
Abstract
There is no accepted standard for measuring mobility in hospitalized patients with an acute exacerbation of chronic obstructive pulmonary disease (AECOPD). The objective of this study was to assess convergent, discriminant, and known-group validity and floor/ceiling effects of the de Morton Mobility Index (DEMMI) in hospitalized patients with AECOPD. Individuals with AECOPD (n = 22) admitted to an acute care hospital medical ward were recruited. Data on the DEMMI, gait speed, daytime energy expenditure, step counts, 6-minute walk distance (6MWD), dyspnea, respiratory and heart rates, quality of life, and oxygen supplementation were collected on day 3 of admission. The DEMMI demonstrated convergent validity with the 6MWD and gait velocity measures (Spearman’s ρ 0.69 and 0.61, respectively; p < 0.003) but not with measures of physical activity or respiratory impairment. Discriminant validity was present, with no correlation between the DEMMI and quality of life and resting heart rate. Known-group validity (gait aids vs. no gait aids) was demonstrated (p = 0.009). There was no floor effect but there was evidence of a possible ceiling effect (14% of participants received a perfect score). The DEMMI is feasible and showed moderate to strong validity with measures of observed physical function in hospitalized patients with AECOPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by frequent exacerbations known as acute exacerbations of COPD (AECOPD), often resulting in lengthy hospitalizations. 1 Decreased physical activity is common in AECOPD 2,3 and is a risk factor for readmission. Individuals who are active 60 minutes per day have a 50% reduced risk of readmission after discharge from hospital with an AECOPD. 4 Physical inactivity is also highly related to increased mortality, even after adjusting for severity of lung disease and oxygen use. 5
Hospitalized patients with an AECOPD are inactive. Pitta et al. 2 reported that hospitalized patients with COPD spend most of their day sitting. One month post-AECOPD, time spent sitting had not decreased back to baseline levels. Several investigators have reported low functional capacity in hospitalized AECOPD patients, with 6-minute walk test values ranging from 218 m to 300 m. 6 –8 Little is known about the specific mobility limitations of hospitalized patients with AECOPD. It is important to know whether problems with mobility impact physical activity and which aspects of mobility are affected. There is no accepted standard for measuring mobility in hospitalized patients with AECOPD. Indeed, Oliveira and Marques 9 recently reported the lack of consensus related to outcomes, noting numerous different outcome measures have been used in studies of hospitalized AECOPD patients, although few related to mobility. There is a need for valid measures in this population to develop appropriate, individualized mobilization exercises as part of an inpatient rehabilitation program. The de Morton Mobility Index (DEMMI) is a hierarchical, 15-item observed assessment of mobility. It is a reliable measure for hospital populations 10 that has been validated in acute, 11 subacute, 12 and community 13 adult patient groups, but not specifically in inpatients with AECOPD. This population is unique because mobility limitations in AECOPD may be due to respiratory impairments, such as severe dyspnea or oxygen desaturation, as well as musculoskeletal factors. It is necessary to assess the validity, feasibility, and minimal clinically important difference (MCID) of the DEMMI in hospitalized AECOPD populations prior to recommending its use by physiotherapists in an acute care rehabilitation setting. Therefore, the objectives of this study were (1) to assess the convergent, discriminant, and known-group validity of the DEMMI in a hospitalized AECOPD population and (2) to assess the feasibility of using the tool in terms of floor and ceiling effects. We also calculated a preliminary estimate of the MCID of the DEMMI in the AECOPD inpatient population.
Methods
Study design and participant selection
This study was conducted in a university teaching hospital in Vancouver, Canada. Consecutive patients admitted to hospital with an AECOPD were recruited. All measures were taken at day 3 of the hospital admission. Eligible patients were individuals (1) with a physician diagnosis and/or spirometric evidence of COPD (post-bronchodilator forced expiratory volume, first second (FEV1) to forced vital capacity (FVC) ratio less than 0.70), (2) admitted to an acute care ward from the patient’s primary residence for an AECOPD, according to the physician notes in the hospital chart, (3) with no intubation or invasive ventilation as part of the current admission, and (4) who were able to understand verbal English instructions. Patients were excluded if they (1) were unable to give informed consent, (2) were confused or agitated, or (3) had activity contraindicated. Ethical approval was obtained from the Providence Health Research Institute/University of British Columbia (certificate # 11-00960) and all patients provided written informed consent.
Study procedure
Participants with an AECOPD were identified on day 2 of their admission. Once consent was obtained, information on age, gender, prior use of gait aids, and comorbidities were collected from the hospital chart. On the morning of day 3, participants completed the questionnaires and had their height, weight, and resting heart rate, respiratory rate, blood pressure, and oxygen saturation measured. The DEMMI, gait speed, and 6-minute walk distance (6MWD) tests were then conducted followed by 24-hour measurement of energy expenditure and physical activity.
Measurements
de Morton Mobility Index
Each participant underwent a DEMMI mobility assessment 14 by a trained physiotherapist on day 3. The 15 tests of mobility in the DEMMI tool are divided into five categories: (1) bed—“roll onto side,” “bridge,” and “lying to sitting”; (2) chair—“sit unsupported in chair,” “sit to stand from chair,” and “sit to stand without using arms”; (3) static balance (no gait aid)—“stand unsupported,” “stand feet together,” “stand on toes,” and “tandem stand with eyes closed”; (4) walking—“walking distance +/− gait aid,” “walking independence”; and (5) dynamic balance (no gait aid)—“pick up pen from floor,” “walks 4 steps backwards,” and “jump.” The test takes approximately 15 minutes to administer. Depending on the task, the physiotherapist scored a “0,” “1,” or “2,” with higher scores indicating greater independence with mobility. The scores for all tasks were summed and then converted to a DEMMI score with a possible range of 0–100. The DEMMI tool and details on administration and scoring can be downloaded here:
https://ahsri.uow.edu.au/content/groups/public/@web/@chsd/@aroc/documents/doc/uow234573.pdf
Gait velocity and 6MWD tests
Gait velocity was measured over a 4-m unobstructed corridor with a 2-m acceleration and deceleration area. 15 Participants walked at a usual pace between two marked points using walking aids if necessary. Two measurements were performed and the highest value retained.
The 6-minute walk test was performed using an internal hallway with a marked distance of 40 m according to American Thoracic Society standards. 16 Standardized encouragements were applied during the tests. Participants used their walking aids and those on supplemental oxygen had assistance carrying the tank during the test. Heart rate and saturation were recorded at one minute intervals during the test. The Borg dyspnea scale 17 and blood pressure were measured at the beginning and end of the test.
Physical activity and energy expenditure
Physical activity was evaluated with an activity monitor (SenseWear, BodyMedia, Pittsburgh, Pennsylvania, USA), which has been previously validated in COPD. 18 The SenseWear device was placed on the participant’s arm after the physical tests were completed and worn for 24 hours. A 24-hour recording period was chosen as it was anticipated that physical activity would increase with each day of hospital admission, and we aimed to estimate physical activity in the time period closest to the measurement of mobility. The variables recorded from the SenseWear device were duration on body (hours), daytime energy expenditure between 7:00 a.m. and 9:00 p.m. (when physical activity was most likely to be encouraged), and the total number of steps.
Health-related quality of life
Each participant completed the St George’s Respiratory Questionnaire, 19 a 50-item health-related quality of life questionnaire that is valid in COPD. The items are then scored on a scale of 0–100 for three domains—symptoms, activities, and impact—and a total score. A higher score indicates worse quality of life.
Statistical analysis
Patient characteristics are described using means and standard deviations or counts and proportions, where appropriate. Relationships between continuous variables were graphically represented using scatterplots. Spearman’s ρ calculations were used to estimate correlations. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, North Carolina, USA). A sample size of 19 individuals was required to detect with 80% power a correlation coefficient of 0.60 with an α < 0.05.
Convergent validity
To assess convergent validity, we hypothesized there would be significant correlations between the DEMMI score and the measures of physical function (6MWD, gait velocity, total steps, and daytime energy expenditure) and measures of respiratory impairment (dyspnea at rest and during exercise, respiratory rate, and the need of supplemental oxygen).
Discriminant validity
To assess discriminant validity, we hypothesized there would be no significant correlation between the DEMMI score and resting heart rate or quality of life.
Known-group validity
We assessed known-group validity using independent t-tests to compare DEMMI scores between patients who used no gait aids versus those who needed a walker or a cane.
Floor and ceiling effects and MCID estimate
Similar to other studies, 20,21 we determined a floor or ceiling effect was present if 15% of the population scored the lowest or highest DEMMI score, respectively. We also assessed the proportion of the population who achieved the highest possible score for each of the five individual DEMMI domains, as in a clinical setting, the physiotherapist would also consider domain-specific limitations when creating an individualized rehabilitation program. We calculated a preliminary estimate of the MCID, using the method recommended by Norman et al. 22 and used in other DEMMI validity studies, 13,14,21 in which the MCID is estimated by dividing in half the baseline standard deviation of the DEMMI score.
Results
Participant recruitment
Figure 1 illustrates the study flowchart. Ninety-six patients were hospitalized with a primary diagnosis of AECOPD between March 2012 and December 2013 and were screened for eligibility. Thirty-eight individuals did not meet the inclusion criteria (including 13 who had physician-ordered bed rest due to medical instability), and 36 participants declined participation, were unable to participate due to clinical schedule of tests and treatments, or were discharged before day 3, leaving 22 participants enrolled in the study.
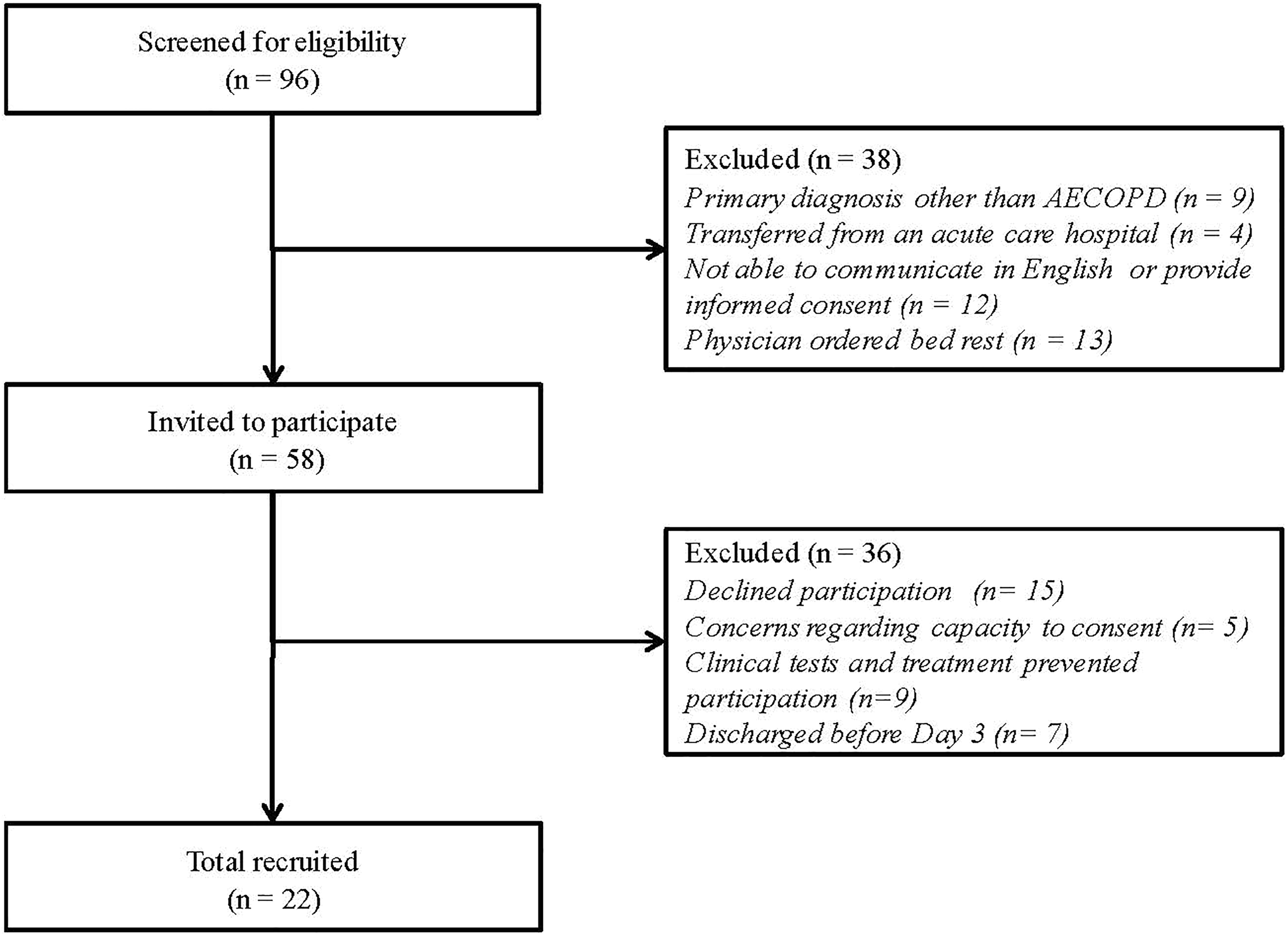
Study of flowchart.
Participant characteristics
Table 1 reports the characteristics of study population. They were predominantly male, with a mean age of 60 (standard deviation (SD) 10) years, and a 34 (SD 18) pack-year smoking history. Sixty-four percent of the participants were active smokers. Prior spirometry tests were available for 73% of the sample, with the remainder having tests done while hospitalized. Spirometry results indicated moderate to severe airflow obstruction. Sixty-four percent of the participants had a previous history of a cardiovascular, musculoskeletal, and/or neuropsychiatric comorbidity. Forty-six percent of the population used a gait aid prior to admission. The mean length of hospital stay for the current AECOPD was 7 (SD 4.5) days.
Characteristics of the participants.

SD: standard deviation; kg: kilogram; m: meter; FEV1: forced expiratory volume, first second; FVC: forced vital capacity; SGRQ: St George’s Respiratory Questionnaire; 6MWD: 6-minute walk distance; IQR: interquartile range.
DEMMI scores and feasibility of the measure
Figure 2(a) shows the distribution of DEMMI scores. The mean DEMMI score was 70 (SD 20) and was normally distributed (p = 0.10). No participant had a DEMMI score of 0, indicating there was no floor effect and the measure was feasible to use in this population. Fourteen percent of participants achieved a score of 100. Within the bed, chair, static balance, walking, and dynamic balance domains, 77%, 95%, 14%, 50%, and 73% of participants, respectively, achieved a perfect score.

DEMMI score frequency diistribution and relationships with measures of validity.
Validity
Figure 2(b) to (h) and Table 2 show correlation coefficients and selected scatterplots between the total DEMMI score and the 6MWD, gait velocity, total daily steps, total waking energy expenditure, Borg dyspnea score at rest, Borg dyspnea score during exercise, and respiratory rate at rest (for convergent validity; between the DEMMI and resting heart rate and quality of life (for discriminant validity); and between the DEMMI and gait aid use (for known group validity). The scatterplot and statistical analysis indicated that there were significant moderate to strong correlations between the DEMMI score and the 6MWD and the gait velocity. The scatterplots and correlation coefficients between the DEMMI and variables related to physical activity, energy expenditure, and respiratory impairment were not significant. Evidence of discriminant validity was present with no correlation detected between the total DEMMI score and quality of life or heart rate at rest. Known-group validity was demonstrated as there was a significant difference in DEMMI score between those who used a gait aid on admission versus those who did not (p = 0.009).
Validity of the DEMMI.

DEMMI: de Morton Mobility Index; TEE: total energy expenditure; HR: heart rate; SGRQ: St George’s Respiratory Questionnaire; SD: standard deviation.
A preliminary estimate of the MCID was calculated to be 10 DEMMI points.
Discussion
In this study, we examined validity, floor, and ceiling effects and calculated a preliminary MCID of the DEMMI in a population of hospitalized individuals with AECOPD. The DEMMI showed moderate to strong validity with measures of physical function, specifically 6MWD and gait velocity. This finding was in agreement with validity studies of the DEMMI in other populations. de Morton and Lane 12 reported a correlation coefficient of −0.69 (p < 0.01) between the DEMMI and the time to walk 6 m, and a correlation coefficient of 0.57 (p = 0.06) for the 6MWD in 40–80 patients in an inpatient geriatric rehabilitation hospital. The preliminary estimate of the MCID of 10 DEMMI points was similar to that reported by de Morton et al. in a general acute care population (MCID = 10 points) 14 and an older community population (MCID = 11 points). 13 It was higher than the MCID reported by de Morton and Lane 12 in a subacute geriatric hospital population (MCID = 6 points), which may be attributed to our younger demographic.
Contrary to our hypothesis, there was no relationship between the DEMMI and measures of daytime physical activity. The examination of the scatter plots identified many individuals with high DEMMI scores (>70 points) who were extremely inactive during the day. The high correlation observed between the DEMMI and the 6MWD and gait velocity, but not with measures of daytime physical activity is likely due to the fact that 6MWD and gait velocity are tests of physical function conducted by a health-care professional, whereas steps taken and daytime energy expenditure assess actual physical activity in the day, which is impacted by many factors (e.g. personal choice, available supervision and equipment, and physical space) beyond physical ability.
In addition, there was also no relationship between the DEMMI and dyspnea, respiratory rate, and the need for oxygen supplementation. This was despite the understanding that increased dyspnea and dynamic hyperinflation are associated with a lower 6MWD 23 and associated respiratory symptoms limit walking and other forms of exercise in COPD. 24 This finding may not be evidence of poor validity of the DEMMI tool, as there was also no relationship between dyspnea ratings and 6MWD in this sample (data not shown). It would appear that although patients reported high levels of dyspnea, had a high respiratory rate, or required supplemental oxygen, these factors did not impact their capacity to be mobile at the levels required in the hospital setting.
In this population, the DEMMI demonstrated known-group validity. This finding was similar to other studies. 11,20,21,25 There was no evidence of a floor effect, although we did not test patients until day 3 of their hospital stay as most physical therapy referrals occur at day 2 or 3 of an admission. Fourteen percent of the population achieved a perfect DEMMI score. While this amount did not achieve our predetermined threshold of 15%, it still indicates that a sizable proportion of the AECOPD population may not have limitations in mobility which can be detected by the DEMMI. It is important to note that two of the three participants who had a perfect DEMMI score had low 6MWD and gait velocity values. Further work on DEMMI ceiling effects in a larger sample of patients is warranted.
We also reported the proportion of individuals who achieved perfect scores within each DEMMI domain. Previous studies have not reported on domain-specific mobility. While the tool is meant to provide an overall quantitative mobility score for use as an outcome measure, it may be helpful for physiotherapists to use the tool to characterize within-domain limitations in mobility. This qualitative use of the DEMMI has not been validated, but future research could determine if targeted, individualized inpatient physiotherapy interventions based on limitations in specific DEMMI domains could result in better patient outcomes. These interventions could include screening for specific limitations, setting goals of therapy, and discharge planning.
There were some limitations to the study. We calculated our sample size based on the validity analysis, which required a sample of 19 individuals for adequate power. However, the possibility of a DEMMI ceiling effect in this group could not be confirmed or denied in this study. In addition, this study was conducted with patients who were younger (mean age 60 years) than typical AECOPD populations. Although the mean DEMMI score was similar to other reports, this younger group may be more mobile than older patients and a sampling bias may be present. Some patients who met the initial criteria of the study were discharged before day 3, also indicating a less severe AECOPD cohort. However, there was a sizable proportion of screened patients (14%) who did not meet the study eligibility as they were on physician-ordered bed rest when screened for the study. Inclusion of these more frail patients may have impacted our results. The feasibility and psychometric properties of the DEMMI in older, more frail AECOPD patients have yet to be determined.
We used the SenseWear triaxial accelerometer to assess steps and physical activity. The SenseWear is less accurate in slowly walking individuals, 18,26 which may have underestimated the relationship between the DEMMI score and step counts. We selected the 6MWT, the 4-m gait speed test, and measures of physical activity to address aspects of validity. Other functional tests, such as the Timed Up and Go, or the Short Performance Battery Scale, also address elements of mobility and could have yielded a different result.
The MCID was calculated using the distribution-based method on a small sample. Using an anchor-based method may provide results that are more comparable across studies. Calculating an MCID using a larger sample of AECOPD inpatients with a greater variation of age and disease severity, combined with responsiveness data, is recommended.
Conclusion
In this study of AECOPD patients, the DEMMI was found to have good convergent, discriminant, and known-group validity related to measures of observed physical function and is an appropriate measure of mobility for physiotherapists’ and other health-care professionals’ use in the acute care setting. Future research should focus on the use of the DEMMI as an assessment and outcome measure for inpatient pulmonary rehabilitation, including physical therapy and mobility interventions, for individuals with AECOPD. Further work on understanding the DEMMI reliability, predictive properties, and responsiveness on important outcomes, such as readmission rates and physical activity post-discharge, is warranted.
Footnotes
Authors' Note
Jessica A Inskip is now employed by Roche Canada Ltd.
Acknowledgment
We would like to acknowledge physiotherapist Mary Carlsen, who conducted the DEMMI assessments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Respiratory Health Professionals and from the Physiotherapy Foundation of Canada. PC is a Michael Smith Foundation for Health Research Career Scholar.