
Abstract
The aim of the study is to explore the experiences of inpatients with an acute exacerbation of chronic obstructive pulmonary disease, who participated in a very early exercise programme while acutely unwell. This qualitative study analysed responses from participant interviews as part of a mixed method trial whereby participants were randomly allocated into three groups: low intensity, moderate to high intensity aerobic and resistance exercises or a control group who received routine physiotherapy. Everyone allocated to the exercise groups were invited to participate in the qualitative study. Interviews were within a week post discharge and the results were analysed thematically. A total of 19 participants were interviewed and described their experience as positive and beneficial and reported an increased motivation towards exercising. These findings converged with the high levels of exercise adherence (83%) and within-group improvements in walking capacity observed in both exercise groups. Participants also reported commencement of a home exercise programme after discharge but intention to participate in community pulmonary rehabilitation remained low. Participation in a very early exercise programme while acutely unwell can lead to positive attitude towards exercise. The results converge with the quantitative results that provided preliminary evidence of programme feasibility and within-group improvement in exercise tolerance.
Keywords
Introduction
Exercise is a primary and integral non-pharmacological approach in the management of patients with stable chronic obstructive pulmonary disease (COPD). 1–3 Implementing an exercise programme for people with COPD while their condition is stable has been demonstrated to improve exercise tolerance, quality of life and reduce hospital readmissions. 1–4 However, an acute exacerbation of COPD requiring hospitalisation has been shown to have detrimental effects on exercise capacity, muscle strength and physical activity levels for people with COPD. 5–7 Declines in these parameters have also been associated with increase in mortality risk and morbidity among people with COPD. 8,9
However, getting people with COPD to exercise can be challenging. Patients are often hesitant to participate in pulmonary rehabilitation, being concerned that the exercise component of pulmonary rehabilitation would increase their shortness of breath. 10 A recent survey conducted among people with COPD revealed that 26% of people associated participation in strenuous activity with exacerbation of their COPD condition and were reluctant to exercise. 11 Perhaps related to these concerns, the adherence rate to exercise classes for people with COPD remains low, 12,13 despite the known positive effects of exercise for this population.
In a recent phase one randomised controlled trial, an exercise programme based on the principles of pulmonary rehabilitation was implemented with people requiring hospitalisation for an acute exacerbation of COPD and was found to be safe and feasible 14 Another trial demonstrated that implementation of a quadriceps strengthening exercise programme for patients requiring hospitalisation for an acute exacerbation of COPD was effective in preventing quadriceps muscle deterioration. 15 These programmes were conducted while patients were medically unwell and symptomatic from their acute exacerbation.
The quantitative results of these trials were promising and suggested that very early exercise during an exacerbation of COPD may be safe and feasible and therefore have the potential to address the detrimental effects of hospitalisation in this population. 14,15 However, they did not report participants’ perceptions of the programme nor their attitudes towards exercising when unwell. In light of the challenges of adherence and negative perceptions of pulmonary rehabilitation during stable COPD, an exercise programme implemented when acutely unwell with significant increases in dyspnoea may reinforce any negative perceptions of exercise. This may in turn negatively impact on uptake and adherence to community pulmonary rehabilitation, especially if patients perceived exercising not to be beneficial for their COPD condition.
Therefore, the aims of this study were to use a qualitative research design to explore people’s attitudes and experiences towards participation in an exercise programme when acutely unwell and whether this early exercise programme experiences changed perceptions about ongoing exercise and attendance to pulmonary rehabilitation following discharge.
Methods
This article reported on the findings of a qualitative study completed as part of a mixed-methods trial. The findings were briefly discussed in relation to those coming from the randomised controlled trial 14,16 The lack of previous studies investigating experiences and perceptions of people with COPD exercising while acutely unwell meant that we did not have preconceived judgements thereby allowing us to appropriately adopt the phenomenology approach to explore the lived experience of exercising while unwell. 17
Participants
Participants were recruited from a sample of people involved in the randomised controlled trial. 14 Purposive sampling strategies were used to obtain rich and meaningful information from the interviews. 17 Participants were included if they had been admitted to hospital with an acute exacerbation of COPD, recruited in the randomised controlled trial and allocated to the exercise groups and were able to attend an interview session following hospital discharge. Patients allocated to the control group in the randomised controlled trial were not invited to participate. Written informed consent to participate in the interview was obtained from each participant prior to commencement of the trial. The study received approval from the ethics committees of Eastern Health – Maroondah Hospital (E59-0809) and La Trobe University (FHEC 08/191).
Procedure
Semi-structured interviews were used to obtain rich thick descriptions of the participants’ perception, experience and attitude towards the exercise programme. 18 Participants were given an interview time prior discharge from hospital and a choice between face-to-face and phone interview, as each mode of interview has its merits. 19 All interviews were completed within a week of discharge from hospital to increase the likelihood of participants having a clear recollection of the programme.
Each interview was conducted by a clinician who had previous experience in conducting semi-structured interviews and did not have any previous contact with the participants. This allowed participants to be comfortable to express their unbiased opinions.
Intervention
The exercise rehabilitation programme involved supervised twice-daily 15 minutes physiotherapy sessions that included both resistance and aerobic training from the second day of admission to hospital till the day of discharge in addition to standard physiotherapy treatment. Full details of the programme are described elsewhere. 14 Depending on allocation, participants were either required to exercise at a low intensity (40% maximal intensity) or at a moderate to high intensity (70% maximal intensity). Aerobic intensity was based on the results of 3-minute walk test at baseline, while strengthening intensity was based on repetitions maximum. All participants were given a copy of the exercise programme and a resistance band at time of discharge and were encouraged to continue their exercise programme at home.
Data analysis
All interviews were audiotaped and transcribed verbatim. Credibility of the study was addressed by the use of member checking for all transcripts to maximise the accuracy of the responses. Once the transcribed transcript had been checked, all identifiable information was removed from the transcript and the participants were assigned a participant identity number to ensure anonymity.
Qualitative software, NVIVO (QSR, Melbourne, Australia) was used to assist with the management of data. The process of assigning open codes was completed on all transcribed transcripts by two researchers independently (CYT and FCB). The codes provided an insightful meaning to the data and to establish any new relationships within the common exercise experience. 17 Codes were then analysed and compared, creating links between a category and subcategories. Finally, an analysis on all categories and subcategories was completed to find the main theme that linked all other categories together. The thematic analysis allowed us to formulate any possible themes from the interview transcripts without being influenced by any preconceived judgements. These themes were compared with the findings of the randomised controlled trial to explore for any convergence of the themes.
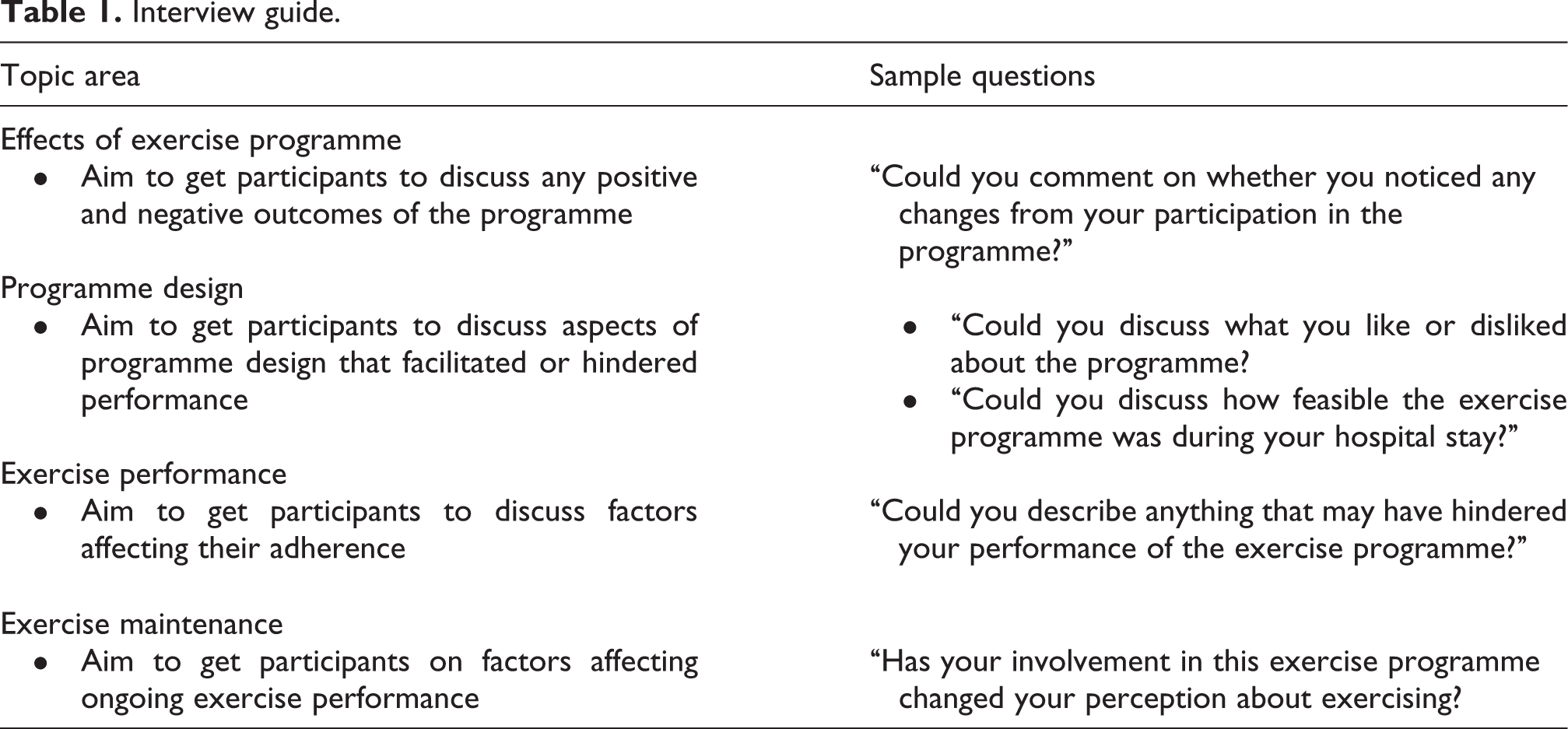
Effort was made to improve rigor by establishing credibility, transferability, dependability and conformability of the data. 17 For this study, the first author (CYT) had 7 years of clinical experience as a physiotherapist with patients admitted for acute exacerbation of COPD and supervised the physiotherapy sessions. The second author (NFT) had a physiotherapy background, worked at the affiliated university and had experience in qualitative research. The third author (FCB) had over 10 years of cardiorespiratory physiotherapy experience and worked at the affiliated university. The first and third authors completed coding. By having no direct contact with the participants, the third author was able to remain neutral to the coding process, thus reducing the potential of subjective prejudices from the first author. In addition, transferability and dependability of the study was ensured through the use of standard interview guides that had been agreed upon by the research team prior to interviews so as to ensure the same set of questions were asked of each participants (Table 1).
Interview guide.
Results
Of the 21 participants invited for the study, 19 (90%) took part. Two participants declined to participate, as they felt too unwell to participate in the interview. The sample comprised 12 women and 7 men, who averaged 70 years of age. Based on the GOLD guidelines, 20 participants were of a moderate severity (50–79% predicted forced expiratory volume in one second) in their COPD condition (Table 2). The average 3-minute walk test distance covered by participants who completed the exercise programme was 108 m (SD, 62 m) at base line (Table 2). This is approximately two-thirds of the average 3-minute walk test distance achieved by people with stable COPD status. 21
Demographic characteristics of participants.

F: female; M: male; Low: 40% maximal intensity; Mod: 70% maximal intensity; 3-MWT: 3-minute walk test distance; FEV1: forced expiratory volume in one second.
All participants completed the exercise rehabilitation programme during their hospital admission. Fourteen (74%) participants had previously attended pulmonary rehabilitation or a community based exercise class (Table 2). Eighteen interviews were conducted via the phone. The median length of stay in hospital was 6.0 days (range 3–16 days), while the median length of time in the exercise programme was 5.0 days (range 2–15 days).
The randomised controlled trial examining implementation of the exercise programme for patients (n = 32) admitted with an acute exacerbation of COPD found the programme to be safe and feasible. 14 Adherence to exercise was 83%, and from 174 exercise sessions, there was only one event classified as serious and in that case, symptoms had resolved within an hour and the person continued with their exercise at the next session. The exercise groups improved significantly in walking distance in the 3-minute walk test; however, no significant between-group differences were observed. 14
From analysis of the 19 transcribed interviews, one main theme (positive experience with exercise programme) and two sub-themes (increased motivation towards exercise at home and reluctance towards formal ongoing exercise programmes) emerged.
Main theme: positive experience with the exercise programme
There was an overwhelming response from the participants, irrespective of the intensity of the exercise programme allocated, expressing that their experience with the exercise programme was positive and enjoyable:
I thoroughly enjoyed the programme and I think I did quite well. You had people there with you showing you what you do and it was great company at the same time. It was not a chore but a fun thing to do. (P11) The fact that I was actively exercising while in hospital made the difference. (P2) The fact that I can do them to the point that I cannot do anymore was good. The flexibility of knowing that I can sit down if I cannot do it anymore and just take a few minutes to catch my breath back was good. (P15) I was just so grateful that someone encouraged me throughout my hospital stay to exercise even though it might be hard at that time. (P15) I think it was extremely useful to do the exercises while in hospital. (P2) It was very helpful. The exercises that were conducted improved my breathing quite substantially. (P5)
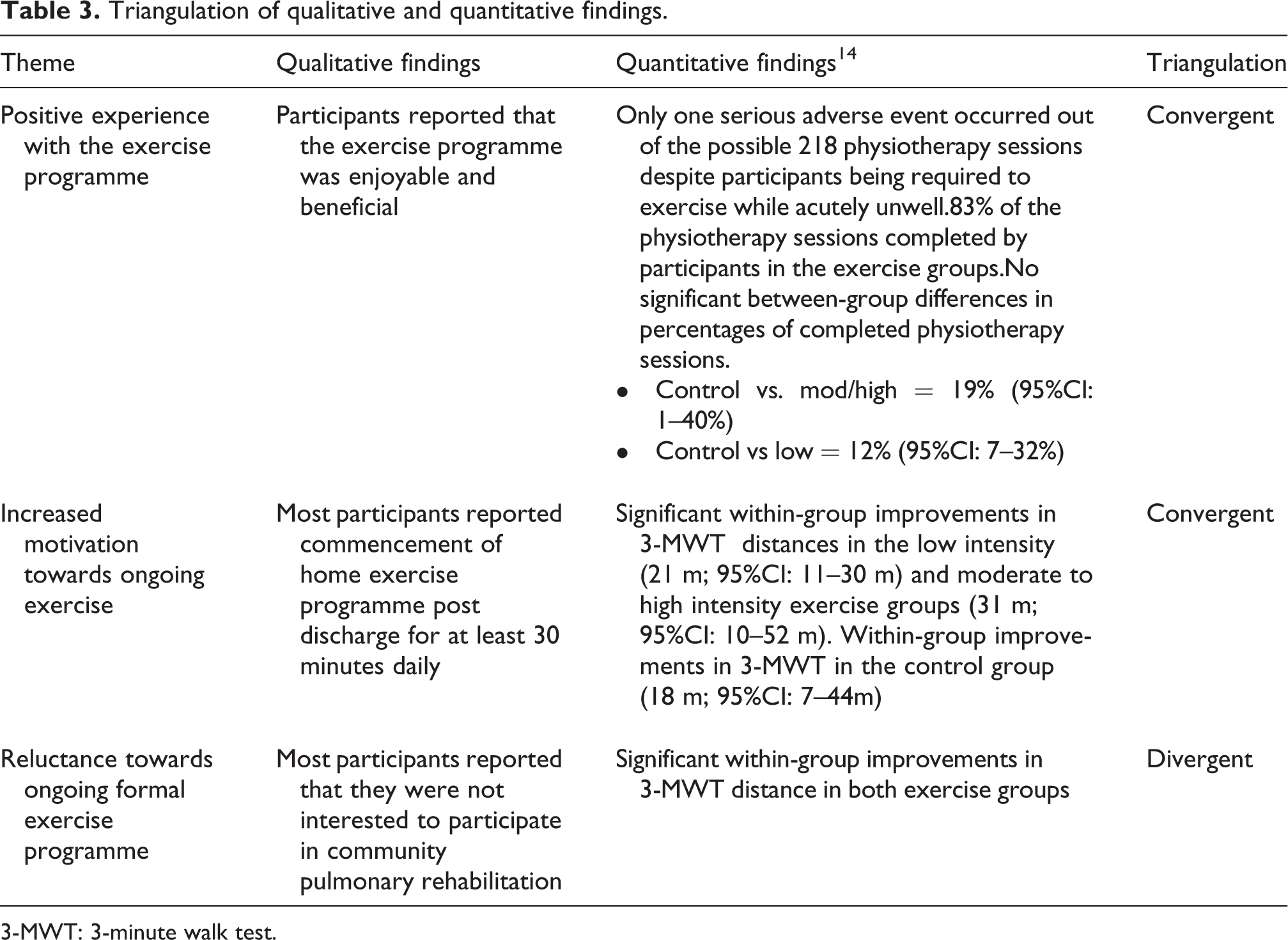
Participants did not report a negative experience with the programme or felt that the programme was ineffective. This finding converged with the quantitative data that indicated that it was safe to exercise, and a high percentage of physiotherapy sessions (83%) were completed among participants in the exercise groups with no significant differences between the two intensities of exercise, nor the control group and the exercise groups (Table 3). 14
Triangulation of qualitative and quantitative findings.
3-MWT: 3-minute walk test.
However, perceptions from participants that symptoms and co-morbidities had hindered their ability to participate in the programme had emerged during the interviews:
My muscles tend to really ache and cramp up quite a bit after the exercise programme and it took me a while after discharge to get rid of the muscle ache. (P18) I felt that two days were really short and if I had more time doing the exercises over a period of time, I believe that the exercises will improve my general mobility and also clear my lungs. (P3)
Sub-theme: increased motivation towards ongoing exercise
Related to the overall positive feedback regarding the exercise programme, a sub-theme emerged, that participant’s attitudes towards ongoing exercise had changed because of their experience with the inpatient programme. Convergent with the significant within-group improvements in 3-minute walk test distances in both the exercise groups (Table 3), participants reported a positive change in attitude towards exercise after participation in the exercise programme:
It had changed my attitude to keep going even if I am a little short of breathe or a little tired. (P15)
Sub-theme: reluctance towards ongoing formal exercise programmes
From the quantitative data, the exercise programme seemed to have motivated participants towards ongoing exercising. However, when participants were asked whether they were interested in attending ongoing formal community exercise programmes such as pulmonary rehabilitation, few expressed an intention to attend. It emerged that participants preferred exercising at home:
Basically I prefer not to work in a group. I prefer to do my own exercises and I have a pretty full schedule at the moment and may not have the time to attend an exercise programme. (P3) It is not my thing to do community exercise programme. I am worried about the travelling time and how far is it for me to walk to the facility. (P12)
Discussion
An overall positive experience among participants who had completed a very early exercise programme during their admission to hospital with an acute exacerbation of COPD was the main theme that emerged from this qualitative study. Participants who completed this exercise programme enjoyed the experience, despite being acutely unwell with potentially increased symptoms of dyspnoea. The programme appeared to reinforce the benefits of exercise to participants and motivated the majority of them to continue with an ongoing exercise programme after discharge.
Most participants did not cite feeling unwell during their acute exacerbation as a barrier towards their participation in the programme. Importantly, participants did express that participating in the exercise programme made them realise that they were able to exercise even when symptomatic. The above findings of the interviews converge with the reported adherence rates of 83%, 14 indicating that the exercise programme was indeed feasible (Table 3). Participants reporting that the exercise programme was enjoyable and that their acutely unwell status was not a barrier to participating may help counter concerns that getting people with COPD to exercise is challenging, especially when they are unwell. 10,12
Motivation to exercise at home on discharge appeared to be high in participants following the implementation of a very early exercise programme. The majority of the participants reported commencing a home exercise programme meeting the American Thoracic Society and the European Respiratory Society’s guideline of at least 30 minutes of moderate physical activity, 3–5 times a week following discharged from hospital (Table 2). 22 The positive health behaviour with reported independent home exercise might be related to the participants’ perception of benefits from undergoing the exercise programme as inpatients. The perceived benefits of the programme reported by participants converge with the results of the quantitative trial, where significant within-group improvements in 3-minute walk test distance in the both exercise groups were observed. 14
Considering that it has been demonstrated that physical activity levels for people with COPD decline to below population mean with a hospitalisation and remain below this mean 7 days after admission, 6 reported increases in motivation to exercise once home is a significant positive effect of commencing a supervised exercise programme when acutely unwell.
Personal and environmental factors can affect adherence to exercise in people with COPD. 23 The main personal factors included lack of perceived benefits, negative experience towards exercises and more importantly, a perception of poor health status that leads to a perception of an inability to exercise. 12,13,23–25 It seems that implementation of this early exercise programme may have addressed the personal factors affecting the level of adherence to exercise among COPD patients. 14 It might be expected that the reported improvement in motivation towards exercise may increase uptake of community pulmonary rehabilitation post discharge. However, willingness to take up pulmonary rehabilitation post discharge remained low among our participants.
A lack of transport and accessibility emerged from this study as the main deterrent for patients considering commencing community pulmonary rehabilitation. These results are consistent with literature finding accessibility issues as a consistent environmental factor affecting adherence to pulmonary rehabilitation. 12,13,23 It is possible that environmental factors may have a larger influence than personal factors in influencing the willingness of people with COPD to participate in community pulmonary rehabilitation. No further follow-up was conducted in this study to find out whether participants did eventually attend pulmonary rehabilitation as the aim of the study was only to determine perceptions of exercise when acutely unwell. Further research into whether changed perceptions affects uptake of community pulmonary rehabilitation is warranted.
Another theme that emerged as a reason for not intending to participate in pulmonary rehabilitation programme was the preference for independent home exercise over formalised exercise groups. Even though participants had expressed that they enjoyed the support that staff had given them during the exercise programme and felt that some supervision would benefit them with maintenance of their exercise programme, most participants reported preferring to exercise on their own either due to personal preference or being too “busy” to participate in a formal exercise programme. Utilising telecommunications to engage people with COPD with exercises at home while being supervised by a physiotherapist may eliminate issues such as transport and accessibility, addressing individual preference of exercising on their own. 26,27
Strengths and limitations
The short time between discharge and interview was both a strength and limitation of this study. The short time allowed participants to provide greater insights on their opinions about the programme. However, this also meant that we did not find out whether participants continued their exercise programme at home or whether they did change their mind regarding participation in community pulmonary rehabilitation. We were also unable to establish whether participants were completing the reported home exercise programme regimen. Also, interviewing those in the control group would have allowed us to describe differences in the perceptions about ongoing exercise and participation in community pulmonary rehabilitation programs and provided a clearer understanding of the impact the programme had on these perceptions.
Implications for future research or clinical practice
This qualitative study in combination with the results from the randomised controlled trial has indicated that implementation of a very early exercise programme for people with an acute exacerbation of COPD requiring hospitalisation may not only be feasible and safe but also enjoyable, beneficial and improve attitudes towards independent exercise at home among people with COPD. 14 However, despite these positive results, intention to participate in community pulmonary rehabilitation after discharge remained low. Exploration of long-term effects of exercise training for people with COPD who are acutely unwell is warranted, since changes in attitudes towards physical activity may be evident when a very early exercise programme is commenced.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.