
Abstract
The aims of this article were to determine the levels of serum high-sensitivity cardiac troponin T (hs-cTnT) in obstructive sleep apnea (OSA) patients without cardiovascular disease (CVD) and to assess the efficacy of continuous positive airway pressure (CPAP). Snorers referred for polysomnography (PSG) for the investigation of OSA were eligible and hs-cTnT levels measured in our pilot study. Hs-cTnT was measured again after 3 months of CPAP treatment in participants with severe OSA. A total of 93 participants recruited after PSG. When compared with simple snoring group, severe OSA group had comparable higher hs-cTnT (7.5 ± 3.0 vs. 5.0 ± 2.1; p < 0.05). Hs-cTnT was positively correlated with apnea hypopnea index, and oxygen desaturation index (r = 0.283, 0.282; p = 0.006, 0.006, respectively). Hs-cTnT levels were not significantly altered in 28 individuals who received 3 months of CPAP treatment (8.4 ± 2.4 vs.7.6 ± 2.1; p = 0.064). Elevated hs-cTnT levels were observed in severe OSA patients without CVD, and CPAP treatment had no influence on this levels.
Keywords
Background
Obstructive sleep apnea (OSA) is a worldwide and highly prevalent disorder, affecting up to 25% of middle-aged men. 1 It is characterized by recurrent partial or complete upper airway obstruction during sleep, following by nocturnal intermittent hypoxia and sleep fragmentation. 2 OSA has been confirmed to be associated with cardiovascular morbidity and mortality. 3 –5 A growing body of evidence has demonstrated the high risk and mortality of ischemic heart diseases and myocardial injury in OSA patients. 6,7 Continuous positive airway pressure (CPAP) treatment can help to attenuate heart failure and to lower the risk of recurrent myocardial infarction in patients with sleep apnea and cardiovascular diseases (CVDs). 8 –10
Cardiac troponin, one of the intracellular cardiac myofibrillar proteins, is considered a novel biomarker for diagnosis of myocardial injury. 11 Compared to conventional detection, high-sensitivity cardiac troponin T (hs-cTnT) with a lower detection range has reliable predictive value for myocardial infarction, coronary artery disease (CAD), and heart failure. 12
A previous study showed that hs-cTnT was associated with disease severity in patients with OSA and cardiovascular morbidities, such as heart failure and CAD. 13 In contrast, Gami et al. 14 claimed that cTnT was not altered in patients with severe OSA and coexisting CAD. There are inconclusive data regarding the influence of intermittent hypoxia, a hallmark of OSA, on myocardial injury in OSA patients without any complication. Thus, there are limited data about serum hs-cTnT levels in OSA patients without CVD. Since intermittent hypoxia, familiar to ischemic reperfusion injury, might influence coronary artery blood flow, we hypothesized that enhanced hs-cTnT levels were observed in OSA patients.
The purpose of the present study was to determine whether serum hs-cTnT levels are raised in OSA patients without coexistent CVDs and to assess the impact of CPAP treatment on hs-cTnT in OSA patients.
Materials and methods
This pilot study was conducted at the Sleep Laboratory of the Respiratory Department of Zhongshan Hospital, Xiamen University between May 2014 and August 2015.The Institutional Review Boards of our hospital approved the present study. Informed consent was obtained from each enrolled participants.
Participants
Medical history (especially CVDs), sleep symptoms, and Epworth Sleepiness Scale (ESS) were collected from each participant. Snoring participants with or without daytime sleepiness who underwent full-night polysomnography (PSG) were enrolled consecutively. The exclusion criteria were as follows: (1) CVDs influencing serum hs-cTnT, such as CAD, acute coronary syndrome, atrial arrhythmias, or heart failure; CVDs were diagnosed by the symptoms, physical examination, biomarkers of myocardial damage, electrocardiogram, and echocardiography; (2) apparent respiratory diseases, such as pneumonia and pulmonary embolism; (3) chronic disease, such as chronic obstructive pulmonary disease, liver cirrhosis, renal failure, or mental disorder; and (4) previous OSA treatment.
Anthropometric and PSG
Body weight and height were measured in the morning, body mass index (BMI) was calculated as weight (kg)/height 2 (m). Waist circumference was measured at a level midway between the lower costal margin and the iliac crest. Blood pressure was measured on the right arm with the participants in a sitting position, using a mercury sphygmomanometer. PSG (E series, Compumedics, Australia) consisted of the following variables: oronasal airflow, snoring, thoracic and abdominal respiratory efforts, pulse oxygen saturation, body position, electroencephalography, electrooculography, electromyography, and electrocardiography. PSG records were staged in accordance with the criteria of the American Academy of Sleep Medicine (AASM). 15 Apnea hypopnea index (AHI) was defined as the number of apneas and hypopneas per hour of sleep. Oxygen desaturation index (ODI) was defined as the total number of episodes of oxygen desaturation ≥4% from the immediate baseline. Percentage of total sleep time spent with SaO2 < 90% and lowest oxygen saturation were also obtained. The severity of OSA was classified as simple snoring, mild, moderate, and severe by AHI <5, 5–14.9, 15–29.9, and ≥30 events/h, respectively. PSG was repeated during the CPAP titration.
Blood samples measurements
Blood samples for hs-cTnT were collected in the morning after the PSG when the participants have been fasted for at least 7 h. Glucose, lipid profiles, and serum creatinine were detected by standard methods on an automated Hitachi 7600 analyzer (Hitachi Inc., Tokyo, Japan). Hs-cTnT was detected using a third-generation Roche Elecsys assay (Roche Diagnostics, Shanghai, China). The low limit of the detection of hs-cTnT assay is 3 pg/mL, and the upper reference limit (corresponding to the 99% in a healthy population) is 14 pg/mL. The hs-cTnT estimates were repeated after 3 months of CPAP treatment.
CPAP treatment
Twenty-eight severe OSA patients with CPAP treatment (AutoSet, S9 series, Spirit, ResMed, Australia) were followed up for 3 months. An average CPAP that uses time ≥4.0 h per night was considered to be good compliance. The usage time, average AHI, and median pressure were obtained from a SmartCard of CPAP machine.
Statistical analysis
SPSS statistical software version 21.0 for Windows (SPSS, Inc, Chicago, Illinois, USA) was used for statistical analysis. Categorical variables were presented as number (percentage). Descriptive variables were showed as mean ± standard deviation (SD) and were analyzed by one-way analysis of variance, followed by post hoc comparisons. Spearman correlation was conducted to evaluate the interrelation between clinical, polysomnographic, biochemical variables, and hs-cTnT. Multiple linear regression analysis was performed to explore the independent predictors of hs-cTnT. Paired t-tests were conducted to evaluate the difference of hs-cTnT before and after CPAP treatment. A p value <0.05 was considered statistically significant.
Results
Clinical, PSG, and biochemical variables in participants stratified by AHI score
A total of 93 participants (81.7% male, mean age 47.9 ± 11.8 years, and mean BMI 27.2 ± 2.9 kg/m2) were recruited after PSG in the study. Compared with simple snoring group, severe OSA group had comparable higher BMI and waist circumference. In contrast, blood pressure, lipid profiles, and glucose showed no significant difference between each group. There was a higher hs-cTnT levels in severe OSA group than in simple snoring group (7.5 ± 3.0 vs. 5.0 ± 2.1; p < 0.005; Table 1).
Characteristics of enrolled subjects stratified by the severity of OSA.

OSA: obstructive sleep apnea; ESS: Epworth Sleepiness Scale; BMI: body mass index; AHI: apnea hypopnea index; ODI: oxygen desaturation index; TST: percentage of total sleep time spent with SaO2 < 90%; LaSO2: lowest O2 saturation; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; hs-cTnT: high-sensitivity cardiac troponin T.
a p < 0.005
Correlation and multiple regression analysis
Table 2 and Figure 1 show that there was a weak positive correlation between hs-cTnT and AHI and hs-cTnT and ODI (r = 0.283, 0.282; p = 0.006, 0.006, respectively). The hs-cTnT was also inversely correlated with the lowest oxygen saturation (r = −0.207; p = 0.046). After adjustment for age, BMI, systolic blood pressure, diastolic blood pressure, total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and glucose, multiple linear regression demonstrated that AHI was an independent risk factor for elevated hs-cTnT (R 2 = 0.188; p = 0.000).

Scatter plot shows the correlation between polysomnographic parameters and hs-cTnT. (a) AHI was positively correlated with hs-cTnT; (b) ODI was associated with hs-cTnT. hs-cTnT: high-sensitivity cardiac troponin T; AHI: apnea hypopnea index; ODI: oxygen desaturation index.
Correlations between hs-cTnT and clinical, polysomnographic parameters.

hs-cTnT: high-sensitivity cardiac troponin T; BMI: body mass index; AHI: apnea hypopnea index; ODI: oxygen desaturation index; TST: percentage of total sleep time spent with SaO2 < 90%; LaSO2: lowest O2 saturation; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol.
Relationship between ESS and hs-cTnT in OSA patients
In order to evaluate the influence of daytime sleepiness on hs-cTnT, we divided OSA patients (n = 78) into low ESS group (ESS ≤ 10; n = 48) and high ESS group (ESS > 10; n = 30) according to the previous studies. 16,17 No significant difference in hs-cTnT levels was observed in OSA patients with or without daytime sleepiness (Figure 2(a)), and the relationship between ESS and hs-cTnT in all participants (n = 93) did not reach statistically significant (Figure 2(b)).

Relationship between ESS and hs-cTnT.(a) hs-cTnT levels was similar in OSA patients regardless of the ESS score; (b) scatter plot shows that ESS was not correlated with hs-cTnT in all participants (n = 93). ESS: Epworth Sleepiness Scale; hs-cTnT: high-sensitivity cardiac troponin T; OSA: obstructive sleep apnea.
Change of hs-cTnT after 3 months of CPAP treatment
A total of 28 severe OSA participants with CPAP treatment participated in the further study. The mean age was 49.4 ± 13.0, the CPAP mean usage duration was 6.4 ± 3.8 h/night, and the median pressure was 9.49 (6.15–13.19) cm H2O. The characteristics of the 28 participants are outlined in Table 3. The mean AHI after CPAP treatment was 2.73 ± 1.71 events/h. Hs-cTnT levels were not significantly altered in 28 individuals who received 3 months of CPAP (8.4 ± 2.4 vs. 7.6 ± 2.1; p = 0.064; Figure 3). The associations between polysomnographic parameters, ESS, and hs-cTnT were also detected both before and after CPAP treatment in 28 severe OSA patients. However, no statistical correlations were showed between the changes of AHI and hs-cTnT (Figure 4(a)), ODI and hs-cTnT (Figure 4(b)), and ESS and hs-cTnT (Figure 4(c)).

Change of hs-cTnT after CPAP treatment. hs-cTnT: high-sensitivity cardiac troponin T; CPAP: continuous positive airway pressure.
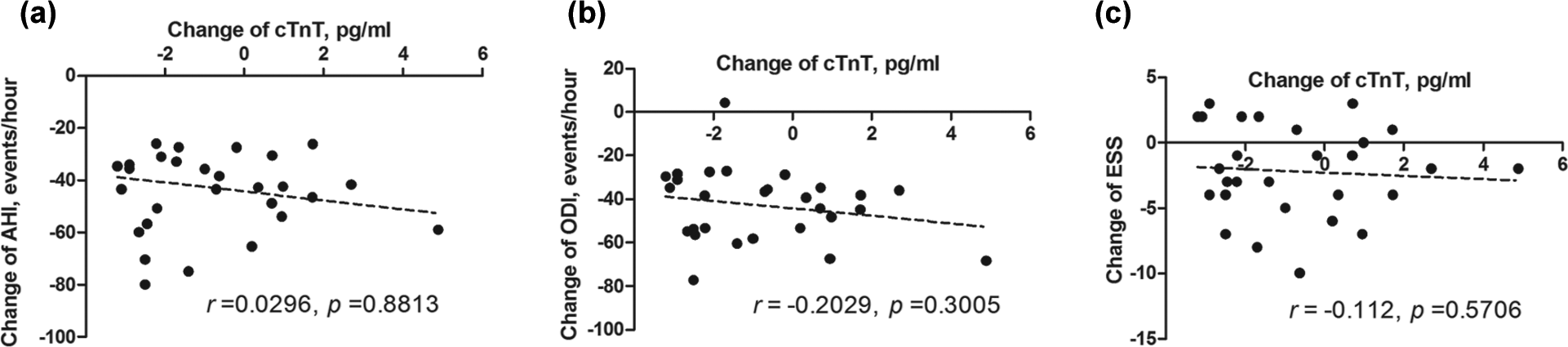
Correlation between the changes of polysomnographic parameters and hs-cTnT before and after CPAP treatment in 28 severe OSA patients. (a) Correlation between AHI and hs-cTnT pre-CPAP and post-CPAP treatment. (b) Correlation between ODI and hs-cTnT pre-CPAP and post-CPAP treatment. (c) Correlation between ESS and hs-cTnT pre-CPAP and post-CPAP treatment. hs-cTnT: high-sensitivity cardiac troponin T; CPAP: continuous positive airway pressure; OSA: obstructive sleep apnea; AHI: apnea hypopnea index; ODI: oxygen desaturation index; ESS: Epworth sleepiness scale.
Characteristics of 28 (25 males) severe OSA patients (baseline and after 3 months CPAP treatment).

OSA: obstructive sleep apnea; CPAP: continuous positive airway pressure; ESS: Epworth Sleepiness Scale; BMI: body mass index; AHI: apnea hypopnea index; ODI: oxygen desaturation index; TST: percentage of total sleep time spent with SaO2 < 90%; LaSO2: lowest O2 saturation; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; hs-cTnT: high-sensitivity cardiac troponin T.
a p < 0.001
Discussion
The present study examined the association between OSA and hs-cTnT in patients without preexisting of CVD and evaluated the efficacy of CPAP on hs-cTnT in OSA patients without CVD. Our results illustrated that serum hs-cTnT levels were relatively high in severe OSA patients when compared with simple snoring participants. After adjustment for confounding factors, AHI, the polysomnographic variable, was an independent risk factor for increased hs-cTnT levels. After 3 months of CPAP treatment, the hs-cTnT levels remained unchanged in OSA patients.
Cardiac troponin is one of the components of myofibrillar contractile apparatus. 18 The third generation assay, hs-cTnT, is widely considered as a novel biomarker of myocardial damage and a reliable predictor for cardiovascular events and mortality risk. 12,19 Recently, a large body of evidence indicated that elevated hs-cTnT was also detected in patients with diabetes mellitus, sepsis, renal failure, and acute pulmonary embolism. 20 –23
There is a paucity of information regarding the serum hs-cTnT levels in OSA patients. Gami et al. 14 in 2004 failed to find detectable cardiac troponin T in 15 male volunteers with OSA and CAD. A study with 505 subjects showed that hs-cTnT was associated with the severity of OSA; however, the association no longer existed after adjustment for the following cardiovascular risk factors: old age, male sex, current hypertension, and diabetes mellitus. 13 A study involving 200 male participants without CAD indicated that the proportion of participants with detectable hs-cTnT level was higher in OSA patients than in control participants. 24 The Atherosclerosis Risk in Communities (ARIC) Study and the Sleep HeartHealth Study (SHHS) (ARIC-SHHS) study, with 1645 participants free of CAD and heart failure, demonstrated that OSA severity is independently associated with the increased levels of hs-cTnT. 25 Consistent with most of previous studies, our results delineated that when compared with control group, patients with severe OSA had comparably high hs-cTnT. After adjustment for confounding factors, AHI was independently associated with hs-cTnT. The novelty of our study was that all participants we enrolled were free of various diseases, which may influence the concentrations of hs-cTnT, such as CVDs, hypertension, and chronic condition of lung, liver, and kidney.
Previous studies indicated that compared with OSA patients without daytime sleepiness, OSA patients with excessive daytime sleepiness had high risk to develop hypertension, 26 CVD, 27,28 and nonalcoholic fatty liver disease. 29 Study also inferred that it was ESS score rather than AHI associated with cardiovascular risk. 27 OSA patients with high ESS score had an increased CPAP adherence. 30 In the present study, however, no significant difference was observed in hs-cTnT levels in OSA patients with or without excessive daytime sleepiness. There was also not a correlation between ESS score and hs-cTnT either in whole enrolled participants or in 28 severe OSA patients received CPAP treatment. The small sample size and strict inclusion criteria may be postulated as potential reasons.
Various factors might contribute to myocardial injury in OSA patients: intermittent hypoxia, sympathetic activation, oxidative stress, vascular endothelial dysfunction, and metabolic abnormalities. All the factors aforementioned may trigger or aggravate hypertension, ventricular hypertrophy, myocardial fibrosis, and heart systolic/diastolic dysfunction in OSA patients. 31 Several experimental studies concerning the relationship between intermittent hypoxia and myocardial injury yielded uncertain conclusion. A study by Han et al. 32 revealed that intermittent hypoxia-induced cholesterol accumulation and caspase-dependent apoptosis in the heart may induce the cardiac damage. Park and Suzuki 33 proved that enhanced cardiac injury was not seen in mice treated with 4 weeks of intermittent hypoxia, and they speculated that the heart had adapted to intermittent hypoxia. Both human research and experimental studies are required to draw a definite conclusion of the relationship between OSA and myocardial injury, especial to identify whether OSA patients develop CVD in the near future.
CPAP was widely accepted as the first choice for OSA treatment strategy. Robust data proved that CPAP treatment can help to normalize the blood pressure and to decrease the risk and mortality of CVD in OSA population. 2,9 Nevertheless, the influence of CPAP on hs-cTnT yielded equivocal results. A study involving 200 participants without coexistent CAD demonstrated that a significant increase in hs-cTnT was found after 1 year of CPAP device application, and the authors postulated that CPAP treatment might aggravate cardiovascular events. 24 Colish et al. 34 pointed out that in OSA patients, after 12 months of CPAP treatment, there were a significant changes in right ventricular end-diastolic diameter, left atrial volume index, and pulmonary hypertension, but not in C-reactive protein, N-terminal pro-B-type natriuretic peptide, and hs-cTnT. The study by Cifci et al. 35 also failed to show statistically significant difference in hs-cTnT pre-CPAP therapy and post-CPAP therapy in OSA patients. Fifteen OSA patients with CAD were investigated by Gami et al. in 2004, and the results illustrated that 4 h of CPAP treatment had no influence on hs-cTnT levels. 14 A study from Germany also supported the idea that one night of CPAP application had no effect on hs-cTnT in OSA patients with coexisting CAD. 36 Similar to previous studies, the result of the present study showed that serum hs-cTnT levels were not altered after 3 months of CPAP treatment in severe OSA patients without coexisting cardiovascular events. No significant correlations were found between polysomnographic parameters, AHI or ODI, and hs-cTnT in 28 severe OSA patients both before and after CPAP treatment. We speculated that numerous factors might possibly explain these results: most importantly, only OSA participants without cardiovascular complications were enrolled, and the mean concentrations (8.4 ± 2.4 pg/mL) of basal hs-cTnT prior to CPAP therapy were in the normal range (3–14 pg/mL). It might partly explain the aforementioned phenomenon that hs-cTnT was sensitive to myosite injury or necrosis rather than ischemia. Furthermore, the small sample size (28 patients) and the short-term usage of CPAP might influence the negative results. However, OSA patients without coexisting CVDs are difficult to collect. Our study group spent totally 15 months searching for patients who met our strict inclusion criterion. Of the 93 enrolled patients (30 severe OSA), only 28 participants underwent 3 months of CPAP treatment. The question of the small simple size was also confronted in other previous studies when concerning the hs-cTnT levels in OSA patients. 14,34 –36 Further long-term, larger randomized controlled trials are needed to clarify the effect of CPAP on hs-cTnT levels among OSA patients.
Several limitations should be mentioned of the present study. First, the present study was a pre- and post comparative study rather than case-control study. Second, the small sample size would not be powered to detect a difference in hs-cTnT and larger studies are warranted. Third, we only studied 3 months of treatment and did not include an effect with longer treatment.
Conclusions
The present study indicated that the relatively high concentrations of hs-cTnT levels were observed in severe OSA patients without CVD. No significant change in hs-cTnT was observed after 3 months of CPAP treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by grant 2013-2-88 for Youth Research Fund from Fujian Provincial Health Bureau and grant 3502Z20154019 for Fund from Xiamen Science and Technology Bureau.