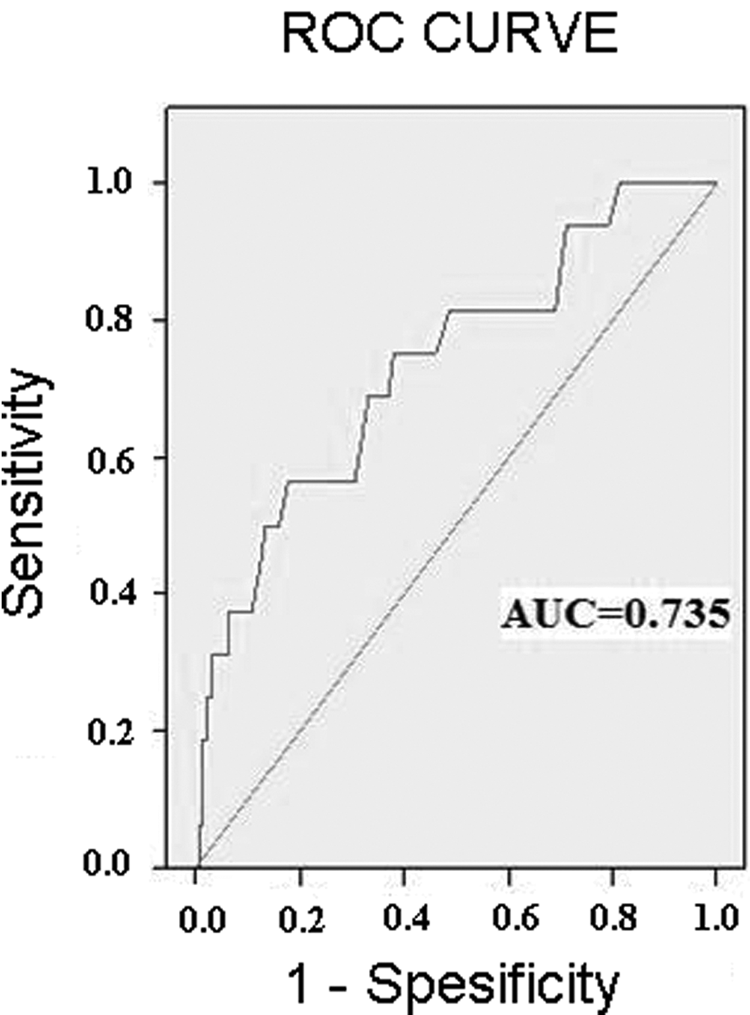
Receiver-operating characteristic curves for RDW of PE patients to predict CTEPH. RDW: red cell distribution width; PE: pulmonary embolism; CTEPH: chronic thromboembolic pulmonary hypertension.

Comparison between RDW levels of CTEPH patients at the time of diagnosis during follow-up and the baseline RDW level of CTEPH patients at the time of initial PE diagnosis. RDW: red cell distribution width; CTEPH: chronic thromboembolic pulmonary hypertension; PE: pulmonary embolism.

Cumulative incidence of CTEPH in the study cohort stratified by the RDW level at the cutoff level of 14.65. CTEPH: chronic thromboembolic pulmonary hypertension; RDW: red cell distribution width.
Clinical features and demographical characteristics of the patients.

CTEPH: chronic thromboembolic pulmonary hypertension; RDW: red cell distribution width; PE: pulmonary embolism; sPAP: systolic pulmonary arterial pressure; VTE: venous thromboembolism.
Individual data for each CTEPH patient.

CTEPH: chronic thromboembolic pulmonary hypertension; PE: pulmonary embolism; VTE: venous thromboembolism; V/P: ventilation/perfusion; CT: computed tomography; sPAP: systolic pulmonary arterial pressure; ECHO: echocardiography; RDW: red cell distribution width.
aThese patients had contrast nephropathy risk factors and they were diagnosed with symptoms; V/P scan and echocardiography were used instead of CT angiography for CTEPH.
In univariate analysis, a significant association was found between CTEPH development and age, history of VTE, initial sPAP, idiopathic PE, uric acid, and RDW (Table 3).
Risk factors for the prediction of symptomatic CTEPH in univariate analysis.

CTEPH: chronic thromboembolic pulmonary hypertension; OR: odds ratio; CI: confidence interval; CRP: C-reactive protein; sPAP: systolic pulmonary arterial pressure; VTE: venous thromboembolism; PE: pulmonary embolism; RDW: red cell distribution width.
A multivariate regression analysis showed that RDW, hazard ratio (HR): 1.58 (95% CI: 1.09–2.30), was a predictor of CTEPH (p = 0.016). Other potential predictors for CTEPH at multivariate regression analysis are summarized in Table 4.
Predictors of symptomatic CTEPH in multivariate analysis.
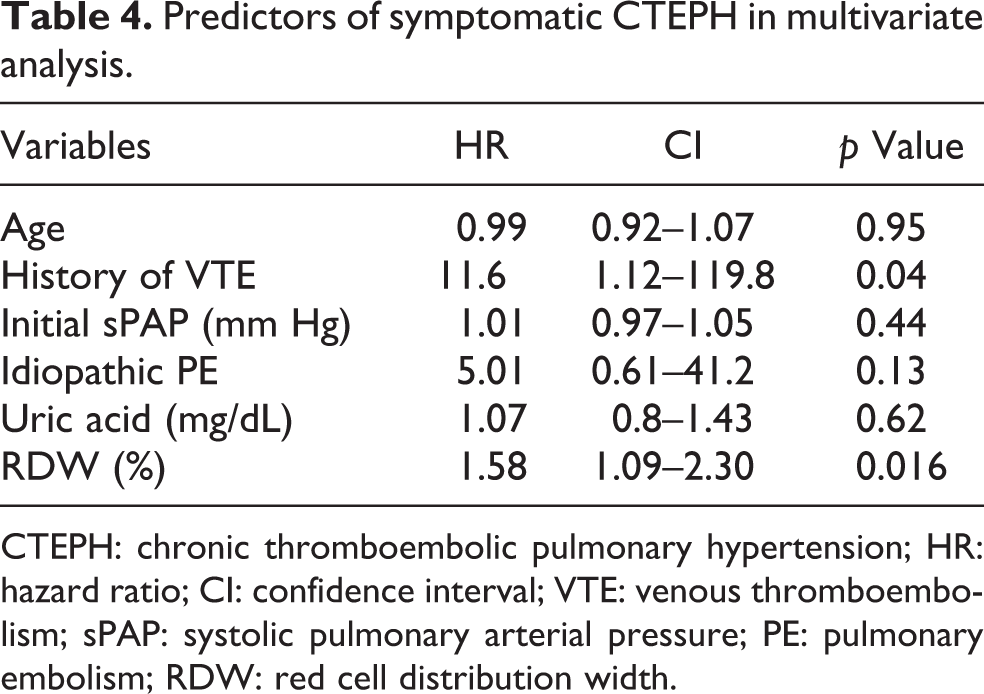
CTEPH: chronic thromboembolic pulmonary hypertension; HR: hazard ratio; CI: confidence interval; VTE: venous thromboembolism; sPAP: systolic pulmonary arterial pressure; PE: pulmonary embolism; RDW: red cell distribution width.
Discussion
CTEPH has been known as one of the leading causes of severe pulmonary hypertension. CTEPH is often underdiagnosed, and its exact prevalence is obscure. Also, the pathogenesis of the disease is not been clearly understood, and risk factors attributed to the occurrence of CTEPH still remain poorly defined. Intraluminal in situ thrombus, fibrous stenosis, and total obliteration of pulmonary arteries by pulmonary arteriopathy are characteristic features of CTEPH. 5,17 –19 The risk for the development of CTEPH is increased when PE is detected in young or old age having large perfusion defects, during recurrent or unprovoked (idiopathic) PE, when pulmonary artery systolic pressure is >50 mm Hg at initial manifestation of PE, and when there is persistent pulmonary hypertension on ECHO performed 6 months after acute PE is detected. 5,20 –22 CTEPH condition occurs due to chronic medical risk factors that lead to the development of chronic inflammatory disorders such as osteomyelitis and inflammatory bowel disease, myeloproliferative syndromes, the presence of a ventriculoatrial shunt, and splenectomy. 23 Based on the similarities with these chronic medical conditions and on available data, one may speculate that chronic inflammatory processes are involved in the pathogenesis of CTEPH. 24 This hypothesis is augmented by some studies showing that inflammation may cause a prothrombotic state by reducing the resolution of pulmonary thromboemboli, and CTEPH has some common features with focal and systemic inflammation. 25 –27
The RDW is a routinely and an easily measured parameter as a part of CBC and has recently been shown to be associated with cardiovascular disease, PE, pulmonary hypertension, and obstructive sleep apnea. 8,10,28 –31 It has been proposed that during HF, RDW levels have some features in common with a combination of chronic inflammation and oxidative stress. 32 Both RDW and CTEPH have some common features from the point of inflammation. For these reasons, RDW may reflect multiple factors related to the association with the pulmonary hypertension. Inflammation is a component of pulmonary hypertension and particularly interleukin 6 has been linked to the development of pulmonary hypertension in experimental models. 33,34 Oxidative stress and inflammation have been proposed as the important determinants of RDW and its association with cardiopulmonary thrombotic diseases. 12 The role of inflammation in CTEPH pathogenesis has been emphasized in studies illustrating the expression of the C-reactive protein receptor lectin-type oxidized low-density lipoprotein receptor 1 on cells isolated from the major pulmonary vessels in CTEPH. 35 From the point of chronic inflammatory processes that are involved in the pathogenesis of CTEPH, RDW may potentially reflect the inflammatory status in CTEPH. Release of inflammatory cytokines that may affect bone marrow function and erythrocyte maturation, which is induced by erythropoietin, is inhibited therefore this process may lead increased RDW. 8,10,30 Chronic cardiopulmonary diseases have an association with nutritional deficiencies, comorbid diseases, and deterioration of renal function. As a result of these conditions, RDW may also increase. 29,36 All these mechanisms might be proposed for the elevation of RDW in pulmonary vascular diseases particularly in CTEPH.
There has been an increase in the use of RDW in literature, and it has been proposed as a useful parameter for predicting mortality in patients with acute and chronic HF, 37 –39 PE, 10 and pulmonary arterial hypertension. 30 Its association is mostly independent of hemoglobin and hematocrit levels in these studies. Some studies have shown that higher RDW values are also related to an increased risk of mortality in the general population. 40 Zorlu et al. evaluated 136 consecutive patients with acute PE prospectively. 10 An RDW cutoff value of 14.6% predicted early mortality with 95% sensitivity and 53% specificity in their study. They also found that RDW values of 14.6% on admission had prognostic significance in a univariate Cox proportional hazards analysis (HR of 15 for early mortality). 10 The present study also found an RDW cutoff value of 14.65% to predict CTEPH in PE patients with 62% sensitivity and 75% specificity. One important finding of the present study is the negative predictive value of RDW at cutoff 14.65 that was 96.7%. Of course, this negative predictive value could not be solely used to exclude CTEPH during PE follow-up. Besides clinical symptoms, ECHO, and radiology, low level of RDW might provide additional diagnostic information. RDW levels of patients with CTEPH were not only high at the beginning of PE diagnosis retrospectively but also high at the time of CTEPH diagnosis during follow-up period compared with the baseline RDW levels of these patients at the initial PE diagnosis. Therefore, high levels of RDW at the beginning of PE diagnosis and persistent high level of RDW during follow-up could alert the physician about CTEPH in PE patients. On the other hand, there is also a limitation about the ECHO, because ECHO largely depends on the experience of the operator and accurate identification of pulmonary hypertension, which needs an expert cardiologist in ECHO. Measuring and following up the RDW levels could also contribute to the prediction of CTEPH especially in intermediate and high-risk patients with acute PE besides using ECHO especially when the right heart catheterization is not readily available or not easily performed for these patients.
CTEPH patients present with progressive dyspnea and exercise intolerance. These symptoms may be caused by various conditions including coronary heart disease, HF, obstructive lung diseases, and interstitial lung disease. Although the initial diagnostic evaluation indicates that the potential cause of the progressive dyspnea and exercise intolerance is pulmonary hypertension, the many different types of pulmonary hypertension should be considered as the alternative possible diagnoses. Aftertaking a detailed history and conducting physical examination, patients with symptoms and signs of pulmonary hypertension and with a confirmed PE history should be evaluated for CTEPH with the use of imaging procedures. High RDW level could contribute to the evaluation of the patients suspected to have CTEPH besides ECHO, ventilation perfusion scan, and computed tomography angiography. Besides all the clinical, echocardiographical, and radiological diagnostic tools, high RDW level may provide an awareness about the CTEPH during early and late follow-ups in PE patients.
This study has various limitations. The first is that pulmonary hypertension was diagnosed using ECHO rather than pulmonary artery catheterization. However, an sPAP value > 50 mm Hg (sPAP > 60 mm Hg in approximately 90% of CTEPH cases) was measured in all the CTEPH-developing cases. In addition, there is a powerful correlation between sPAP > 50 mm Hg at ECHO and by pulmonary catheterization. 13 Moreover, in all patients, PE was confirmed again at least twice by individuals unaware of each other’s conclusions. On the other hand, we do not know the number of asymptomatic cases. However, these patients are frequently reported to be diagnosed after becoming symptomatic and the clinical significance is debatable. In addition, asymptomatic CTEPH is not an uncommon finding after PE. 6 Although the present study was retrospective, CTEPH was diagnosed with ECHO and scintigraphy findings and chronic thrombus by computerized tomography angiography. Moreover, PE was diagnosed with computerized tomography angiography in 98% of cases. Our results can therefore be accepted as objective. The second limitation is that although we did not include the PE patients with low hemoglobin levels, which influence RDW values, in the study, we do not know the previous exact medical history of the study population in terms of whether they had been treated for iron deficiency anemia or not, and this also interferes with the RDW values due to the retrospective cohort. The study design is retrospective; therefore, prospective randomized controlled studies will be better for showing this association more precisely. The third limitation is that the incidence of chronic thromboembolic hypertension was found to be a higher percentage in this study because we did not include the PE patients with low hemoglobin levels and also, to prevent bias, we did not include the patients with malignancies and HF, and these have been shown to increase RDW level in previous studies. 12
In conclusion, high RDW levels are an independent predictor of CTEPH in PE patients. Therefore, RDW levels may be used as a potential marker to predict CTEPH in PE patients. Further prospective studies are needed to provide additional information about this association especially in CTEPH patients diagnosed by right heart catheterization.
Footnotes
Acknowledgment
The authors thank Prof. RW Guillery from the University of Oxford, UK, for correcting the language part of this article.
Authors’ Note
This article was presented at the European Respiratory Society Annual Congress 2012 held at Vienna, Austria, during 1–5 September 2012.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.