
Abstract
We aimed to evaluate and compare the effects of continuous positive airway pressure (CPAP) and mandibular advancement device (MAD) in reducing the intensity of sleep bruxism (SB) in patients with obstructive sleep apnea (OSA). Forty-eight adults with OSA were subjected to single-night full polysomnography (PSG) in the Sleep Laboratory of the Wroclaw Medical University. The respiratory events and bruxism episodes were scored according to the standards of the American Academy of Sleep Medicine. The patients were assigned to the CPAP treatment or the MAD treatment in accordance to apnea–hypopnea index (AHI). The second PSG examination was conducted during the MAD or CPAP treatment to assess the effect of treatment on bruxism episode index (BEI) and AHI. The mean AHI and mean BEI in the study material were estimated to be 30.05 ± 15.39 and 5.10 ± 5.31, respectively. The bruxism parameters were significantly decreased in both the CPAP and MAD groups. Compared to the MAD, the CPAP treatment was more effective in reducing AHI; however, there was no significant difference in effectiveness of CPAP and MAD treatment in BEI reduction. Both CPAP and MAD treatments were effective against SB coexisting with OSA. Due to the application of these treatment options, the risk of OSA should be estimated in patients with SB.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a common respiratory sleep disorder characterized by recurrent partial (hypopnea) or complete (apnea) obstruction of the upper airway during sleep, which results in intermittent hypoxia, arousals, and sleep fragmentation. 1 Recently, it has been estimated that globally 936 million adults, aged 30–69 years, have mild-to-severe OSA. 1 OSA may coexist with other sleep disorders such as insomnia, periodic limb movement disorder, 2 parasomias,3,4 and sleep bruxism (SB). 5 According to the American Academy of Sleep Medicine (AASM), SB can be defined as a “repetitive jaw muscle activity characterized by the clenching or grinding of teeth and/or bracing or thrusting of the mandible.” 6 Furthermore, the international consensus on the assessment of bruxism has defined SB as a “masticatory muscle activity during sleep that is characterized as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals.” 7 The exact prevalence of SB is difficult to determine due to the fact that most population studies use the data collected from self-reported questionnaires, while most bruxers are unaware of their condition. 8 However, it is assumed that the prevalence of SB is 13%. 9
A study reported that 33–50% of subjects with OSA also suffer from SB. 5 A considerable number of risk factors have been identified for SB, which include stress, smoking, caffeine and alcohol consumption, anxiety, use of drugs,10,11 and OSA.12However, the effectiveness of the treatments used for the management of SB is still limited. 13 SB treatment is usually symptomatic and is directed toward teeth protection and pain relief.14,15 Continuous positive airway pressure (CPAP) and mandibular advancement device (MAD) are two effective treatment options available for OSA;16,17 however, CPAP is more effective than MAD in reducing the respiratory events.18–20 Recently, our research group identified that diabetes, 12 hypertension, and hypoxia 21 act as independent risk factors for SB. Among them, hypoxia may be effectively treated using the CPAP or MAD treatment. Therefore, in the present study, we aimed to assess the reduction in SB frequency with the CPAP and MAD treatment in patients with coexisting OSA and SB.
Material and methods
This prospective outcome study was conducted in accordance with the amended Declaration of Helsinki. The study was approved by the Ethical Committee of Wroclaw Medical University (ID KB-195/2017). Written informed consent was obtained from all the patients before inclusion in the study.
A total of 48 adults hospitalized in the Department and Clinic of Internal Medicine, Occupational Diseases, Hypertension and Clinical Oncology of Wroclaw Medical University were included in the study. All these subjects were clinically suspected to have OSA.
The general inclusion criteria were as follows: age between 18 and 90 years, clinical suspicion of OSA, and willingness to participate in the study. The inclusion criteria that were specific to the CPAP treatment were as follows: apnea–hypopnea index (AHI)>15 and consent to undergo this form of treatment. On the other hand, the inclusion criteria that were specific to the MAD treatment were as follows: AHI <15 or >15 and not willing to undergo the CPAP treatment.
The general exclusion criteria of the study were as follows: neurological disorders and/or neuropathic pain, treatment with or addiction to analgesics and/or drugs that affect the muscle functions and breathing, active inflammation, history of pharyngeal surgery for the treatment of OSA, active malignancy and severe mental disorders, and cognitive disability. The exclusion criteria that were specific to the CPAP treatment were as follows: central sleep apnea, obesity hypoventilation syndrome, chronic obstructive pulmonary disease, and congestive heart failure. The exclusion criteria that were specific to the MAD treatment were as follows: severe temporomandibular disorders, limited range of the lower jaw motions, less than eight natural stable teeth in one dental arch, severe gingivitis and/or periodontitis, increased teeth mobility, tooth decays, poor oral hygiene, massive malocclusions, and need for acute dental treatment.
All the included patients underwent a single-night full polysomnography (PSG; first examination) with NoxA1 (NOX Medical, Iceland) in the Sleep Laboratory of the Wroclaw Medical University. Scoring and analysis of the tests were carried out by a qualified, certified physician, following the AASM guidelines, using a Noxturnal system. Polysomnograms were assessed in 30 s epochs in accordance with the 2013 AASM standard criteria for sleep scoring. The PSG outcome variables included sleep latency (SL), total sleep time (TST), sleep efficiency (SE, %), and the percentages of N1 (sleep stage 1), N2 (sleep stage 2), N3 (sleep stage 3), and rapid eye movement (REM) sleep. Abnormal respiratory events were scored based on the pressure airflow signal evaluated in accordance with the standard criteria of the AASM Task Force. 22 The arterial oxygen saturation (SpO2) was measured using finger pulse oximetry. Apnea was defined as the absence of airflow for ≥10 s, while hypopnea was defined as a reduction in the amplitude of breathing by ≥30% for ≥10 s with a ≥3% decline in blood oxygen saturation or arousal.
SB was assessed using bilateral masseter electromyography (EMG) and by audio–video evaluation. Bruxism episode index (BEI) was scored according to the AASM standards. 6 In addition, the three forms of EMG pathways—phasic, tonic, and mixed—were scored. The new SB episodes were scored after at least 3 seconds of stable EMG and when the activity was at least twice the amplitude of the background EMG.22,23 The electrodes were placed on the right and left masseter muscles to measure electromyographic activity. EMF bursts within 3 s were considered part of the same episode. Persistent episodes lasting> 2 s were rated as tonic bruxism and more than three cyclic EMG increases lasting 0.25–2 s as phase bruxism. Episodes combining the features of a tonic episode and a phase episode were assessed as mixed bruxism. Events that mimic sleep bruxism in EMG (e.g., coughing, swallowing saliva, or yawning) after video evaluation were excluded from BEI. BEI is the number of episodes of bruxism (tonic, phasic, and mixed) recorded during the study per hour of sleep. The events during the awake state were not included in the BEI. Based on the BEI, the severity of SB is classified as follows: BEI <2 not significant, BEI = 2–4 mild, or moderate or BEI> 4 severe.
Participants with an AHI of >15per hour were assigned to the CPAP treatment and were connected with an auto-adjusting CPAP machine (Autoset S8, ResMed, Abingdon, UK). The second PSG examination was conducted during the CPAP treatment in the Sleep Laboratory of the Wroclaw Medical University. Automatic titration was performed to eliminate respiratory events.
Participants with an AHI of <15per hour were assigned to the MAD treatment. For these subjects, protrusion was individually adjusted up to 65% of the possible maximum. The custom, titratable MAD was manufactured by a qualified dentist. The second PSG examination was conducted using MAD in the Sleep Laboratory of the Wroclaw Medical University.
Participants who had an AHI of >15 and were not willing to undergo the CPAP treatment were also assigned to the MAD treatment. One patient, who was initially assigned to the CPAP treatment, withdrew after the first night of the treatment and was then assigned to the MAD treatment. The recruitment process is shown in Figure 1. Scheme of subjects’ recruitment to the CPAP and MAD groups. CPAP: continuous positive airway pressure, MAD: mandibular advancement device, AHI: apnea–hypopnea index, PSG: polysomnography, OSA: obstructive sleep apnea.
The second polysomnography with CPAP or MAD treatment was conducted 10–12 weeks after baseline polysomnography. In MAD group, the PSG was conducted a week after completed MAD adjustment. In CPAP group, the effect of CPAP was assessed during first night of device treatment.
Statistical analysis was performed using the Statistica 12 software developed by StatSoft (Dell Inc., USA). The normality of distribution of all the parameters was analyzed using the Shapiro–Wilk test. The significance of mean differences between two groups (intergroup differences) was determined using the standard Student t-test for the parametric data and the Mann–Whitney U test for the nonparametric data. The significance of mean differences for the dependent variables (measured before and during treatment) was determined using the Student t-test for the parametric data and the Wilcoxon signed-rank test for the nonparametric data. Correlation analysis was performed with Spearman’s rank correlation test. The relationships between the analyzed variables were determined also by multivariable stepwise regression analysis. Statistical significance was set at p < 0.05 for all the tests.
Results
Baseline polysomnographic parameters evaluated in the entire group, CPAP group, and MAD group.

CPAP: continuous positive airway pressure, MAD: mandibular advancement device, BEI: bruxism episode index, AHI: apnea–hypopnea index, ODI: oxygen desaturation index, TST: total sleep time, SL: sleep latency, REML: REM latency, WASO: wake after sleep onset, SE: sleep efficiency, N1: sleep stage 1, N2: sleep stage 2, N3: sleep stage 3, R: rapid eye movement sleep stage, ArI:arousal index, mean SpO2: mean oxygen saturation, minute. SpO2: minimal oxygen saturation, mean desat, mean desaturation; *p statistically significant.
Effect of the MAD and CPAP treatment on sleep bruxism parameters.

CPAP: continuous positive airway pressure, MAD: mandibular advancement device, BEI: bruxism episode index; *p statistically significant.
Sleep and respiratory parameters in the CPAP group (n = 30) and MAD group (n = 19).

CPAP: continuous positive airway pressure, MAD: mandibular advancement device, AHI: apnea–hypopnea index, ODI: oxygen desaturation index, TST: total sleep time, SL: sleep latency, REML: REM latency, WASO: wake after sleep onset, SE: sleep efficiency, N1: sleep stage 1, N2: sleep stage 2, N3: sleep stage 3, R: rapid eye movement sleep stage, ArI: arousal index, mean SpO2: mean oxygen saturation, minute. SpO2: minimal oxygen saturation, mean desat, mean desaturation; *p statistically significant
Due to the baseline differences in the MAD and CPAP groups, the effects on sleep and respiratory parameters were compared in only patients with an AHI of >15 (Supplementary Table B). The CPAP treatment was found to be more effective in decreasing AHI, ODI, snoring, and mean O2 saturation (Supplementary Table B, Figure 2), whereas the MAD treatment was more effective in decreasing BEI and phasic BEI (Table 4, Figure 3). AHI reduction in the study groups. The graph present data from entire study group: CPAP group (n = 30) and MAD group (n = 19). CPAP: continuous positive airway pressure, MAD: mandibular advancement device, AHI: apnea–hypopnea index. Comparison of the effectiveness (Δ of bruxism parameters) of the CPAP (n = 30) and MAD (n = 19) treatment. CPAP: continuous positive airway pressure, MAD: mandibular advancement device, BEI: bruxism episode index. BEI reduction in the study groups The graph present data from entire study group: CPAP group (n = 30) and MAD group (n = 19). Caption: CPAP: continuous positive airway pressure, MAD: mandibular advancement device, BEI: bruxism episode index.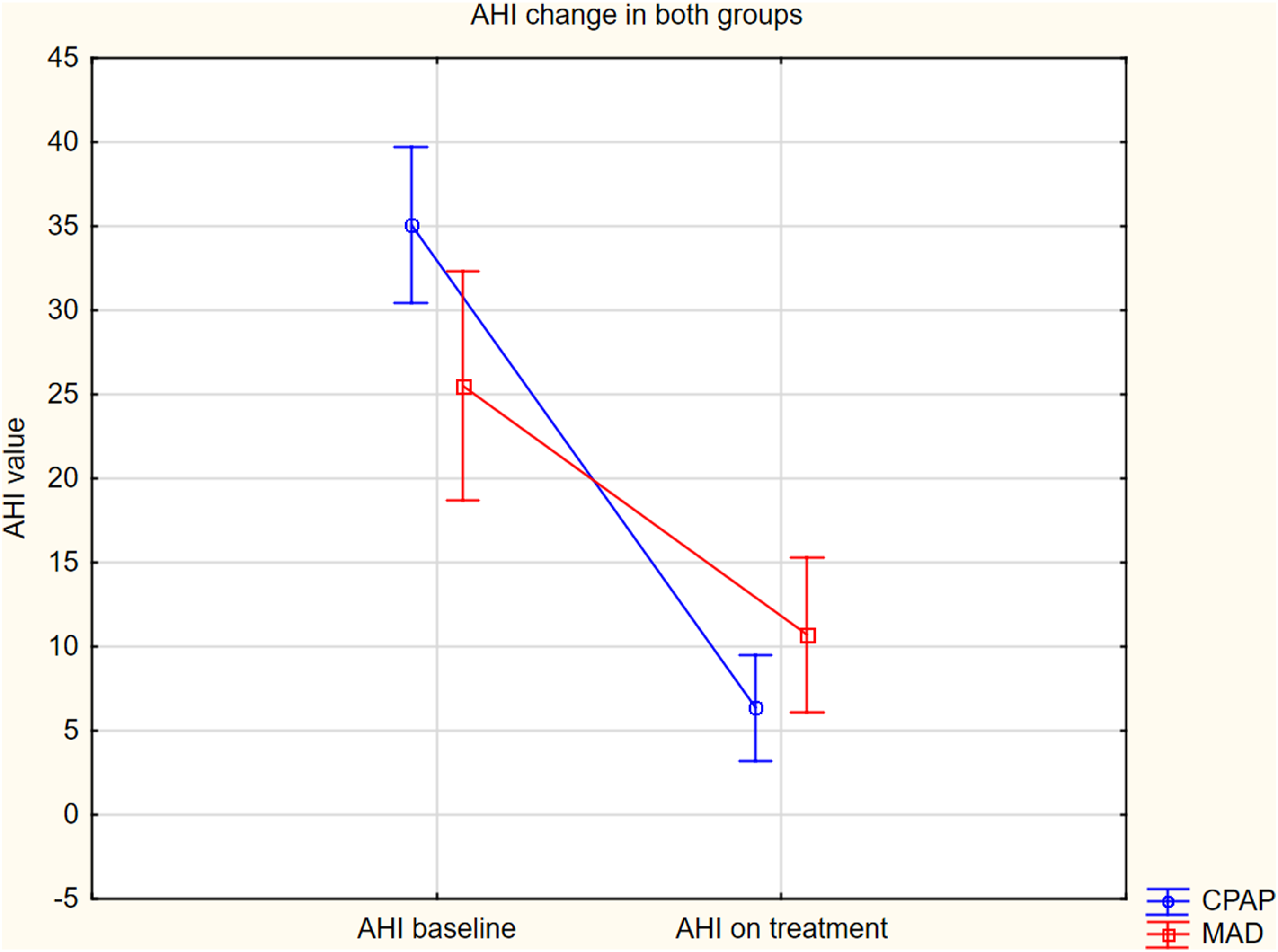


Furthermore, we studied the correlations between the differences in BEI and sleep and respiratory parameters in the entire studied group. We observed a negative correlation between the reduction in BEI (ΔBEI) and AHI (ΔAHI) (r = −0.28, p = 0.04), ΔBEI and Δsnoring (r = −0.29, p = 0.04), and ΔBEI and ΔSE (r = 0.37, p = 0.01). In addition, a positive correlation was observed between ΔBEI and ΔSL (r = 0.30, p = 0.04).
In the next step, we examined the correlation in the group with AHI >15. We observed a positive correlation between ΔBEI and an increase in minimal oxygen saturation (r = 0.30, p = 0.05), whereas a negative correlation between ΔBEI and an increase in average desaturation (r = −0.31, p = 0.04).
Then we conducted multivariable stepwise regression analysis and determined factors independent of the BEI and AHI decrease after treatment.
For the “BEI decrease after treatment” variable the following relationship model was obtained: BEI decrease after treatment = 0.041 age—1.207 diabetes + 0.919 BEI before treatment—0.088 mean SpO2 before treatment + 0.068 mean heart rate (HR) before treatment. Multivariable analysis showed that older age, higher BEI before treatment, and higher average pre-treatment HR are independently associated with greater BEI decrease after treatment. Diabetes and higher mean SpO2 before treatment are independent factors associated with lower BEI decrease after treatment. The method of treatment (CPAP vs MAD) does not affect BEI decrease after treatment independently of other factors.
For the “AHI decrease after treatment” variable the following relationship model was obtained: AHI decrease after treatment = 5.213 CPAP treatment (yes)/MAD treatment (no) + 8.482 male sex + 0.606 AHI before treatment—0.521 BEI before treatment—0.367 minimum SpO2 before treatment. Multivariable analysis showed that for CPAP treatment (compared to MAD treatment) male gender and higher AHI before treatment are independently associated with greater drops in AHI after treatment. Higher pre-treatment BEI and higher pre-treatment minimum SpO2 are independent factors associated with smaller post-treatment AHI decreases.
Summarizing, based on multivariable stepwise regression analysis, it can be stated that the choice of treatment method (CPAP vs MAD) is significant in the context of the greater impact of CPAP on AHI decrease, while it is not significant in the context of BEI decrease (Supplementary Table C).
Discussion
The most important observation of our study was the reduction of BEI in both the CPAP and MAD group. This confirmed that both CPAP and MAD might be effective in the management of SB. However, we have assessed the CPAP effectiveness in the first single night, therefore, long-term effects can be different. There were no significant differences in effectiveness between these two treatment methods. Oksenberg and Arons as well as Martinot et al. described that severe OSA cases with bruxism were successfully treated with CPAP.24,25 Furthermore, different types of oral devices have been shown to reduce bruxism episodes.26,27 Some studies have confirmed the higher efficacy of MAD in reducing SB episodes compared to occlusal splints.28–30 However, the groups were commonly not large, CPAP was not studied, intraoral appliances were used because of occurrence other medical conditions, or study was not conducted in a sleep laboratory. Therefore, we cannot compare these results with those of the present study. Moreover, no large, reliable clinical trials have been carried out on bruxism management with CPAP and MAD thus far. In the present study, we have evaluated and compared the reduction in SB frequency with the CPAP and MAD treatment in patients with coexisting OSA and SB.
SB is a common sleep phenomenon, frequently co-occurring with other sleep disorders such as periodic limb movement disorder, 31 catathrenia, 32 sexsomnia, 33 and sleep-related breathing disorders.34,35 Although the relationship between OSA and SB remains controversial, the hypothesis that SB can act as a protective factor of OSA is fairly accepted. 36 Currently, there are ineffective treatments available for SB, and certain pharmacological, psychological, and dental strategies and rehabilitation techniques are used to manage the condition. Because of its complex underlying mechanism, treatment schemes based on a single method are usually not sufficient to treat SB.
Recently, the relationship between SB and hypoxia has been receiving much attention. Hypoxia, which is considered as a new risk factor for SB, may be a promising treatment goal in patients with OSA and SB. Dumaiset al. demonstrated that minor transient hypoxia is potentially associated with the onset of bruxism episode, independent of concomitant sleep arousal or body movements. 37 Interestingly, mild transient hypoxia observed before the onset of bruxism episode was not found to be linked to changes in the end-tidal CO2. 38 Recently, our research team showed that AHI, lower mean SpO2, and higher SpO2percentage (<90%) constituted independent risk factors for an increase in BEI.21Considering these data, we looked for a relationship between the reduction of BEI and changes in the PSG parameters and observed that there were correlations between the reduction in BEI and AHI, SL, and SE in the entire study group. In the group with AHI>15, we observed a positive linear correlation between BEI reduction and an increase in minimal oxygen saturation, whereas a negative linear correlation between BEI reduction and an increase in average desaturation. These observations suggest that improvement of oxygen saturation might be responsible for the reduction in BEI during the treatment of OSA; however, causality cannot be assumed and futher studies are needed to clear the effect of oxygen saturation variability on bruxism intensity.
In the present study, we have observed reduction of frequency of AHI, ODI, snoring, arousal index (ArI), N1 duration (% of TST), percentage of sleep with oxygen saturation <90%, and mean desaturation value during the first night of CPAP treatment. CPAP also increased mean oxygen saturation, minimal oxygen saturation, and N3 duration (% of TST). However, SL was found to be increased and SE and TST were decreased compared to the first diagnostic PSG. This adverse effect of CPAP on sleep can be related to the fact that the assessment was made during the first night of the CPAP treatment. It is well known that CPAP tolerance may be poor on the first night of treatment. In the case of the MAD treatment, a reduction in AHI, ODI, snoring, N1 duration, ArI, percentage of sleep with oxygen saturation <90%, and an increase in mean desaturation and N3 duration were noted. However, no effect was observed on mean oxygen saturation. In addition, there was no adverse effect on SL, SE, and TST, which confirms the better tolerance of the MAD treatment, compared to CPAP. 39 Furthermore, the CPAP treatment was more effective in reducing AHI, while both treatment methods were similarly effective in reducing BEI. Both CPAP and MAD were effective in bruxism episodes count reduction; however, some residual SB episodes were observed. The clinical significance of residual SB episodes remains unclear and further studies are needed.
Although MAD is considered better tolerated treatment than CPAP, it may result in excessive salivation. On the other hand, sleep bruxism is concerned as protective mechanism of mouth dryness, 40 thus this side-effect of MADs might result in effective bruxism reduction. However, salivation was not investigated in this study and the exact mechanism supporting bruxism reduction remains to be explained.
The importance of the bruxism phenotypes is not well understood. Episodes of bruxism in SB patients are more often phased or mixed, while in healthy subjects tonic is more common. 41 Increased severity of phasic bruxism was observed in hypertensives, while the tonic activity was similar in hypertensives and normotensives. 21 The SB-type phase frequency correlated positively with the frequency of obstructive apnea and oxygen desaturation. 34 Therefore, phasic episodes may be associated with OSA and hypertension. In the present study, MAD was more effective than CPAP in total reduction of BEI and phasic BEI; however, multivariable stepwise regression analysis showed that both treatments were similarly effective in reducing bruxism episodes.
To our best knowledge, this is the first clinical study on the treatment of SB using CPAP, which demonstrated the effectiveness of CPAP and MAD in the management of this condition. However, the study has some limitations. First, the MAD group was relatively small and consisted mostly of patients with moderate OSA. Second, the efficacy of the CPAP treatment was measured on a single initial overnight study on the first night of treatment and we do not know if benefit would be sustained and therefore, the later outcomes might differ.
We cannot also exclude selection biases for patients opting for CPAP versus MAD treatment. Another serious limitation was lack of randomization. The patients in the CPAP and MAD groups were not matched for OSA severity.
Conclusion
Both CPAP and MAD might be effective in the reducing of SB events coexisting with OSA at the initial stage of using the device. CPAP is more effective in improving sleep and respiratory parameters. There is no statistically significant difference in effectiveness of MAD and CPAP in reducing the number of bruxism episodes. However, future studies are needed to assess the effectiveness of CPAP and MAD after following months of treatment.
Supplemental Material
sj-pdf-1-crd-10.1177_14799731211052301 – Supplemental Material for The effect of continuous positive airway pressure and mandibular advancement device on sleep bruxism intensity in obstructive sleep apnea patients
Supplemental Material, sj-pdf-1-crd-10.1177_14799731211052301 for The effect of continuous positive airway pressure and mandibular advancement device on sleep bruxism intensity in obstructive sleep apnea patients by Helena Martynowicz, Tomasz Wieczorek, Piotr Macek, Anna Wojakowska, Rafał Poręba, Paweł Gać, Grzegorz Mazur, Robert Skomro, Joanna Smardz and Mieszko Więckiewicz in Chronic Respiratory Disease
Footnotes
Author Contributions
HM and MW contributed to the study conception; HM and MW designed the study; PM, TW, AW, JS, RP, PG, and HM were responsible for data acquisition and analysis; HM, MW, RP, and TW interpreted the data; HM, MW, TW, and JS prepared the manuscript draft; MW, GM, and RS revised the draft; MW and HM supervised the study. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was co-financed by the Grant of Wroclaw Medical University (SUB-A210.19.053). The funding source was not involved in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.