
Abstract
High-flow nasal cannula (HFNC) therapy has been increasingly applied to treat patients with severe hypoxemic respiratory failure. We investigated whether vital signs reflect the reduction of work of breathing in a simulator study and a clinical study. In the simulator study, a standard model high-fidelity human patient simulator (HPS) directly received 35 L/minute of 100% O2 via the HFNC. In the clinical study, the medical records of patients with hypoxemic respiratory failure who received HFNC therapy between January 2013 and May 2015 were retrospectively reviewed. Statistical analysis was performed using a one-way repeated analysis of variance followed by Bonferroni post-hoc testing. In the HPS, HFNC therapy significantly reduced the partial pressure of alveolar CO2, respiratory rate, and tidal volume (p < 0.001), and all values returned to baseline following HFNC therapy termination (p < 0.001). In the clinical study including 48 patients, the respiratory rate was significantly reduced from 27 ± 9 (baseline) to 24 ± 8 (3 hours), 24 ± 8 (5 hours), and 24 ± 8.0 (6 hours) (p < 0.05). The heart rate also decreased significantly (p < 0.05). Our results suggested that HFNC therapy reduced work of breathing and assessing vital signs can be important.
Keywords
Introduction
Although first developed for use in neonates, 1 high-flow nasal cannula (HFNC) therapy is currently used to avoid endotracheal intubation in patients with severe hypoxemic respiratory failure. 2 Several clinical trials targeting critical patients have been performed, and HFNC therapy seems beneficial in patients with nonhypercapnic acute hypoxemic respiratory failure, 3 hypoxemic patients after cardiothoracic surgery, 4 and post-extubated patients with low risk for reintubation. 5 HFNC therapy has already been widely applied in immunocompromised patients, 6 but clinical evidence is still not enough whether HFNC therapy is superior to noninvasive ventilation in immunocompromised patients. 7 –9 A recent cross-sectional multicenter survey in Japan 10 reported that HFNC therapy was applied in an elderly population with moderate-to-severe respiratory failure, including a number of do-not-intubate (DNI) patients. HFNC therapy is applicable not only to patients in the intensive care unit (ICU) that appears in highly selected clinical trials, but also to patients with DNI disorder, 11 as an alternative O2 therapy to reduce suffering at the end of life.
The potential beneficial effects of HFNC are as follows: (1) administration of a constant fraction of inspired O2 (FIO2), (2) generation of positive end-expiratory pressure (PEEP), (3) reduction of the anatomical dead space, (4) improvement of mucociliary clearance, and (5) decreased work of breathing. 1 Most of the previous studies were performed to address generation of PEEP and decreased work of breathing, because PEEP was measureable 12 and decreased work of breathing can be evaluated by electrical impedance tomography, respiratory rate, or the tidal volume (V T) 13 even in the clinical setting. Although the mechanism seems reasonable, it is difficult to elucidate whether HFNC washes the expired volume of CO2 from the airway, particularly in the clinical setting.
In this study, we aimed to investigate the beneficial effects of HFNC therapy in the reduction work of breathing. We tested whether vital signs such as respiratory rate and heart rate reflect the reduction of work of breathing in a simulator study and a clinical study.
Methods
Study design and data collection
Simulator study
As previously described, 14 a standard model high-fidelity human patient simulator (HPS; CAE Healthcare, Sarasota, Florida, USA) computerized to simulate the physiology of a 33-year-old male with a weight of 70 kg and height of 182 cm was used. To mimic spontaneous breathing, bellows generate negative pressure in the model lung of the simulator (Figure 1). 15 The gases inside the model lung were drawn out every 5 seconds at a rate of 3 L/minute and the partial pressure of O2 (PAO2) and CO2 (PACO2) was measured. A volume of O2 equivalent to the O2 consumption was extracted, and a volume of CO2 equivalent to the CO2 consumption was added. These mixed gases were returned into the model lung as exhalation gases. The initial settings of the component of returned gases during inspiration of room air were PAO2, 110 mmHg; PACO2, 40 mmHg; and vapor pressure, 0 mmHg. The initial settings of the respiratory variables of this model were V T, 700 mL and respiratory rate, 14 breaths/minute. The gases inside the model lung were measured, while other parameters were calculated.

Illustrating the mechanism of the respiratory system of the high-fidelity HPS. Movement of the bellows creates negative pressure inside the model lung of the simulator and mimics spontaneous breathing. The gases mixed inside the model lung were drawn out continuously at a rate of 3 L/minute, and the partial pressure of O2, CO2, and N2 were measured directly (PAO2, PACO2, and PAN2, respectively). PaO2 was calculated by a formula included in the rate of pulmonary venous shunt. The partial pressure of O2, CO2, and N2 that represent exhalation gases were calculated and the mixed gases were returned to the model lung at a rate of 3 L/minute. The initial settings of the component of exhalation gases were maintained at 110 mmHg PAO2 and 40 mmHg PACO2 during inspiration of room air. HFNC: high-flow nasal cannula; HPS: human patient simulator.
Adjustable respiratory parameters included in the HPS were: (1) metabolic CO2 production, (2) O2 consumption (default 200 mL/minute), (3) the end-tidal CO2 relative to the PaCO2 (default 1), (4) an influence of PaCO2 on V T and respiratory rate, (5) baseline respiratory rate and V T, (6) respiratory quotient (default 0.8), (7) V T/respiratory rate control to changes in arterial oxygen tension, and (8) shunt fraction (default 0.02). These values were adjusted to maintain the PACO2 at a set point of 40 mmHg as default. These parameters can be adjusted according to the desired scenario.
In this study, after 10 minute spontaneous respiration of room air, the HPS directly received O2 via the HFNC, which supplied 100% O2 at a flow rate of 35 L/minute. The actual measurements of PACO2, respiratory rate, and V T were recorded every 5 seconds for 3 minutes. After 3 minutes of inhalation, the HFNC was withdrawn, and the actual measurements of PACO2, respiratory rate, and V T were recorded every 5 seconds for the next 3 minutes. These procedures were repeated six times.
Clinical study
The clinical study was a retrospective study conducted at Kyorin University Hospital (Tokyo, Japan), that is, an educational hospital with an advanced emergency medical service center. Kyorin University Hospital has 1125 beds and more than 2000 ambulatory patients come daily. The study protocol was approved by our Institutional Review Board on Human Research (H27-043). Written informed consent was not required, as this was an observational retrospective cohort study. The study period was between January 2013 and May 2015.
Patients with hypoxemic respiratory failure who received HFNC therapy in the ICU or high dependency unit (HDU) during the study period were enrolled in this study. During the study period, HFNC therapy was restricted to use only in the ICU or HDU, and our respiratory support team (RST) had recorded all patients who received HFNC therapy. An anesthesiologist who did not belong to the RST retrospectively collected clinical data from the ICU medical and nursing charts and the hospital database. For HFNC therapy, O2 was delivered via Optiflow (Fisher & Paykel, Aukland, New Zealand). The flow rate and FIO2 were set by the attending physician, based on the patient’s condition. Patients aged <15 years were excluded. In addition, because we used the O2 saturation/FIO2 ratio (S/F ratio) as an index of the O2 status, patients with a peripheral capillary O2 saturation (SpO2) of ≥97% or S/F ratio of ≥315 before and after connection to the HFNC were excluded, because the oxyhemoglobin dissociation curve is flat above these levels. 16 From these patients, we collected data regarding patient age and sex, previous performance status, vital signs, lactate levels upon ICU (or HDU) admission, ICU (or HDU) length of stay, and ICU (or HDU) hospital mortalities. With the exception of hospital mortality, all of these data were included in the ICU medical and nursing charts. Hospital mortality rates were collected from the hospital database. The heart rate, respiratory rate, and SpO2 collected at 0, 1, 2, 3, 4, 5, and 6 hours following the initiation of HFNC therapy were compared to evaluate the beneficial effects of HFNC on vital signs.
Statistical analyses
Data are expressed as the mean ± standard deviation and median ± interquartile range (IQR) for normally and non-normally distributed continuous data, respectively. Statistical analyses were performed using a one-way repeated analysis of variance followed by the Bonferroni post-hoc test. All statistical analyses were conducted with EZR (Saitama Medical Center, Jichi Medical University, Omiya, Japan), which is a graphical user interface for R (R Foundation for Statistical Computing, v3.1.1). 17 The level of significance was set at p = 0.05.
Results
Simulator study
Figure 2(a) illustrates the changes in PACO2, Figure 2(b) illustrates the respiratory rate, and Figure 2(c) illustrates the V T following the initiation and termination of HFNC therapy. The PACO2, respiratory rate, and V T were significantly decreased 3 minutes after the initiation of HFNC therapy (p < 0.001). These values significantly increased following the termination of HFNC therapy (p < 0.001). These results suggested that the beneficial effects of HFNC therapy were evident in the normal setting of the HPS model.

Changes in the partial pressure of CO2, respiratory rate, and tidal volume following the initiation and termination of HFNC therapy. After stabilization with room air, the HPS directly received 100% O2 at a flow rate of 35 L/minute. (a) The partial pressure of CO2 (PACO2), (b) respiratory rate, and (c) tidal volume (V T) were recorded every 5 seconds for 3 minutes. After stabilization, O2 was withdrawn, and each parameter was recorded every 5 seconds for 3 minutes (n = 6). Values are plotted every 15 seconds. *p < 0.05, † p < 0.01, ‡ p < 0.005, and § p < 0.001 compared with the value at time 0 by the Bonferroni post-hoc test. HFNC: high-flow nasal cannula; HPS: human patient simulator.
Clinical study
During the study period, the RST recorded 110 patients who received HFNC at our ICU or HDU. Among the 110 patients, 1 was excluded because they were aged <15 years and 59 were excluded because their O2 status was not so severe (SpO2 of ≥97% or S/F ratio of ≥315). Finally, 48 patients fulfilled our study criteria. The chief causes of acute respiratory failure before and after application of the exclusion criteria (SpO2 of ≥97% or S/F ratio of ≥315) are provided in Table 1. Although the most frequent cause of HFNC therapy was pneumonia (28%), pulmonary fibrosis became the most frequent cause (40%) when we excluded patients with an SpO2 of ≥97% or S/F ratio of ≥315. Baseline characteristics and outcome of the 48 patients are summarized in Table 2.
Chief causes of acute respiratory failure among patients who received high-flow nasal cannula therapy.
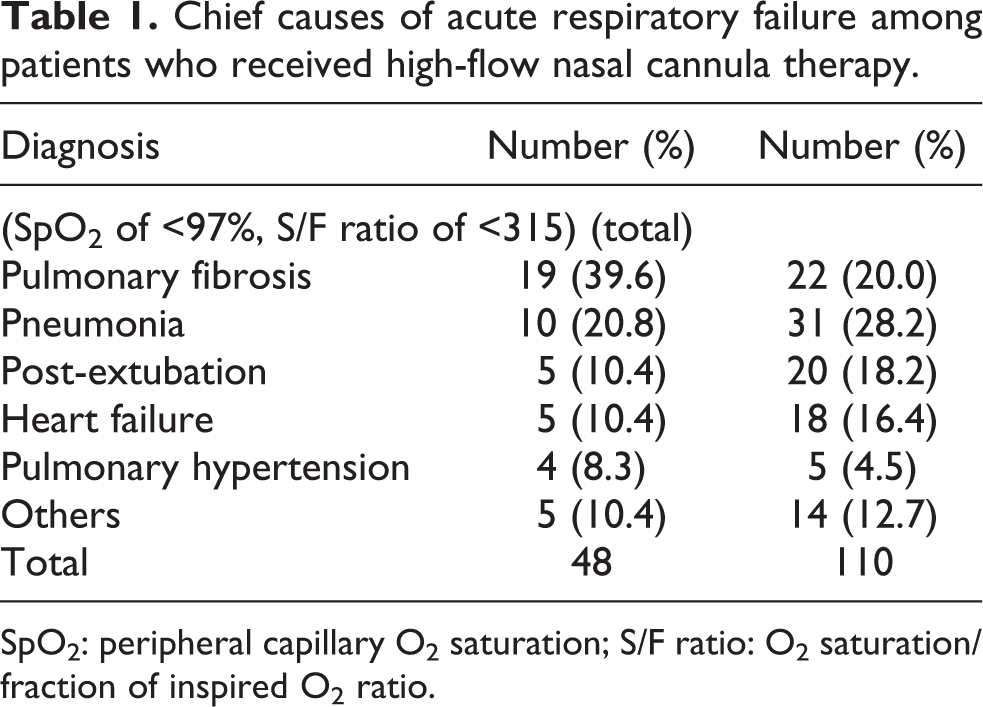
SpO2: peripheral capillary O2 saturation; S/F ratio: O2 saturation/fraction of inspired O2 ratio.
Baseline characteristics and outcome of the 48 patients enrolled in this study characteristics.

IQR: interquartile range; APACHE: acute physiology and chronic health evaluation.
As indicated in Figure 3(a), the respiratory rate significantly decreased from 27 ± 9 (baseline) to 24 ± 8 (3 hours), 24 ± 8 (5 hours), and 24 ± 8 (6 hours; p < 0.05). The heart rate also decreased significantly from 100 ± 21 (0 hours; before HFNC) to 97 ± 21 (1 hours), 94 ± 19 (2 hours), 97 ± 19 (3 hours), and 93 ± 20 (6 hours; p < 0.05; Figure 3(c)). These results suggested that the use of HFNC maintained significant reductions in the respiratory rate and heart rate for 6 hours. In comparison, changes in the S/F ratio did not reach statistical significance (Figure 3(b)).

(a) Changes in the respiratory rate, (b) O2 saturation/fraction of inspired O2 ratio, and (c) heart rate at 0, 1, 2, 3, 4, 5, and 6 hours following initiation of HFNC therapy. Among 110 patients who received HFNC therapy, 48 had a peripheral capillary O2 saturation (SpO2) of <97% or O2 saturation/fraction of inspired O2 ratio (S/F ratio) of <315. In these patients, the respiratory rate, S/F ratio, and heart rate at 0, 1, 2, 3, 4, 5, and 6 hours following initiation of HFNC were compared. Data are expressed as the means ± standard deviation. *p < 0.05 compared to the baseline value by one-way repeated measures analysis of variance followed by the Bonferroni post-hoc test. HFNC: high-flow nasal cannula.
Discussion
Key findings
We investigated the beneficial effects of HFNC therapy in the reduction of work of breathing in a simulator study and a clinical study. In the simulator study using a standard model simulator of a healthy male, we demonstrated that HFNC therapy reduced the PACO2, respiratory rate, and V T simultaneously. In the clinical study, we demonstrated that HFNC therapy reduced the respiratory rate and heart rate, while oxygenation as assessed by the S/F ratio did not change. Notably, these variables remained reduced for 6 hours. These results suggested that HFNC therapy reduced work of breathing, and the HPS reproduced respiratory physiology in the clinical setting. Because respiratory rate, V T and PACO2 were all reduced simultaneously in the HPS, we speculate that HFNC therapy exerts washout effects on the end-tidal CO2, and these washout effects contributed to the reduced work of breathing.
Relationship to previous studies
Clinical studies have reported the favorable effects of HFNC therapy in hypercapnic patients in the reduction of hypercapnia via reduction of the anatomical dead space, resulting in decreased V T and respiratory rate, while keeping PaCO2 unchanged or reduced. In a randomized study, Rittayamai et al. 18 reported that HFNC therapy reduced breathing frequency and heart rate compared to Venturi mask O2 therapy in post-extubation patients, while the O2 saturation did not change. Maggiore et al. 19 reported that the use of an HFNC resulted in improved oxygenation, reduced respiratory rates, and reduced PaCO2 for the initial 48 hours of the post-extubation period compared to Venturi mask O2 therapy. In a prospective study including 77 chronic obstructive pulmonary disease (COPD) patients undergoing long-term O2 treatments, Vogelsinger et al. 20 reported that short-term use of an HFNC was safe in normocapnic and hypercapnic COPD patients and reduced hypercapnia and the O2 consumption. In their study, HFNC therapy reduced the PaCO2, while conventional O2 therapy slightly increased the PaCO2, during their 1 hour observation period. Mauri et al. 21 studied 17 non-intubated patients with acute hypoxemic respiratory failure and found that while the HFNC flow rate progressively reduced the inspiratory effort, CO2 clearance was achieved within 20 minutes of their application period of 30 L/minute of HFNC therapy. Bräunlich et al. 22 reported that 8 hours exposure to nasal high-flow breathing (20 L/minute) significantly reduced the respiratory rate, minute volume, and capillary PCO2 in patients with COPD and idiopathic pulmonary fibrosis. Peters et al. 11 reported that application of HFNC therapy for 1 hour significantly reduced the breathing frequency and increased the O2 saturation in 50 DNI patients with hypoxemic respiratory distress who were admitted to the ICU. Our data from the HPS are consistent with these clinical results, and the HPS well reproduced respiratory physiology in the clinical setting.
Significance and implications
In our clinical study, HFNC therapy reduced the respiratory rate and heart rate. Notably, we observed a longer duration of effects, and these variables remained reduced for 6 hours. In comparison, oxygenation as assessed by the S/F ratio did not change. Because of the limitation of a retrospective observational study, collected parameters on respiratory function were limited in the clinical study. Therefore, to evaluate the beneficial effects of HFNC by respiratory physiology, we conducted the simulator study that yielded parameters of respiratory function minute by minute. Combined with the fact that V T and respiratory rate were reduced in the simulation study, we speculate that the main reason for the reduced respiratory rate was the washout effect of anatomical dead space, rather than the respiratory support effects of generating PEEP. Therefore, assessing vital signs is important when applying HFNC therapy to patients with severe respiratory failure, rather than taking arterial blood samples repeatedly.
In this study, our HPS clearly reproduced the beneficial effects of HFNC on vital signs that were noninvasively measurable in the clinical situation. Decreased PaCO2 may add physiological grounds on the increasing usage of HFNC in obstructive lung diseases with caution due to the concern that it would increase the PaCO2. Because HPS is based on respiratory physiology, we interpreted that we would expect drops of the heart rate and respiratory rate by the sixth hour. In a post-hoc analysis of a prospectively assessed cohort of adult patients with H1N1 pneumonitis, Rello et al. 23 showed that HFNC therapy could demonstrate its failure or success by 6 hours after onset of treatment, while failing patients demonstrated worse oxygenation. These results may suggest that it may be beneficial in the clinical setting to observe vital signs carefully at least for 6 hours, to judge failure or success of HFNC therapy. In cases when these beneficial effects are not observed, the condition of the patient should be closely followed to decide about escalation of therapy.
Strengths and limitations
There are several limitations to discuss in relation to this study. First, in the clinical study, oxygenation was assessed by the S/F ratio, not the arterial pressure of O2/FIO2 ratio (P/F ratio), because most of the patients did not undergo blood gas analysis measurement while receiving HFNC therapy. Although the S/F ratio has been demonstrated to be useful, 16 the gold standard for assessing oxygenation is the P/F ratio. However, because HFNC therapy is not invasive for patients, physicians tend to avoid taking blood samples and observe the patient’s O2 status using the SpO2. Selecting patients with severe hypoxemia (patients with an SpO2 of ≥97% or S/F ratio of ≥315 were excluded) might have been one reason why HFNC therapy did not improve oxygenation.
Second, the relevancy of HPS study to clinical situations was limited. The HPS lacked to reproduce the beneficial role of warm and moist oxygen and patient comfort and work of breathing. 1 In addition, the mechanism underlying the reduced V T in the simulation study was unclear. In humans, HFNC therapy has been demonstrated to increase the V T. Because the PACO2 significantly decreased, we concluded that the washout effect of HFNC reduced the PACO2, and resulted in a reduced minute volume, respiratory rate, and V T. We speculated that the reduced V T could be observed only in the simulation study.
Conclusion
In conclusion, we demonstrated that HFNC therapy reduced work of breathing in the clinical study, and the HPS well reproduced respiratory physiology in the clinical setting. Because the respiratory rate and minute volume were reduced simultaneously, we speculate that the anatomical dead space was reduced by HFNC therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by MEXT KAKENHI grant number JP15K10544.