
Abstract
Asthma and chronic obstructive pulmonary disease (COPD) cause significant morbidity and mortality worldwide, primarily through exacerbations. Exacerbations are often treated with antibiotics but their optimal course duration is uncertain. Reducing antibiotic duration may influence antimicrobial resistance but risks treatment failure. The objective of this article is to review published literature to investigate whether shorter antibiotic therapy duration affects clinical outcomes in the treatment of asthma and COPD exacerbations. We systematically searched electronic databases (MEDLINE, EMBASE, CINAHL, World Health Organisation International Clinical Trial Registry Platform, the Cochrane library, and ISRCTN) with no language, location, or time restrictions. We retrieved observational and controlled trials comparing different durations of the same oral antibiotic therapy in the treatment of acute exacerbations of asthma or COPD in adults. We found no applicable studies for asthma exacerbations. We included 10 randomized, placebo-controlled trials for COPD patients, all from high-income countries. The commonest studied antibiotic class was fluoroquinolones. Antibiotic courses shorter than 6 days were associated with significantly fewer overall adverse events (risk ratio (RR): 0.84, 95% confidence interval (CI): 0.75–0.93, p = 0.001) when compared with those of 7 or more days. There was no statistically significant difference for clinical success or bacteriological eradication in sputum (RR: 1.00, 95% CI: 0.88–1.13 and RR: 1.06, 95% CI: 0.79–1.44, respectively). Shorter durations of antibiotics for COPD exacerbations do not seem to confer a higher risk of treatment failure but are associated with fewer adverse events. This is in keeping with previous studies in community acquired pneumonia, but studies were heterogeneous and differed from usual clinical practice. Further observational and prospective work is needed to explore the significance of antibiotic duration in the treatment of asthma and COPD exacerbations.
Introduction
Background
Asthma and chronic obstructive pulmonary disease (COPD) are common and are becoming more prevalent globally. 1 –4 Exacerbations are a major driver of the morbidity, mortality, and cost associated with these chronic airways diseases. 5,6 The majority of exacerbations are nonbacterial in origin. 7 –9 They are, however, frequently treated with antibiotics hence causing a significant antibiotic burden. 10,11 For example, over 11 years, 22% of 16.1 million asthma presentations to US hospitals received antibiotics, largely against current guidelines. 12
Antimicrobial resistance is one of the most important public health crises facing the world today. Reduced susceptibility to penicillin or penicillin-resistance in Streptococcus pneumoniae exceeds more than 50% in many countries. 13 The World Health Organisation (WHO) issued a global action plan on antimicrobial resistance in 2015 which called for optimization of antibiotic prescribing. 14 Use of shorter antibiotic courses may be beneficial to reduce resistance, improve concordance, costs, and side effects. However, shorter courses risk treatment failure. Patients in middle and lower income countries are more susceptible to failure due to a number of factors: reduced susceptibility to penicillins; limited access to follow-up; malnutrition; and higher risk of abnormal lung architecture caused by air pollution, smoking, and industrial exposures. 15 –17
The ideal duration of antibiotic treatment for asthma and COPD exacerbations is uncertain and a prescribing consensus is a priority for providers. The last systematic review on antibiotic duration in COPD exacerbations was published in 2008 18 and none have been published in asthma exacerbations. We therefore undertook an up-to-date review and meta-analysis to investigate whether shorter courses of oral antibiotic treatment for asthma and COPD exacerbations are associated with different outcomes when compared with longer courses.
Methods
Data sources and search strategy
We conducted systematic searches of bibliographic databases including MEDLINE, EMBASE, and CINAHL through National Health Service library services. We also ran a search of the WHO International Clinical Trial Registry Platform, the Cochrane library, and ISRCTN and used search engines on their own websites. All databases were searched from inception until February 29, 2016. There was no restriction of publication language. We removed duplicate references using reference management software (EndNote X7; Thomson Reuters, USA). The search strategy is described below. The reference lists of earlier reviews on the same topic and abstracts of the European Respiratory Society and American Thoracic Society conferences from the previous year (2015) were hand-searched and titles included if the inclusion criteria were fulfilled.
Study selection
We included observational and controlled trials of adults (≥ 18 years) with a clinical diagnosis of asthma or COPD exacerbation. We only included original studies with explicitly different durations of the same oral antibiotic therapy. We excluded the studies of pneumonia treatment and prophylactic antibiotics.
We reviewed the list of titles to exclude publications which were clearly not contributory on this basis and duplicate titles. Two investigators screened the eligible abstracts independently. We obtained full text articles of selected papers via University of Liverpool library, NHS library, and interlibrary loans. Two investigators reviewed the full texts for eligibility independently. Any disagreement was resolved by a third investigator.
Data extraction
Two authors extracted data using a preset data extraction form which included details of the study’s publication, authorship, and funding; study characteristics (design and location); participants (sample size, method of recruitment, selection, and demographics); outcome measures; interventions; data analysis and reporting; confounding adjustments; and the main findings. Disagreements were resolved by discussion. We used RevMan 5.3 (Cochrane Collaboration) and EndNote X7 software in the collection and management of data from abstracts and papers.
Quality and risk of bias assessment
We assessed the studies’ accuracy and risk of bias using the Cochrane Handbook for Systematic Reviews of Interventions criteria. 19 Controlled trials were additionally analyzed using the Cochrane Collaboration’s tool for assessing risk of bias.
Analysis
We combined intention to treat population data from comparable studies in quantitative analyses. We pooled data using fixed effect model in RevMan 5.3. 20 We used the Mantel–Haenszel method, presenting data as risk ratio (RR) with 95% confidence intervals (CIs). We used statistical significance of p < 0.05 and assessed the degree of heterogeneity using the I2 statistic.
Results
Asthma
We identified 1604 individual titles through database searches (Figure 1). No additional studies were identified by hand-searching. The commonest reason for noninclusion into abstract screening was a lack of an asthma diagnosis for all participants (1304 records). We reviewed 29 abstracts. The commonest reason for not progression to full text review was missing explicit antibiotic duration (eight studies), with other reasons demonstrated in Figure 1. The one full text analyzed assessed antibiotics for one duration only and was hence excluded.
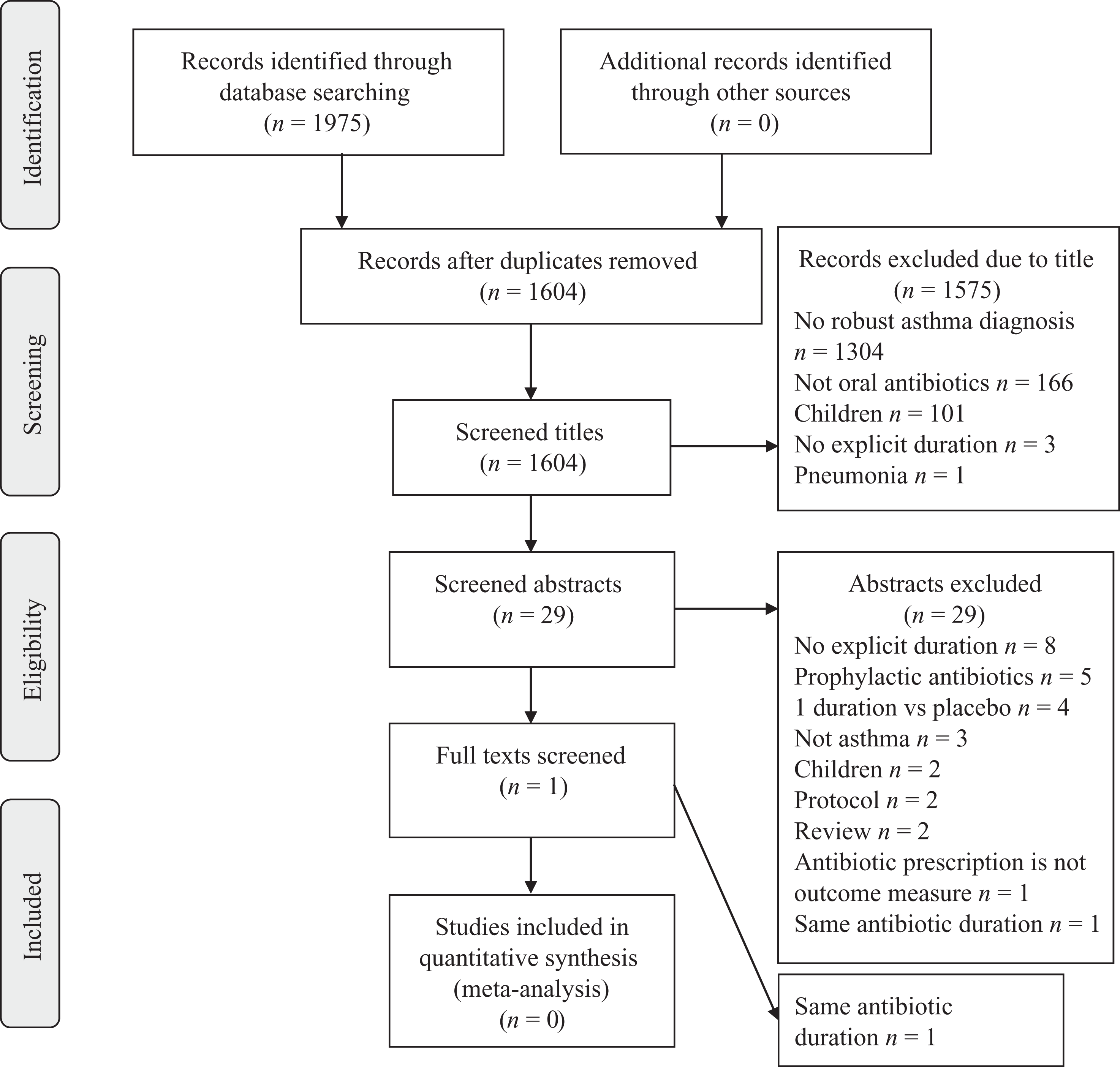
PRISMA flow diagram of systematic search for asthma studies.
COPD
We identified 1762 individual titles in COPD from database searches, 32 from hand-searching of recent reviews and 2 from conference abstracts (Figure 2). 18,21 The commonest reason for noninclusion in abstract screening was lack of COPD diagnosis (951 studies) and not assessing oral antibiotic treatment (603 studies). We screened 160 abstracts. The commonest reasons for exclusion at this stage were not assessing one antibiotic with two different durations (67 studies) or not comparing specific antibiotic durations (26 studies). Thirty-three full texts were eligible for analysis and 10 full texts were included in the final meta-analysis. One text in Polish was translated but was not applicable.

PRISMA flow diagram of systematic search for COPD studies. COPD: chronic obstructive pulmonary disease.
Characteristics and definitions of COPD studies
Design, participants, and setting
All 10 studies included in the meta-analysis were randomized, placebo-controlled trials (Table 1). Nine studies considered “chronic bronchitis” but included individuals with airflow limitation and a smoking history: their design would have predated the global use of the term “COPD.” 32 Eight studies reported smoking status. The youngest enrolled participant was 18 years old. Four studies recruited from outpatients, three from hospital admissions, one from primary care, and two from primary care and outpatients. Two multicenter studies included patients in the developing world (Latin America, Pakistan, Philippines), 29,31 and the rest were based in Europe or North America. Where documented, all exacerbations were diagnosed clinically, one study used microscopically confirmed purulent sputum. 26 There was a range of exacerbation severities from “mild” in outpatients to inpatients not needing critical care or ventilation. 26,30 Eight studies characterized the severity of the underlying lung disease.
Characteristics of included full text studies.

RCT: randomized controlled trial; COPD: chronic obstructive pulmonary disease; LTFU: lost to follow-up.
Interventions and outcomes
Fluoroquinolones were the most commonly examined antimicrobial class (five studies). Two studies assessed grepafloxacin and two assessed co-amoxiclav. The shortest antibiotic treatment was 3 days, the longest 10 days. One study included the potential administration of intravenous antibiotic in the first 3 days of treatment. 30 Follow-up duration varied from 0 days to one year to 3 days after final treatment for 1 year. All studies reported clinical responses (based on sputum production and appearance) and adverse effects. Nine studies assessed changes in sputum microbiology. Spirometry and inflammatory markers were assessed by a smaller number of studies. No studies compared outcomes in high versus low or middle income countries.
Risk of bias
One study had low risk of bias across all domains (Table 2). 26 One study had a high risk of bias due to not considering smoking as a confounding factor. 27 Two studies did not recruit enough patients for the primary end point based on their power calculations. 30,22
Table of risk of bias and study analysis methods.

LTFU: lost to follow-up.
Those with unclear risk of bias lacked information on blinding of participants, personnel, and outcome assessments (8 of 10 studies). All studies were commercially funded, one additionally received noncommercial funding. 30 We did not detect publication bias.
Analysis
Combining the populations of the 10 included studies, 1990 patients received short antibiotic courses (fewer than 6 days) and 1989 patients received long courses (7 or more days).
Clinical response
Nine studies used the resolution of clinical signs or symptoms of acute exacerbations as their primary outcome. Bennett et al. 22 used the absence of mucoid sputum in isolation and was hence excluded from meta-analysis for this outcome. Some studies reported outcomes at multiple time points so we presented clinical success as early (within 6 days of treatment completion), middle (7–14 days after treatment completion), or late (more than 20 days after treatment completion). Two studies assessed outcomes at 7–17 days and 17–23 days after treatment completion—they were excluded from this analysis. 23,28
There was no statistically significant difference between shorter and longer antibiotic courses in early clinical success (RR: 1.00, 95% CI: 0.96–1.03) in the five studies that considered this (Figure 3).

Forest plot of early clinical success, within 6 days of treatment completion, <6 versus ≥7 days antibiotic duration.
There was no statistically significant difference in medium (RR: 1.08, 95% CI: 0.91–1.27; five studies; Figure 4) or late clinical success (RR: 1.00, 95% CI: 0.99–1.11; six studies; Figure 5).

Forest plot of medium clinical success, 7–14 days after treatment completion, <6 versus ≥7 days antibiotic duration.

Forest plot of late clinical success, >20 days after treatment completion, <6 versus ≥7 days antibiotic duration.
Adverse events
Nine studies reported overall adverse events (1882 and 1877 patients for the shorter and longer duration, respectively). There was a statistically significant lower risk of developing adverse events in the shorter treatment group compared with the longer treatment group (RR: 0.84, 95% CI: 0.75–0.93, p = 0.001; Figure 6). For nausea, the risk was statistically significantly lower in the shorter treatment group (RR: 0.71, 95% CI: 0.52–0.98, p = 0.04; eight studies; Online Supplemental Material). No significant difference was found for diarrhea (RR: 1.03, 95% CI: 0.82–1.29; seven studies; see Online Supplemental Material).

Forest plot of overall adverse events, <6 versus ≥7 days antibiotic duration.
Bacteriological response in sputum
Eight studies assessed eradication or presumed eradication of pathogens which were present in pretreatment sputum samples. Presumed eradication was defined as improvement in clinical symptoms without sputum that could be cultured at follow-up. All studies used populations that had an identified pretreatment pathogen in sputum. There was no statistically significant difference between shorter and longer antibiotic treatment 0–6 days after treatment completion (RR: 1.08, 95% CI: 0.71–1.65; three studies) and 7–23 days after treatment completion (RR: 1.08, 95%: CI 0.83–1.39; seven studies; both in Online Supplemental Material).
Other outcomes
Two studies considered spirometric change—there was no statistically significant change in either study between shorter and longer durations. 22,28 One study assessed inflammatory markers, showing no difference between the different durations. 28 One study followed patients up to 1 year, assessing occurrence and time to new exacerbations, demonstrating no statistically significant differences between the groups. 22 Two studies included patients in the developing world but no subgroup analyses for these were reported. 29,31
Discussion
Summary of main findings
The prescription of antibiotics for COPD or asthma exacerbations is a very common clinical activity with serious potential adverse effects. Despite this, we found few studies had investigated optimal antibiotic duration for this indication. There was no difference in clinical success or bacteriological eradication for patients receiving fewer than 6 or more than 7 days of antibiotics for COPD exacerbations. There was, however, a significantly lower risk of side effects overall and specifically nausea in the shorter duration group.
Strengths and limitations
This review was undertaken systematically following best practice guidance from the Cochrane Collaboration. Interpretation of our findings should be made in the context of the analyzed studies having been largely undertaken at a time of significant variation in the diagnosis and treatment of COPD. The populations were therefore heterogeneous in key aspects such as smoking exposure and airflow obstruction (or did not have these clearly recorded) and by description of exacerbation outcomes. It is plausible that some study participants had other diagnoses such as bronchiectasis and chronic asthma. As many studies were undertaken prior to widespread use of standards for the assessment of COPD, it was not possible to stratify results by severity or GOLD criteria.
A sensitivity analysis without the study where the confounding factor smoking caused a high risk of bias showed no difference in our main findings (see Online Supplemental Material). Most of the older studies also had an “unclear” risk of bias by current standards. Fluoroquinolones were the commonest antibiotic class studied, but these are not first line treatment for uncomplicated exacerbations in usual clinical practice. This diminishes the external validity of the findings. 33
Setting in existing literature
Antibiotic courses of 5 or fewer days were as successful as longer courses for clinical and bacteriological cure for chronic bronchitis and COPD exacerbations in a meta-analysis in 2006. However, this study compared course length regardless of drug (e.g., 10 days of cefuroxime with 5 days of telithromycin). 21 Our study adds to the literature by including a search of the last 10 years of medical publications and by restricting analyses to consider only whether shorter courses of the same antibiotic are as effective and well tolerated. This reduces bias created by different mechanisms of action irrespective of duration.
Shorter courses of antibiotics have already been found to be as effective as longer courses in community acquired pneumonia and pharyngitis, and our findings are consistent with this. 18,21,34 –36
Antibiotics are not routinely recommended for the treatment of asthma exacerbations, and three published studies suggest no benefit above placebo. 7,10,25,37 However, antibiotics continue to be prescribed extensively for asthma exacerbations. 10,12 This discrepancy between observed antibiotic prescribing and limited available evidence highlights the need for further studies.
Implications for future research
This review supports the use of shorter courses of antibiotics for the treatment of COPD exacerbations. However, further research is required to ascertain if these findings hold true in the context of current COPD care, antibiotic use, and antibiotic resistance patterns. The development of extensive electronic health record databases of routinely collected data could be used to provide initial evidence in this regard and could support the design of targeted interventional studies. Future studies in high-income countries are likely to also include biomarker-guided treatment. However, significant challenges exist in lower and middle income countries where antibiotic resistance is prevalent and only fixed duration regimens are currently feasible.
Conclusions
This systematic review highlights the paucity of research evidence relevant to usual clinical practice informing selection of antibiotic duration for asthma and COPD exacerbations. It appears that courses of antibiotics of 6 or fewer days are equally as effective as those of 1week or longer, but associated with fewer side effects. However, due to the limitations of the published studies, new observational and interventional studies are needed to robustly inform guidelines.
Supplemental material
Supplemental Material, Review_COPD_Asthma_Abx_supplementary_data_1.0_-_revised_1.0 - Does antibiotic treatment duration affect the outcomes of exacerbations of asthma and COPD? A systematic review
Supplemental Material, Review_COPD_Asthma_Abx_supplementary_data_1.0_-_revised_1.0 for Does antibiotic treatment duration affect the outcomes of exacerbations of asthma and COPD? A systematic review by Marie Stolbrink, Jack Amiry and John D Blakey in Chronic Respiratory Disease
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Marie Stolbrink is funded by a National Institute of Health Research Academic Clinical Fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.