
Abstract
Exercise-induced oxygen desaturation (EID) is prevalent in people with chronic obstructive pulmonary disease (COPD). This article reports a sub-analysis from a randomized controlled trial (RCT) in people with COPD and EID (COPD/EID). The primary aim, in people with COPD/ EID, was to determine the repeatability of the distance and time walked in the incremental shuttle walk test (ISWT) and endurance shuttle walk test (ESWT), respectively. A secondary aim was to determine whether any participant characteristics predicted those who did not demonstrate improvements on a repeat ISWT or ESWT. Participants with nadir oxygen saturation (SpO2) < 90% on the 6-minute walk test were recruited to the RCT. Two ISWTs and two ESWTs were then performed as part of the baseline assessments, and participants were included in this sub-analysis if their nadir SpO2 was <90% during the better of two ISWTs. Repeatability of the tests was analysed using Bland–Altman plots and paired t-tests. Participant characteristics of age, lung function, level of nadir SpO2 and end-test dyspnoea were used to predict those who were not likely to demonstrate improvements on a repeat test using receiver operating curves. Eighty-seven participants (mean age (standard deviation, SD) 70 (7) years; forced expiratory volume in one second (FEV1) 47 (17)% predicted) were included. The mean differences (coefficient of repeatability) for the ISWTs and ESWTs were 9 m (55 m) and 19 seconds (142 seconds) respectively (p < 0.05). No participant characteristic predicted the absence of improvement on the second ISWT (area under the curve (AUC) ranged from 0.49 to 0.58, all p > 0.2) or the second ESWT (AUC ranged from 0.43 to 0.52, all p > 0.3). Although repeating the tests showed only small improvements in distance (ISWT) and time (ESWT) walked in people with COPD/EID, the variability was large making definite conclusions about test repeatability in these individuals difficult.
Keywords
Introduction
Field walk tests such as the six-minute walk test (6MWT), incremental shuttle walk test (ISWT) and endurance shuttle walk test (ESWT) are commonly used in the assessment of exercise tolerance in people with chronic obstructive pulmonary disease (COPD). Exercise-induced oxygen desaturation (EID) during field walk tests is common in people with COPD. A few studies 1 –3 showed that between 47% and 74% of patients referred to pulmonary rehabilitation demonstrated a nadir oxygen saturation (SpO2) during 6MWT of <90%. Although the definition of EID that is clinically important for people with COPD has not been determined, it is often reported as a decline in SpO2 of ≥4% or >4% to <90% during a 6MWT. 1,2
The reliability of field walk tests, such as the ISWT and ESWT, is well established. 4,5 The recent technical standards for field walk tests for people with stable COPD 4 recommended the need to account for improvements that result from test familiarization during the ISWT by recording the better result of two tests. Whether people improve with test familiarization on the ESWT was less clear. 4 The repeatability of the ISWT and ESWT has not been investigated in the subgroup of people with COPD who demonstrate EID (COPD/EID). Given that EID in people with COPD is common, 1,2 and field walk tests are regularly used as part of exercise assessment in rehabilitation programs and to determine the need for ambulatory oxygen therapy in this group, a better understanding of the need to repeat these field walk tests in this subgroup is warranted. There is a possibility that the learning effect in performance of the ISWT and ESWT is not as pronounced in this subgroup as they may experience primarily symptom limitation associated with EID, such as dyspnoea and/or fatigue, to end the test rather than test termination being associated with lack of familiarization. If the learning effect is not as pronounced in those with COPD/EID, there could be resource implications and repeating the walk tests may not be required. It would also be useful for clinicians to know if any patient characteristics could predict those who are not likely to demonstrate improvements on a repeat test in this subgroup; however, this has not been previously determined.
This article reports a sub-analysis from a larger randomized controlled trial (RCT) where people with COPD/EID were recruited. The primary aim of this sub-analysis was to determine the repeatability of the distance and time walked in the ISWT and ESWT, respectively. A secondary aim was to determine whether any participant characteristics predicted those who did not demonstrate improvements on a repeat ISWT or ESWT.
Methods
Participants
Measurements collected during the baseline assessment conducted for a multi-centre RCT were used to address the aims in this sub-analysis. People with COPD were recruited from referrals to pulmonary rehabilitation programs at seven Australian sites (Royal Prince Alfred Hospital, New South Wales (NSW); Concord Repatriation General Hospital, NSW; Liverpool Hospital, NSW; Austin Health and Alfred Health, Victoria; Sir Charles Gardiner Hospital, Western Australia; Prince Charles Hospital, Queensland) and were screened using a 6MWT to ensure evidence of EID (i.e. SpO2 < 90% during the 6MWT performed on room air). The additional inclusion and exclusion criteria for the RCT have been reported previously. 6 For inclusion in these sub-analyses, participants were required to also demonstrate EID during the ISWT (one of two) in which the greater distance was achieved (i.e. SpO2 < 90%). This study was performed with approval from the Ethics Committee of all participating sites and all participants provided written informed consent. The trial was registered with Australian New Zealand Clinical Trials Registry: ACTRN12612000395831.
Measurements
Participants’ age, height, weight, spirometry, lung volumes and diffusing capacity were measured at baseline according to standard protocols. 7
The ISWT and ESWT were performed according to the published protocols. 8,9 Each participant performed two ISWTs on the same day and two ESWTS on another day, within 7 days of the initial ISWTs. Participants rested for at least 30 minutes between tests or until SpO2, Borg dyspnoea score and heart rate returned to resting levels. Heart rate and SpO2 were continuously monitored for all tests using a portable oximeter (RAD-5v Masimo Corp., Irvine, California, USA) and recorded each minute. Additionally, dyspnoea and rate of perceived exertion (RPE) were measured at the beginning and end of all tests using a modified Borg 0–10 scale. 10,11 The initial speed for the ESWT was calculated as 85% of the peak speed that participants achieved on the ISWT. 12 As the ESWT was the primary outcome for the RCT, during baseline testing, if the initial ESWT test time exceeded 8 minutes and the participant showed minimum signs of exertion or breathlessness, the test was terminated and the speed was increased to the next level for the repeat test. However, for the sub-analyses related to ESWT, only data from those participants who performed both baseline tests at the same speed were included.
Power
The sample available for these analyses (n = 66) provided adequate power (1 − β = 0.8, α = 0.05) to detect a within-participant mean difference in performance on the ISWT or ESWT that was equivalent to a moderate effect size or greater (i.e. an effect size ≥0.35 of a SD from the mean). This sample size was also sufficient to detect an area under the receiver operating characteristic (ROC) curve of 0.7, for predictors used to separate those who did versus did not improve their performance on the second ISWT or ESWT.
Statistical analysis
Data were analysed using SPSS version 22 (SPSS Inc., Chicago, Illinois, USA). Repeatability of the walk tests was analysed using the methods of Bland and Altman. 13 For the ISWT and ESWT repeatability, the mean difference was calculated between the first and second tests, and the coefficient of repeatability (CR) was calculated as the product of 1.96 and the SD of the mean difference. The CR provides the limits of agreement around the mean difference within which 95% of the mean difference values will be included. For both the ISWT and ESWT, paired t-tests were used to determine whether the measures (distance, time, cardiorespiratory responses and symptom scores) differed significantly between the first and second tests. ROC curves were used to assess whether there was an optimal cut-point value in the continuous variables of interest (i.e. age, FEV1% predicted, end-test dyspnoea, end-test RPE and nadir SpO2 during the first ISWT or ESWT) that would separate those participants who did versus did not improve on their second ISWT or ESWT. Participants were grouped as ‘no improvement on the second test’ if there was no improvement or a deterioration between the first and second tests or ‘did improve on a second test’ if there was any improvement >0 m between the first and second tests. χ 2 tests were used to assess whether gender was associated with group membership. For all analyses, p values <0.05 were considered significant.
Results
Eighty-seven participants met the inclusion criteria for the study. Their characteristics are presented in Table 1. Eighty-four participants desaturated on both ISWTs, with the three participants who only desaturated on one test having a nadir SpO2 of 91% on the other test. For the ESWT, 66 of the 87 participants had data on two tests at the same walking speed and their characteristics are also presented in Table 1. Of the 66 participants, 61 participants (92%) demonstrated a nadir SpO2 < 90% on at least one of the ESWTs.
Characteristics of participants involved in the ISWT and ESWT analysis.a
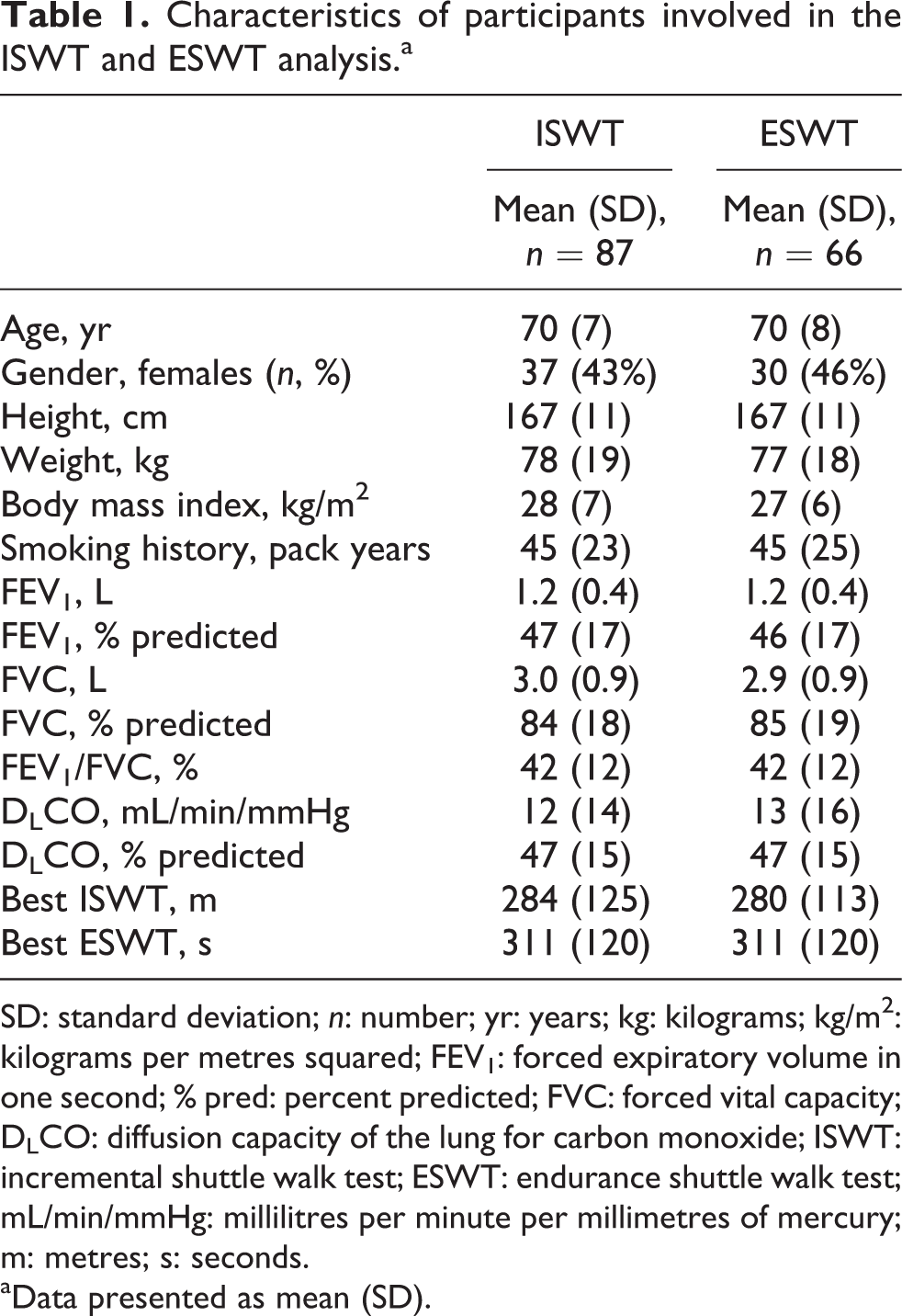
SD: standard deviation; n: number; yr: years; kg: kilograms; kg/m2: kilograms per metres squared; FEV1: forced expiratory volume in one second; % pred: percent predicted; FVC: forced vital capacity; DLCO: diffusion capacity of the lung for carbon monoxide; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; mL/min/mmHg: millilitres per minute per millimetres of mercury; m: metres; s: seconds.
aData presented as mean (SD).
The repeatability of performance and cardiorespiratory responses for the repeat ISWTs and ESWTs are presented in Table 2. For the ISWT and ESWT, the mean differences between the first and second tests (CR) were 9 m (55 m) and 19 seconds (142 seconds), respectively (both p < 0.05). Bland–Altman plots are presented in Figure 1. The end-test cardiorespiratory responses were similar for the two ISWTs and the two ESWTs except for end-test dyspnoea score which was statistically higher on the second test for both the ISWT and ESWT (Table 2).
Exercise performance, cardiorespiratory and symptoms responses during ISWT and ESWT.a

bpm: beats per minute; CI: confidence interval; CR: coefficient of repeatability; ESWT: endurance shuttle walk test; HR: heart rate; ISWT: incremental shuttle walk test; RPE: rate of perceived exertion; SD: standard deviation; SpO2: oxygen saturation.
aData presented for test 1 and test 2 presented as mean (SD).
bSignificantly different between the first and second ISWT or ESWT (p < 0.05).

Bland–Altman plots (a) difference in distance walked in ISWT and (b) difference in time walked in ESWT. Mean difference shown as solid line, 95% limits of agreement as dashed lines (1.96 × SD). ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; SD: standard deviation.
Table 3 presents the ROC curves generated for variables that may have predicted participants who improved versus did not improve on their second ISWT or ESWT. No participant characteristic predicted which participants did not demonstrate an improvement on the second test for the ISWT (area under the curve (AUC) ranged from 0.49 to 0.59, all p > 0.1) or for the ESWT (AUC ranged from 0.43 to 0.52, all p > 0.3). Notably, gender was also not associated with those who did not need a second test for the ISWT (p = 0.1) or ESWT (p = 0.2).
Determination of whether participant characteristics predict those who do not need to do a second test for the ISWT or ESWT.
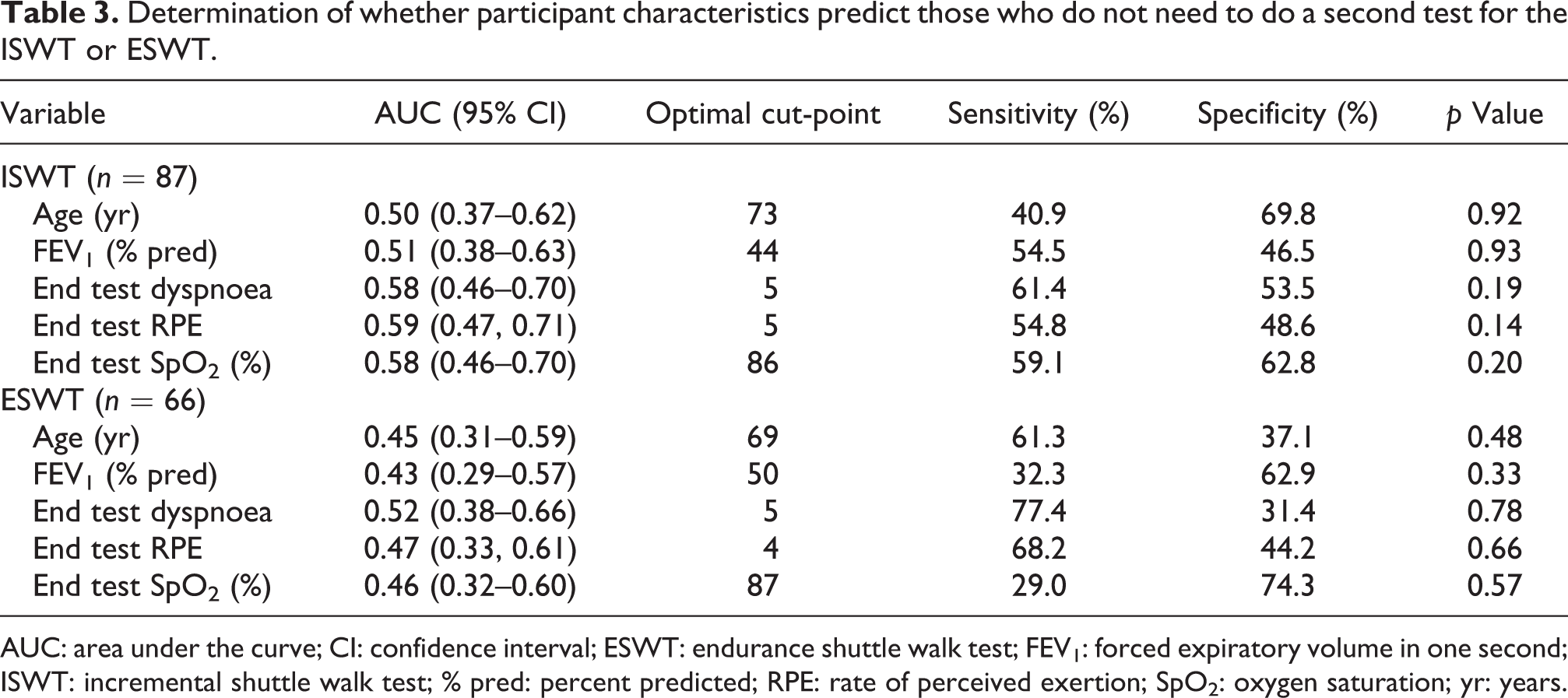
AUC: area under the curve; CI: confidence interval; ESWT: endurance shuttle walk test; FEV1: forced expiratory volume in one second; ISWT: incremental shuttle walk test; % pred: percent predicted; RPE: rate of perceived exertion; SpO2: oxygen saturation; yr: years.
Discussion
To our knowledge, this is the first study to investigate the repeatability of the ISWT and ESWT in people with COPD/EID. The main findings of this study were that the distance walked in the ISWT and the duration of walking in the ESWT showed only small differences between the first and second tests. In addition, there was a statistically significant difference with the end-test dyspnoea score for the ISWT and ESWT with repeat testing, but the difference was only small and not clinically relevant. 14 While these main findings might suggest that repeat tests are not needed for a group of people with COPD/EID, the coefficient of repeatability was wide, indicating variability in individual responses. We were not able to identify any participant characteristics that could predict those who did not demonstrate improvement on a second test.
This study has shown that people with COPD/EID walk significantly further and longer on a second test for the ISWT and ESWT, respectively, but the overall mean difference was small (ISWT = 9 m; ESWT = 19 seconds). Interestingly, this amount of difference was lower than that reported for people with COPD without specified EID (20–25 m on the ISWT and 26 seconds on the ESWT). 4 No study has previously reported on repeatability of the ISWT and ESWT in a large group of people with COPD/EID. One study discussed a subgroup analysis involving people with COPD/EID when reporting the repeatability of the ISWT in people with COPD and showed a difference of 26.5 m between repeat ISWTs in this subgroup. 15 The details provided about the participants in this subgroup analysis were inadequate to enable comparison with the current study.
When reviewing the Bland–Altman plots for both the ISWT and ESWT, the mean differences were small but the upper bounds of the CR were high being 64 m for the ISWT and 161 seconds for the ESWT indicating that some participants had large differences between repeat tests. The proportion of the sample who demonstrated an improvement in ISWT and ESWT on repeat testing was 49% and 53%, respectively (Figure 1(a) and (b)). In stable COPD, it has been suggested that two tests are required for the ISWT in order to account for the learning effect but that one test may be sufficient for the ESWT. 4 As approximately 50% of the group improved on either the ISWT or ESWT with repeat testing, it seems that repeat testing is needed in order to adequately interpret changes in these measures following an intervention.
Understanding whether there are any participant characteristics that can be used to predict who does not demonstrate an improvement on a second ISWT or ESWT would be useful to guide clinicians in their decisions about who requires repeat testing. Obviously, this issue has resource and time implications for assessment clinics or rehabilitation programs. The results of the ROCs in this study for age, FEV1 (%predicted), end-test dyspnoea, end-test RPE and nadir SpO2 during the first ISWT or ESWT indicated AUC values were <0.6 and not significant, suggesting that no participant characteristic was able to predict lack of improvement on a second test.
One of the limitations of this study was that results may have been affected by order bias, as testing sequence was standardized rather than random. In addition, this study has only demonstrated the size of the learning effect in the ISWT and ESWT before exercise training in people with COPD/EID. The learning effect in ISWT and ESWT after exercise training in people with COPD/EID remains unknown. In this study, all testing took place on room air so conclusions can only be made about repeat testing on room air. Given that tests such as the ESWT may also be used to determine response to ambulatory oxygen in people with COPD/EID, in future studies, it would be important to identify whether repeat testing is needed under these conditions.
Conclusion
In a group of people with moderate to severe COPD with EID, repeating the ISWT and the ESWT resulted in only small improvements in walk distance and walk time, respectively. However, the wide CR coupled with the inability to use participant characteristics to predict those who did not improve on repeat testing make conclusions on whether repeat testing should be performed for any given individual with COPD/EID difficult.
Footnotes
Acknowledgements
The authors would like to acknowledge all the assessors at each research centres for their contribution to the study. They would also like to acknowledge Jenny Peat who provided statistical analysis advice.
Authors’ note
Lissa Spencer is now affiliated to Department of Physiotherapy, Royal Prince Alfred Hospital, Missenden Road, Camperdown, New South Wales, Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by Australian Government National Health and Medical Research Council.