
Abstract
Keywords
Introduction
Obstructive sleep apnea syndrome (OSAS) is a very common sleep disorder characterized by upper respiratory tract obstruction and reduced airflow or repetitive respiratory cessation, 1 and causes nocturnal hypoxemia, excessive daytime sleepiness (EDS), periodic snoring, sleep disruption and cardiovascular complications. Both nocturnal hypoxemia and EDS have been found to cause cognitive deficits in OSAS patients,2,3 and decreased performance of psychomotor and executive tasks such as programming, regulation, planning and realization of goal-directed behaviors was linked to the severity of hypoxemia, whereas memory and attention deficits were related to EDS. 4
Continuous positive airway pressure (CPAP) is the most effective treatment for OSAS and has been shown to improve sleep quality and daytime sleepiness.5–7 However, some neuropsychological impairments still persist after CPAP treatment, which indicates existence of irreversible anoxic brain damage caused by nocturnal hypoxemia in patients with severe OSAS.8–10 Previous studies have shown association of electroencephalographic (EEG) features of non-rapid eye movement (NREM) sleep with daytime performance and sleepiness, which suggests that EEG measures may potentially be used as biomarkers of cognitive performance and sleep quality in OSAS patients. 11 Higher slow wave activities during NREM sleep stage 3 (N3) are related to improved procedural learning, memory process and faster reaction time, while reduced theta wave activities in NREM sleep are associated with increased daytime sleepiness.12,13 OSAS patients were found to have abnormal sleep structure which was related to severity of the disorder. With CPAP treatment, sleep architecture and quality were improved immediately as shown by increased slow wave sleep (SWS) and rapid eye movement (REM) sleep. 14 In untreated OSAS patients, EEG slowing was observed over all cortical regions during REM sleep and wakefulness, which might be due to cerebral impairment associated with hypoxemia and recurrence of apneas. 2 Further EEG analyses showed a decrease in alpha and theta relative power as well as an increase in beta (mainly in central cortical region) and delta relative power during wakefulness and REM sleep in OSAS patients without treatment. 15 After CPAP treatment for 6 months, both daytime sleepiness and EEG slowing were improved. Reduction of the airflow in OSAS patients increased K-complexes (KCs), the definitive markers of N2 sleep, which were associated with increased cortical arousals and sleep fragmentation, and consistent with an overall slowing of EEG activity during wakefulness. 16 Nocturnal slow wave activity surrounding KCs during N2 sleep was associated with objectively measured daytime function using psychomotor vigilance test and CPAP treatment led to a decrease in KC density, and an increase in SWA surrounding KCs (ΔSWAK) and relative slow-wave activity (%SWA) during N2 sleep. 17 However, whether there were any changes in EEG activities during N3 sleep in OSAS patients and any effects of CPAP treatment on these changes were unclear. Therefore, the aim of the study was to investigate whether EEG activities during N3 sleep were altered in OSAS patients and to test effects of CPAP treatment on these changes.
Methods
Subjects
The normal controls were recruited from subjects who underwent routine checkup (i.e., physical examination, blood glucose, blood pressure, hepatic and renal function tests, and electrocardiographic examination, etc.) at the Jiangxi Provincial People’s Hospital during the period from March to December 2020, and had good general health (e.g. without ischemic artery disease, hypertension, and diabetes mellitus, etc.) and sleep quality with sleep apnea/hypopnea index (AHI)<5 events per hour of sleep, and regular life habits. They were free from any conditions listed in the exclusion criteria (see below) and a history of EDS, irregular sleep or other sleep disorders. Poor sleepers and shift-workers were excluded.
To conduct this cross-sectional study investigating effects of CPAP treatment on EEG activity during N3 sleep in the OSAS patients compared to normal controls, the OSAS patients were recruited from the inpatients who underwent polysomnographic (PSG) examination and a series of routine medical tests due to obstructive sleep apnea at the Hospital during the period from March to December 2020. Inclusion criteria for the OSAS patients included sleep apnea/hypopnea index (AHI) > 15 events per hour of sleep and a minimum arterial oxygen saturation (SaO2) < 90% during sleep. Exclusion criteria included a history of other sleep disorders, neurological diseases, chronic obstructive pulmonary disease, primary and secondary pulmonary diseases, rheumatic heart disease, cardiomyopathy, symptomatic ischemic artery disease [New York Heart Association (NYHA) Functional Class II or worse] and hypertension (Stage II or higher), uncontrolled diabetes mellitus with complications, excessive alcohol consumption or drug abuse. In addition, patients with a history of stroke, use of any medication known to influence sleep, EEG or respiratory function within a month prior to the study and the use of psychotropics were excluded. No caffeine, tea and other stimulating drinks were allowed 12 h before PSG recordings. However, OSAS patients with hypertension (Stage I), ischemic heart disease (NYHA Functional Class I) or controlled type II diabetes mellitus without any complications were included in the study.
All experimental procedures and research protocols were approved by the Research Ethnic Committee of the Jiangxi Provincial People’s Hospital (No. 2019–014) in accordance with principles of declaration of Helsinki, and informed consents were obtained from all the subjects.
Polysomnographic recordings
PSG recordings were performed as previously reported 18 on the normal subjects and patients with OSAS, and CPAP treatment was applied to the patients with OSAS on the second night. Sleep scoring and staging as well as analyses of respiratory changes were performed according to the standards established by American Academy of Sleep Medicine (AASM). 19 An obstructive sleep apnea episode was defined as a drop in airflow of 90% from baseline lasting at least 10 s with inspiratory movements. A hypopnea episode was determined when a drop in airflow of 30% from baseline lasted for at least 10 s, and events must be associated with ≥3% oxygen saturation decrease from pre-event baseline or an arousal. 19 The number of episodes of apneas and hypopneas per hour of sleep (AHI), minimum SpO2 value recorded during sleep, and the sleep time spent with SpO2 <90% 1 were used to estimate the severity of OSAS.
EEG analyses
Since EEG activities in the frontal part of the brain were more sensitive for evaluation of the outcome and effectiveness of CPAP treatment, 20 and no significant differences in EEG activities were found between the left and right hemispheres in the previous study 21 and in the pre-experiments of this study, and unilateral EEG activities were analyzed in the previous studies.21–23 Therefore, EEG activities recorded from F3-A2 derivation were chosen to analyze in details.
EEG traces were visually examined before quantitative spectral assessment to avoid mini-epochs containing cyclic alternating patterns (CAPs) and artefacts from movements and associated EMG activities. For each subject, a total of 24 mini-epochs (4 s in length for each epoch, a total of 96 s) during each episode of N3 sleep without artefacts were selected according to the previous study. 20 The use of these mini-epochs was essential for the quantitative EEG analysis to avoid EEG segments with artefacts from movements and associated EMG activities during N3 sleep. 24 In addition, respiratory events related EEG segments during N3 sleep were avoided since respiratory events were often associated with cortical arousals, CAPs, and movements as well as related EMG contamination.25,26 Power spectral analysis (PSA) based on fast Fourier transform (FFT) was performed on the F3-A2 derivation using the Brainstorm program (Version 2.0., GNU GPLv2, McGill University, Montreal, QC, Canada) to analyze 4 s mini-epochs with a resolution of 0.25 Hz and a cosine window smoothing.
Four EEG frequency bands were selected for analysis, namely delta (0 to 3.99 Hz), theta (4 to 7.99 Hz), alpha (8 to 13 Hz), and beta (13.01 to 30 Hz) waves. 27 In addition, slow wave activities (0.5-2 Hz) were also analyzed. The amplitudes of delta, theta, alpha and beta waves were respectively determined and the spectral power density of EEG (0-30 Hz) activities were first determined. Then, the mean absolute and relative power for these waves was calculated. Relative EEG power was calculated as the power of a given EEG frequency band divided by the sum of absolute power across the four frequency bands, and it reflected the contribution of EEG activity of a given frequency band to the sum of absolute power.28,29 The absolute power ratio of slow to fast EEG waves (i.e., absolute power of delta and theta waves/absolute power of alpha and beta waves) was calculated. In addition, cortical arousals, which were abrupt shifts in EEG frequency to theta, alpha waves, and/or frequencies greater than 16 Hz but not spindle activity lasting for at least for 3 s, were defined. 19 Since cortical arousals longer than 15 s were scored as wake according to the AASM criteria, 19 only cortical arousals with a duration of 3–15 s were counted when arousal index was calculated.
Statistical analyses
The data were presented as mean ± standard error of mean (SEM) if normally distributed. Otherwise, the data were presented as medians (minimum-maximum). Paired t tests and Wilcoxon signed-rank tests were used for normal and skewed distribution paired data (e.g. before and during CPAP treatment), respectively, and one-way ANOVA on rank followed by Mann–Whitney tests with Bonferroni correction were used to compare power of each type of EEG waves among OSAS patients with treatment and without treatment, and normal controls. The statistical analysis was performed by using SPSS (Version 26, IBM, Armonk, NY, USA). Statistical power analysis was conducted for each test to make sure it was at the desired level and p < .05 was considered to be statistically significant.
Results
General characteristics of sleep variables
Demographic data and sleep and respiratory variables in normal subjects, and in OSAS patients with and without CPAP treatment.
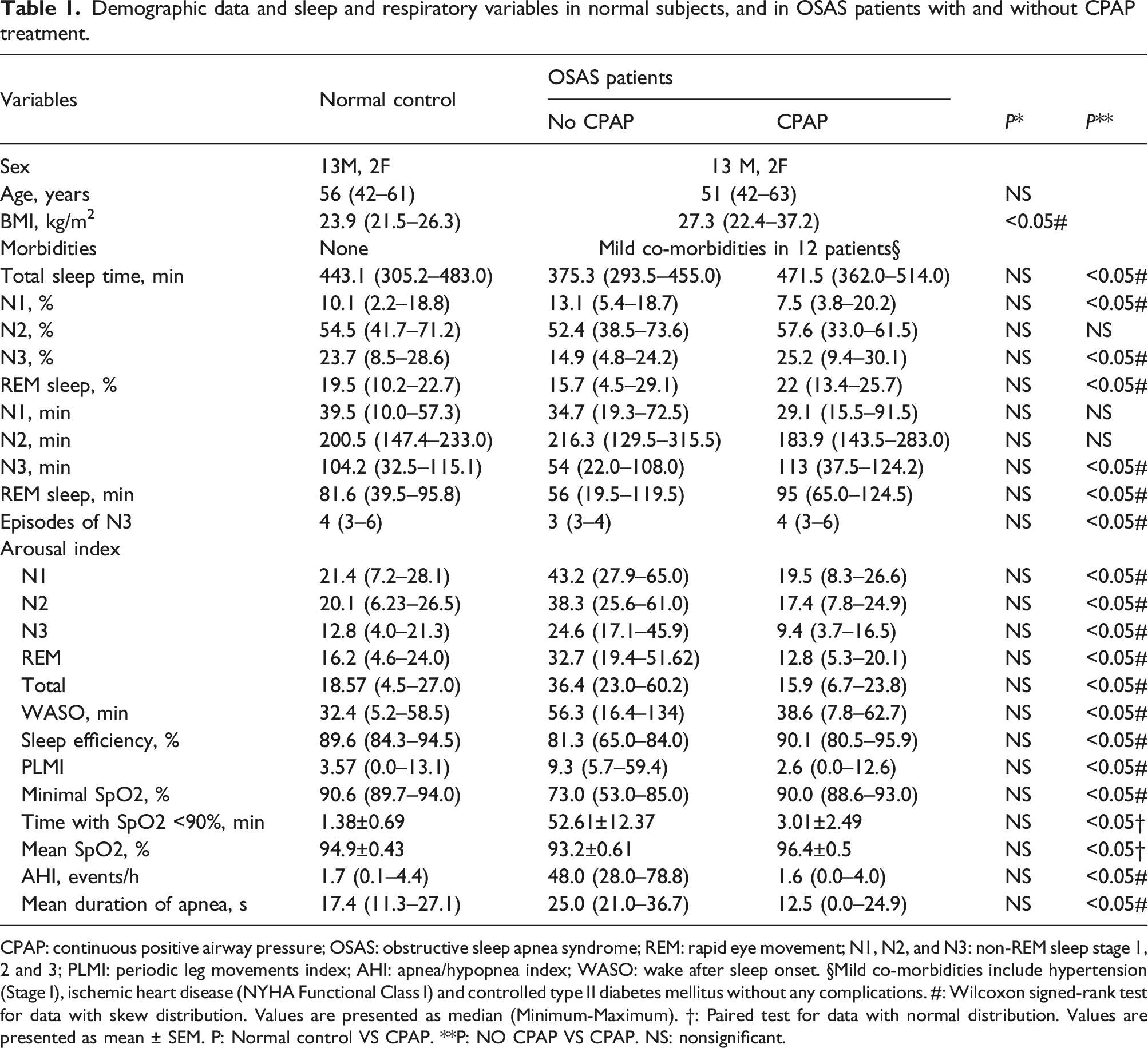
CPAP: continuous positive airway pressure; OSAS: obstructive sleep apnea syndrome; REM: rapid eye movement; N1, N2, and N3: non-REM sleep stage 1, 2 and 3; PLMI: periodic leg movements index; AHI: apnea/hypopnea index; WASO: wake after sleep onset. §Mild co-morbidities include hypertension (Stage I), ischemic heart disease (NYHA Functional Class I) and controlled type II diabetes mellitus without any complications. #: Wilcoxon signed-rank test for data with skew distribution. Values are presented as median (Minimum-Maximum). †: Paired test for data with normal distribution. Values are presented as mean ± SEM. P: Normal control VS CPAP. **P: NO CPAP VS CPAP. NS: nonsignificant.
As shown in Table 1, with CPAP treatment, the total sleep time, sleep efficiency, number of cycles of N3 sleep, and percentage and duration of N3 and REM sleep were significantly increased, while the percentage of N1 sleep, arousal indexes during N1-N3 and REM sleep, and PLMI were significantly decreased. There were no significant differences in the total sleep time, wake after sleep onset (WASO), arousal indexes, sleep efficiency, percentage of N2 and REM sleep, durations of N1 and N2 sleep between normal controls and OSAS patients with CPAP treatment.
The respiratory variables during sleep were significantly improved with CPAP treatment. The minimal SpO2 values were increased significantly from 73.0 (53.0– 85.0)% to 90.0 (88.6–93.0)%, while time spent with SpO2 < 90% was significantly decreased from 52.61 ± 12.37 min (mean ± SEM) to 3.01 ± 2.49 min, AHI was significantly decreased from 48.0 (28.0–78.8) events/h to 1.6 (0.0–4.0) events/h, mean apnea duration was significantly decreased from 25.0 (21.0–36.7) s to 12.5 (0.0–24.9) s and mean SpO2 values were significantly increased from 93.2 ± 0.61% to 96.4 ± 0.5% (p < .05). These respiratory variables in the OSAS patients with CPAP treatment were not significantly different from those in the normal controls.
Effects of CPAP on power of EEG waves during N3 sleep
The power of spectral density of slower waves was obviously decreased in the OSAS patients, and was increased with CPAP treatment to the level similar to that in normal controls (Figure 1). As shown in Figure 2A-C, both mean absolute delta and theta powers were significantly decreased in the OSAS patients (p < .05, No CPAP VS Normal Control) and increased with CPAP treatment (p < .05, No CPAP VS CPAP) to the levels in the normal controls (p > .05, CPAP VS Normal control), while absolute beta power was significantly decreased with CPAP treatment (p < .001, No CPAP VS CPAP). In addition, CPAP treatment significantly increased mean absolute power of slow wave activity (0.5-2 Hz) in OSAS patients (p < .05), making them similar to (not significantly different from) the normal control group. Spectral power density for EEG activities (0–30 Hz) in normal controls (dotted line), and the OSAS patients without (dash line) and with CPAP treatment (solid line) during the first (A), second (B) and third sleep cycle (C) of NREM sleep stage 3. CPAP, continuous positive airway pressure. Absolute (A, B, C) and relative power (D, E, F) of slow wave activities, delta, theta, alpha and beta waves in normal controls (dark grey bars), and apneic patients without (light grey bars) and with CPAP treatment (empty bars) during NREM sleep stage 3 of the first (A, D), second (B, E) and third sleep cycle (C, F). CPAP, continuous positive airway pressure; EEG, electroencephalographic. Values are shown as median (minimum-maximum). One-way ANOVA on rank, *p < .05, **p < .001, and ***p < .0001.

As shown in Figure 2D-F, the relative delta power in the OSAS patients was significantly decreased compared with that in normal controls, and CPAP treatment significantly increased the power. In contrast, the relative powers of theta, alpha and beta in the OSAS patients were significantly increased compared with those in normal controls and CPAP treatment significantly decreased the powers to the levels in the normal controls.
The absolute power ratio of slow to fast EEG waves (i.e., absolute power of delta and theta waves/absolute power of alpha and beta waves) was significantly decreased in the OSAS patients and CPAP treatment significantly increased the ratio to the level in the normal controls (Figure 3). Absolute EEG power ratio of slow (delta and theta waves) to fast EEG waves (alpha and beta waves) in normal controls (dark grey bars) and OSAS patients without (light grey bars) and with CPAP treatment (empty bars) during the first, second and third sleep cycle of sleep stage N3. CPAP, continuous positive airway pressure; EEG, electroencephalographic. Values are shown as median (minimum-maximum). Oneway ANOVA on rank, *p < .05, **p < .001, and ***p < .0001.
Effects of CPAP on amplitude of EEG waves during N3 sleep
The amplitude of slower EEG waves (i.e., delta and theta waves) was significantly decreased in the OSAS patients, and increased by CPAP treatment to the level in the normal controls (Figures 4 and 5). Further analysis showed the amplitudes of slow wave activities (i.e., 0.5-2 Hz) were also significantly decreased in OSAS patients and significantly increased by CPAP treatment to the level in the normal controls (Figure 5). CPAP treatment was not associated with significant changes in the amplitude of faster EEG waves (i.e., alpha and beta waves). Examples of EEG waves during NREM sleep stage 3 in normal controls (A), and the OSAS patients without (B) and with CPAP treatment (C). Vertical bars represent 100 μV and horizontal bar represents 2 s. EEG amplitudes of slow wave activities, delta, theta, alpha and beta waves in normal controls (dark grey bars) and the OSAS patients without (light grey bars) and with CPAP treatment (empty bars) during the first (A), second (B) and third (C) sleep cycle of sleep stage N3. CPAP, continuous positive airway pressure. Values are shown as median (minimum-maximum). One-way ANOVA on rank, *p < .05, **p < .001, and ***p < .0001.

Discussion
In the current study, we have systematically investigated whether EEG activities during N3 sleep were altered by CPAP treatment in the OSAS patients and found CPAP treatment significantly increased the percentage and duration of N3 and REM sleep, mean absolute and relative powers, and amplitudes of delta and theta waves during N3 sleep, and decreased the percentage of N1 and the arousal index in addition to improvement of respiration. These findings might contribute to a better understanding of the effects of CPAP treatment on the central nervous system.
CPAP, which involves sustaining pharyngeal transmural positive pressure and increases end-expiratory volume to stabilize the upper airway tract,30,31 has been considered a standard treatment for OSAS patients. 32 The current study confirmed improvement of respiratory variables with CPAP treatment during sleep as shown by increased minimal and mean SpO2 values, decreased time with SpO2 < 90% and decreased AHI to the levels in normal controls. AHI has been found positively correlated with daytime sleepiness 33 and improvement in respiration with CPAP treatment has been shown to be associated with alleviation of daytime symptoms in OSAS patients. 17
In OSAS patients, there were alterations in sleep architecture, namely a relative decrease in slow wave sleep and REM sleep as well as an increase in light sleep in the current study. 34 CPAP treatment was found to reverse these changes by increasing N3 and REM sleep (Table 1), indicating normal sleep structure was significantly restored, which is consistent with the previous report. 35 Additionally, consistent with previous studies,36,37 the number of N3 sleep cycles was significantly increased with CPAP treatment. The increased deep sleep might be related to cognitive function improvements since duration of deep sleep is associated with refreshing effects of sleep. 38 Furthermore, arousals, which were commonly triggered by ventilatory efforts in response to hypoxia, hypercapnia, or inspiratory resistive load, were significantly decreased with CPAP treatment. The number of arousals was found to be a good predictor of daytime sleepiness, and reduced arousals would indicate an improvement in respiration and oxygenation during sleep, which would help to improve patients’ brain function.39–41
OSAS is associated with cognitive function impairments, especially in some severe OSAS patients. 42 Disruptions of slow wave activities were observed in the OSAS patients, which was similar to EEG changes in older adults suffering from cognitive declines such as AD patients. 43 Slow wave sleep was found to be associated with cortical brain volume and loss of slow wave sleep might facilitate brain aging. 44 CPAP treatment was found to improve attention, and executive and memory functions.45,46 In the current study, CPAP treatment increased absolute power ratio of slow to fast EEG waves and relative delta power, and reduced relative powers of theta, alpha and beta waves in the frontal region during N3 sleep (Figure 2D–F and Figure 3), indicating an improvement in sleep quality. In addition, the amplitudes of delta waves (0-4 Hz), slow wave activities (0.5-2 Hz) and theta waves were significantly increased while the amplitude of beta waves were significantly decreased during N3 sleep (Figure 2A–C and Figure 5) with CPAP treatment.
In this study, CPAP treatment increased the spectral power density of slow EEG activities (Figure 1), indicating that CPAP treatment is effective both in reversing respiratory impairments and normalizing EEG patterns during N3 sleep. These changes with CPAP treatment might be associated with improvements in the central nervous system functions such as motor performance, memory, attention, and vigilance. However, some cognitive disabilities still persist even with CPAP treatment.10,47–49 This is consistent with findings that CPAP treatment could only partially improve abnormal auditory event-related potentials, which was linked to attention vigilance and memory, by shortening the N200 and P300 latencies. 50 Furthermore, even in the absence of EDS, nocturnal arousals, major cognitive deficits, and cortical hypometabolism found by magnetic resonance spectroscopy persisted after CPAP treatment, which was likely related to hypoxic damage prior to CPAP treatment. 51
PSA of EEG activity could provide additional information in conjunction with other diagnostic methods for precise diagnosis, assessment of disease severity, and evaluation of treatment response of many central nervous system diseases such as epilepsy, dementia, traumatic brain injury, and neuropsychiatric disorders. 52 In the current study, it was shown that application of PSA of EEG activity in assessment of changes in EEG activities during N3 sleep associated with improvement of hypoxemia in OSAS patients with CPAP treatment. It is likely that PSA of EEG activity during sleep and wakefulness also have potential applications in assessment of disease severity and evaluation of treatment response of respiratory diseases such as chronic obstructive pulmonary disease.
There were some limitations with the study. First, the results were derived only from recordings with F3-A2 derivation, which was located over the frontal gyrus near the sylvian fissure so they could reflect electrical signals from the region of frontal lobe and temporal lobe. 53 As recordings from C3, C4 and O1 and O2 electrodes were not included, recordings derived from these electrodes might produce different results although large distinctions seem unlikely. Second, the age range of the subjects was narrow and sample size of the study was relatively small. Further studies with more PSG recordings on larger number of subjects are needed. Moreover, the effects of CPAP treatment for only one night were tested and long-term effects of CPAP treatment on EEG activities could not be observed in the current study. Third, the power and amplitudes of EEG waves of selected, but not all, EEG segments during N3 sleep were analyzed. Despite these limitations, the impact of CPAP treatment on EEG activities was shown during N3 sleep in the OSAS patients.
Conclusions
Improvement of oxygen supply in OSAS patients with CPAP treatment leads to significant increases in the duration of N3 sleep and the power and amplitude of slower EEG waves during N3 sleep, which indicates an improvement in sleep quality. This study has further confirmed the benefits of CPAP in OSAS treatment and provided evidence for recommendation of CPAP treatment for OSAS patients.
ORCID iD
Dongyuan Yao https://orcid.org/0000-0002-3291-0231
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jiangxi Provincial Natural Science Foundation Grant; Jiangxi Provincial People’s Hospital Grant, Grant number: S2017ZRMSB2145, 2019-009.