
Abstract
Patients with chronic obstructive pulmonary disease (COPD) who have nocturnal oxygen desaturation (NOD) can be treated with nocturnal oxygen therapy (NOT) to avoid possible morbidity and mortality. Although there is no definite data recommending NOT alone, our aim is to evaluate the relationship between desaturation during the six-minute walk test (6MWT) and NOD in COPD. Fifty-five stable patients with COPD were enrolled in this study. The 6MWT and nocturnal oximetry were performed. Patients with comorbid diseases and respiratory failure were excluded. In total, 55 patients (49 males and 6 females, mean age: 65.8 ± 8.4 years) were analysed. Twenty-seven of the patients had moderate COPD and the remainder (n = 28) had severe COPD. Three patients (11%) with moderate COPD and 12 patients (42.9%) with severe COPD desaturated during 6MWT (p = 0.003). NOD was observed in five patients with severe COPD (17.9%). There were no patients with NOD in the moderate COPD group. Three (25%) of patients with severe COPD who desaturated during the 6MWT also had NOD. NOD was more common in patients with severe COPD and the patients with higher carbon dioxide levels (p = 0.02 and p = 0.001). Three patients (11%) with moderate COPD desaturated during the 6MWT; however they did not have NOD. Although the sample size in this study was too small to be conclusive, NOD was more common in desaturators during the 6MWT particularly in patients with severe COPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide. 1 –3 The quality of life is poor in the vast majority of patients with COPD, and these patients die at early ages. 4 Morbidity and mortality are mostly due to respiratory failure and its complications. 5 Patients with moderate and severe COPD suffer from hypoxaemia. 6,7 In previous studies, long-term oxygen therapy (LTOT) has been reported to reduce mortality in COPD patients with respiratory failure; therefore, early identification of individuals for LTOT is important. 8 –10 Some patients with COPD may desaturate only during exercise or sleep. Current guidelines do not recommend nocturnal oxygen treatment (NOT) for patients with nocturnal oxygen desaturation (NOD) accompanied by daytime normoxaemia. The clinical importance of NOD is unclear in the literature, and there is a need for studies to understand complications and results of NOD. Nocturnal oximetry is used for evaluating NOD, which is a process that requires overnight monitoring. It is also time-consuming due to staff time. This study was designed to investigate the utility of the 6-minute walk test (6MWT), a more practical test, instead of nocturnal oximetry for identifying patients who have NOD. Our aim was to evaluate whether desaturation during 6MWT was useful in predicting NOD at different stages of COPD.
Methods
The study was performed between September 2011 and June 2012 in the Pulmonology Department of our university. Patients with moderate and severe COPD who were not hypoxaemic at rest were included in this study. Patients were excluded if they had a history of acute exacerbation of COPD in the previous month, respiratory failure, were on LTOT or noninvasive mechanical ventilation, had clinically decompensated heart failure (newly developed peripheral oedema, orthopnoea and paroxysmal nocturnal dyspnoea) or were known or suspected to have obesity hypoventilation/obstructive sleep apnoea syndrome. Suspicion of obstructive sleep apnoea syndrome depended on having cardinal symptoms (snoring, witnessed apnoea and excessive daytime sleepiness) and an Epworth Sleepiness Scale score ≥10. Body mass index (BMI) was calculated using the formula: weight (kg)/height 2 (m2). 11 Patients with BMI ≥35 and partial arterial carbon dioxide (paCO2) >45 mmHg were excluded from the study to exclude possible sleep disorders. COPD diagnosis and disease severity were determined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guideline criteria. 12 According to the GOLD guideline criteria, patients were classified as moderate (stage II) COPD if postbronchodilator forced expiratory volume in one second (FEV1) was 50–80% of predicted and as severe (stage III) COPD if FEV1 was 30–50% of predicted values.
All patients underwent spirometry, carbon monoxide diffusion test (DLCO), arterial blood gas analysis (ABG) at rest under normal room air conditions. In order to evaluate the severity of dyspnoea, modified Medical Research Council (mMRC) and Modified Borg dyspnoea scales were used. 13,14 Spirometry and DLCO tests were performed using Zan 100 MGA USB Pulmonary Function Device (No:130033, Zan Messgerate, Germany) in accordance with approved standards. 15 ABG was performed in the room air after 15 minutes rest using a Cobass b 221 System (Roche Inc., Pleasanton, California, USA). The 6MWT was performed in accordance with the American Thoracic Society guidelines. 16 The 6MWT was performed in a 30-metre long, straight corridor under the guidance of a single respiratory physiotherapist. There was no practice test prior to 6MWT, but our physiotherapist showed each patient how to walk and turn after a lap was completed. During the exercise, the physiotherapist informed the patients when each minute had elapsed and encouraged them to continue. Oxygen saturation during the test was recorded using the finger probe of a portable pulse oximeter (VM 2160 pulse oximeter, Viamed, UK). During this process, baseline and end 6MWT values of blood pressure, pulse rate, peripheral oxygen saturation (SpO2), Borg dyspnoea scale and mMRC scores of the patients were recorded. At the end of the test, the 6-minute walk distance (6MWD) was recorded. Oxygen desaturation during exercise was defined as a fall in SpO2 of ≥4% to a value <90% which was measured using a pulse oximeter at baseline and at the end of the 6MWT. 17 The test was stopped when the saturation dropped below 90% if subjects were exhausted or had intolerable dyspnoea. Patients were asked to rate their perceived dyspnoea on a 10-point Borg scale prior to and immediately after completion of the 6MWT. The 6MWTs were performed in the daytime, prior to the sleep study, which was conducted on the same day. For the nocturnal oximetry study, we used a pulse oximeter (model MD300K12 SN: 09172090018, Choicemmed, China), which records pulse and saturation every 4 seconds. The patients spent one night at our sleep laboratory for nocturnal oximetry study. The mean and lowest overnight saturation and time spent with saturation <90% were recorded. NOD was considered when the time spent with saturation <90% was recorded as ≥30% of total sleep time. The study was carried out according to the principles of the Helsinki Declaration. All subjects gave informed consent to the study. The study was approved by the Istanbul Medical Faculty Institutional Board Ethics Committee (approval number: 2011/1405-661), Istanbul University, Istanbul, Turkey.
Statistical analysis
Statistical analysis was performed by using Statistical Package for Social Sciences 17.0 software package program. Descriptive values were given as mean, standard deviation, minimum and maximum. Categorical variables were expressed as number of cases and the percentage value. Whether continuous variables were appropriate to normal distribution were analyzed using Kolmogorov–Smirnov and Shapiro–Wilk tests. In the comparison of groups for COPD stages (moderate and severe) or patients who desaturated during exercise and who did not, the Student’s t test and Mann–Whitney U test were used according to the situation of variables (normally distributed or not). The difference between baseline and final values of Borg, mMRC scores and SpO2 during the 6MWT were evaluated using t test and Wilcoxon test in paired series. Comparison of categorical variables was performed using χ 2 and Fisher’s exact tests. Spearman’s correlation test was used to analyse the relationship between the variables. Statistical significance was set as p < 0.05.
Results
In total, 55 patients (49 males and 6 females, mean age: 65.8 ± 8.4 years) were included in this study. Twenty-seven patients (49.1%) had moderate COPD, and 28 patients (50.9%) had severe COPD. Demographic characteristics of the groups are summarized in Table 1. Mean FEV1 of the whole group was 1352 ± 348 ml (FEV1% predicted of normal: 51.2% ± 11.8%). The mMRC score of moderate COPD group was 0.37 and for the severe COPD group it was 0.9. The difference between the groups was significant (p = 0.01). PaCO2 levels were significantly higher in the patients with severe COPD than patients with moderate COPD (p = 0.001). There were no differences between the groups for the DLCO, 6MWD, partial arterial oxygen pressure (PaO2) and arterial oxygen saturation (SaO2) values. Data for spirometry, DLCO, ABG analysis, 6MWT and the nocturnal oximetry of the groups are given in Table 1.
Demographic characteristics and laboratory findings of the groups.

COPD: chronic obstructive pulmonary disease; BMI: body mass index; mMRC: modified Medical Research Council; FEV1: forced expiratory volume in one second; PaO2: partial arterial oxygen; PaCO2: partial arterial carbon dioxide; SaO2: arterial oxygen saturation; SpO2: peripheral oxygen saturation; DLCO: carbon monoxide diffusion test; 6MWD: six-minute walk distance; 6MWT: six-minute walk test; SD: standard deviation.
a% of predicted normal.
The 6MWT was stopped when the saturation dropped below 90%, if subjects were exhausted or heavily dyspnoeic. Two patients desaturated to 80%, and they were severely symptomatic, thus their tests were terminated early. In all, 15 (27%) patients desaturated during the 6MWT. Of the whole group, the mean DLCO, FEV1, resting PaO2 and SaO2 of the patients who desaturated during the 6MWT were lower than the patients who did not desaturate (p < 0.001, p = 0.01, p = 0.003, p = 0.006, respectively). The mMRC scale and final BORG scale scores during 6MWT were higher in patients who desaturated (p = 0.01 and p = 0.02). PaCO2 levels and 6MWD of the patients who desaturated were similar to those who did not desaturate. Also nocturnal mean oxygen saturation and the lowest nocturnal oxygen saturation were significantly lower in patients who desaturated during 6MWT (p = 0.001 and p = 0.01, respectively). The comparison of the patients who desaturated during the 6MWT and those who did not are given in Table 2.
Comparison of the patients who desaturated during 6MWT and the others who did not.

6MWT: six-minute walk test; FEV1: forced expiratory volume in one second; PaO2: partial arterial oxygen; PaCO2: partial arterial carbon dioxide; SaO2: arterial oxygen saturation; SpO2: peripheral oxygen saturation; 6MWD: six-minute walk distance; DLCO: carbon monoxide diffusion test; NOD: nocturnal oxygen desaturation; SD: standard deviation.
a% of predicted normal.
When we analysed the groups separately, 3 (11%) of the patients who desaturated during the 6MWT had moderate COPD and 12 (42.9%) were in the severe COPD group. The number of desaturators was significantly higher in the severe COPD group (p = 0.003). There was a positive correlation between DLCO and final SpO2 during the 6MWT (r s = 0.586, p = 0.001) for the patients with severe COPD.
NOD was observed in five (n = 5/55, 9.1%) patients and each of them was in the severe COPD group (n = 5/28, 17.9%). However, there were no patients who had NOD in the moderate COPD group. The difference between the groups was statistically significant (p = 0.02). The mean saturation and the lowest saturation during sleep were lower and time spent with SpO2 < 90% was higher in the patients with severe COPD when compared with the patients with moderate COPD (p = 0.04, p = 0.01 and p = 0.04, respectively). There was no relationship between NOD, 6MWD and DLCO for the whole study group. However, NOD was more frequent in patients who had lower daytime PaO2 and SaO2 and higher PaCO2 and mMRC scale scores (p = 0.01, p = 0.002, p = 0.001 and p = 0.01, respectively). The final SpO2 during the 6MWT and mean nocturnal SpO2 showed a moderate correlation with NOD in the patients with severe COPD (r s = 0.450, p = 0.01). The comparison of the patients who had NOD and those who did not is given in Table 3.
Comparison of the patients who had NOD and the others who did not.
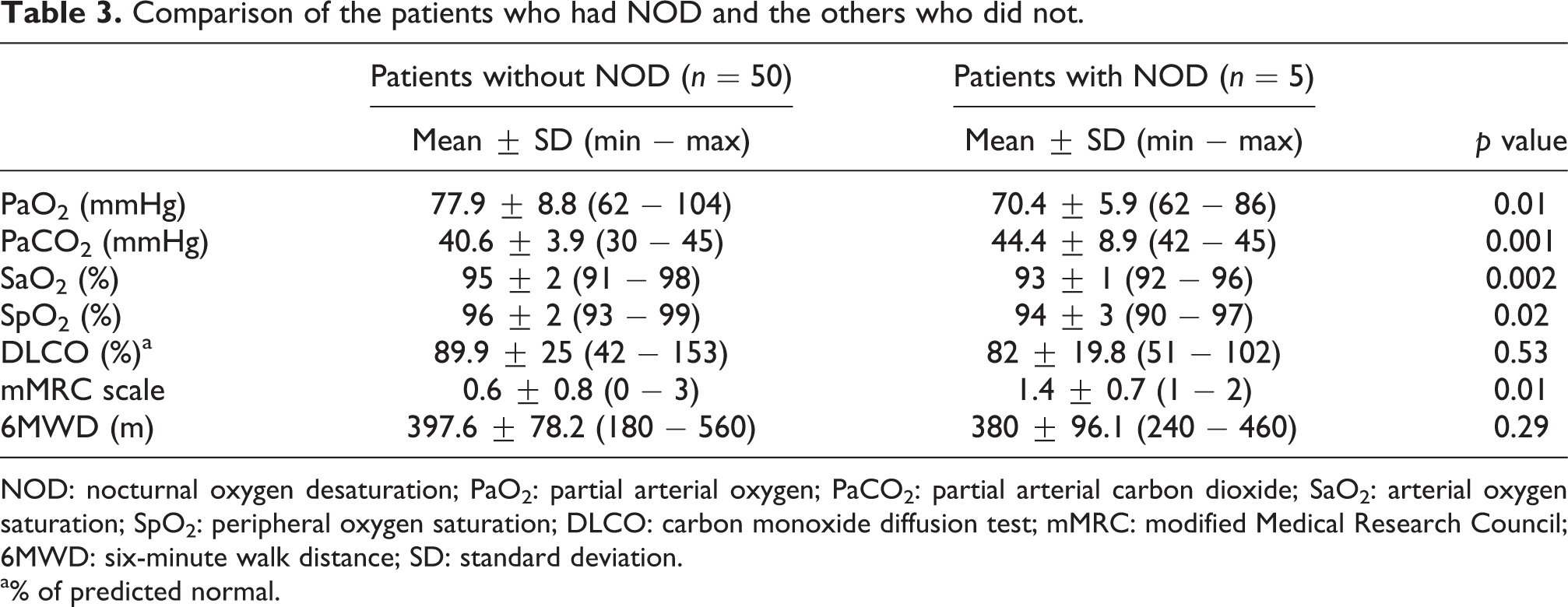
NOD: nocturnal oxygen desaturation; PaO2: partial arterial oxygen; PaCO2: partial arterial carbon dioxide; SaO2: arterial oxygen saturation; SpO2: peripheral oxygen saturation; DLCO: carbon monoxide diffusion test; mMRC: modified Medical Research Council; 6MWD: six-minute walk distance; SD: standard deviation.
a% of predicted normal.
Three of 15 patients (20%) who desaturated during the 6MWT also had NOD. All of these patients had severe COPD, so NOD and coexisting exercise desaturation were present in 10.7% (n = 3/28) of the patients with severe COPD. Three (11%) patients with moderate COPD desaturated during exercise, but none of them had NOD.
Discussion
LTOT indications and the positive effects of LTOT on prognosis have been clearly identified for patients with severe hypoxaemia at rest. However, the debate continues regarding the effectiveness of oxygen therapy in patients who need oxygen therapy only during exercise or sleep. 9,10,18 –21 On the other hand, it is not clear whether patients who desaturate during exercise have coexisting NOD or not because there are different mechanisms of desaturation in exercise and sleep. Patients who desaturated during exercise may not desaturate during sleep. In the literature, it is not clear whether NOT improves survival of patients with COPD who have NOD but are not hypoxaemic with daytime rest. There are several studies in this area. 22 –25 However, there is evidence that some patients with mild hypoxaemia at rest in normal room air conditions can develop clinically significant NOD, which may lead to pulmonary hypertension. 24 In the study of Fletcher et al., survival was significantly better in COPD patients without NOD, and the authors advocated NOT for COPD patients with mild–moderate hypoxaemia in daytime rest. 24 Contrary to this, in a recent study by Chaouat et al., it was suggested that NOD did not lead to permanent pulmonary hypertension in patients with COPD who have mild hypoxaemia in the daytime. 25 There are also studies reporting no significant increase in mortality rate in patients with mild hypoxaemia. 22,23,25,26 According to these data, we think that patients in the advanced stages of COPD with mild–moderate daytime hypoxaemia may show different results with NOT. Current guidelines do not recommend NOT for isolated NOD. The effect of NOT is controversial, and new studies are needed in this area to assess the significance of isolated NOD in patients with COPD.
The exact prevalence of NOD in COPD is not known. There are studies with different results depending on the sample studied. Fletcher et al. found that 27% of patients with daytime PaO2 equal or more than 60 mmHg experienced rapid eye movement period-desaturation. 24 Subsequently, two more studies including small numbers of patients with COPD reported the prevalence of NOD to be approximately 50%. However, some patients in these studies had some degree of daytime hypoxaemia. 27,28 Scott et al. reported that 19.4% of their study population had NOD. 29
There are some difficulties in performing nocturnal oximetry in some countries due to the need for hospitalization, staff and the overload of sleep laboratories. There are also portable and at-home night pulse oximetry options instead of hospital settings. However, this has some limitations like possible damage or loss of the device by the patient or the pulse oximeter could fall off the finger without the patient noticing during sleep. This would produce a short recording time due to the early removal of the device. The 6MWT, on the other hand, can be conducted easily without hospitalization and is inexpensive. In our study, oxygen desaturation during exercise was defined as a fall in SpO2 of ≥4% to a value <90% which was measured using a pulse oximeter at baseline and end of 6MWT. 17 There are also different definitions for desaturation during exercise but we used the criteria of British Thoracic Society. 17 SpO2 of 90% corresponds to PaO2 = 60 mmHg, and this is the limit for moderate hypoxaemia. This is the rationale for the choice of desaturation criteria during exercise in our study. If we can detect a relationship between exercise desaturation and NOD, we can suggest that there is no need for nocturnal oximetry in hospital. Because of this we aimed to investigate the relationship between desaturation during exercise and NOD in patients with COPD. There are very few studies evaluating the relationship between desaturation during exercise and NOD. 29 –32 One of these studies performed by Mulloy et al. included 25 COPD patients with PaO2 < 10 kPa (mean = 8.6 kPa) and reported that desaturation during the 6MWT does not provide extra information to daytime ABG for identifying patients with NOD. 30 Additionally, Fletcher et al. studied patients with COPD who have daytime PaO2 equal to or greater than 60 mmHg. This study showed that desaturation during exercise could not predict NOD. 31 On the contrary, a more recent study of Scott et al. included a larger group of patients with COPD (n = 303). This study consisted of two subgroups. One group was the exploratory study group (n = 103) and the other was the validation group (n = 200). They diagnosed NOD according to an overnight measurement of SpO2 via a pulse oxymeter with a finger probe, similar to our study. The definition for exercise desaturation in this study was desaturation to or below 88%. This definition was different from our study. Scott et al. concluded that oxygen saturation change during a 6MWT was useful to identify COPD patients who might desaturate during sleep. 29 Garcia Talavera et al. included 83 patients with moderate to severe COPD who had PaO2 > 60 mmHg in their study and found that patients with COPD who desaturated in the first minute of the 6MWT were those most likely to desaturate during sleep. 32 In our study, NOD tended to be more common in patients who desaturated during exercise, but it did not reach statistical significance. Additionally, we could not demonstrate a correspondence between exercise desaturation and NOD. In our study, all of the patients with NOD were in the severe COPD group. According to our findings, the 6MWT may be useful to predict NOD but only for patients with severe COPD. However, our result is not strong enough to suggest that desaturation during 6MWT predicts NOD. More studies with larger sample groups are needed to make a conclusive decision on this finding.
Although some studies report that pulmonary function was not useful for predicting NOD, there are some studies saying the opposite. 29,33 The studies of Hadeli et al. and Owens et al. identified lower DLCO values as the strongest indicator of desaturation during exercise in patients with COPD. 34,35 In both studies, it was recommended to perform exercise testing for evaluating desaturation especially for moderate to severe COPD patients with DLCO < 70%. Similarly, in our study, we demonstrated that DLCO levels were significantly lower in patients who desaturated during the 6MWT. Our findings showed that patients who desaturated during the 6MWT also had lower FEV1, PaO2 values and higher mMRC scale scores. The study of Boer et al. showed good correlation between the mMRC scale score and walk-test performance, but they concluded that because dyspnoea scales were subjective, they would not be a substitute for objective methods of measuring functional capacity. 36 In our study, mMRC scale scores were very low in the severe COPD group, but it was significantly higher than the moderate COPD group. This could also be associated with it being a subjective scale. Despite detection of mMRC scale scores significantly higher in patients with severe COPD, our study did not show such difference in the 6MWD relative to the stages of COPD.
In our study, although we excluded hypercapnic patients in order to exclude sleep disorders, NOD correlated with high PaCO2 and low PaO2 values. The study of Chaouat et al. included 94 COPD patients with PaO2 in the range of 56–69 mmHg. In contrast to our study, the authors used polysomnography to exclude sleep apnoea syndrome. The results of Chaouat et al. were similar to our study in that NOD correlated with high PaCO2. However, they did not show such a relationship for PaO2. 33 Scott et al. showed a correlation between low PaO2 and low SaO2 with NOD, similar to our study. 29
Cote et al. investigated the relationship between mortality rate and the 6MWD in patients with COPD. 37 It was shown that mortality increased significantly when the 6MWD was under 350 metres. This study highlighted the prognostic significance of the walking distance. 37 In our study, there was no difference in 6MWDs between the patients with moderate and severe COPD. On the other hand, the mean 6MWD was similar for the patients who desaturated during exercise or sleep and those who did not.
There are some limitations of our study. We included all patients with COPD in our outpatient clinic who were suitable according to our inclusion and exclusion criteria. Because inclusion of the patients continued for a limited time period, we did not do a power calculation. This is a limitation of our study. Secondly, admission of patients with very severe COPD might be less due to functional disability. Therefore, these patients might have been missed in our study. Consequently, the rate of patients in our study who desaturated may have appeared lower than the true rate. Additionally, the number of participants in our study was limited. More studies with larger participant numbers should be performed to investigate the predictors of NOD in patients with COPD. In order to rule out other causes of NOD, patients with sleep apnoea syndrome were excluded from the study. In our study, the diagnosis of sleep apnoea syndrome was considered according to the cardinal symptoms of sleep apnoea, Epworth Sleepiness Scale score, hypercapnea and high BMI instead of polysomnography. Polysomnography is the gold standard method for determining sleep apnoea syndrome. Although there are ‘at-home sleep studies’ to diagnose sleep apnoea syndrome, the limitation of this method is confidence of the true sleeping status of the patient. This is because these devices have no electroencephalogram recording. Using nocturnal oximetry, we could record only oxygen saturation and pulse rate through the night. It was not possible to understand whether the patients were asleep or not. Therefore, the level of NOD in our patients may have been more than we have reported. Three patients in the moderate COPD group who desaturated during exercise did not desaturate during sleep. We may conclude that having moderate disease might be the reason for not having NOD. We cannot be certain whether the patients were asleep or not during the nocturnal oximetry. In addition, using the finger probe with cold peripheries or using it whilst walking (motion artefact), would cause inaccuracies in readings whilst performing the 6MWT or sleep study. Therefore, ABG might be preferred after the 6MWT in order to evaluate the final SpO2. We chose not to perform ABGs because it is an invasive test.
Conclusion
Early detection of nocturnal hypoxaemia in severe COPD and giving oxygen therapy may be very important to improve mortality and morbidity of this disease. However, the current data and guidelines do not recommend NOT for isolated NOD. The clinical importance of NOD and the need for NOT alone should be studied in larger populations. Although the number of cases and statistical relationships in this study is not enough to be conclusive, NOD was more common in desaturators during 6MWT particularly in patients with severe COPD.
Footnotes
Acknowledgements
The authors thank Dr Turhan Ece, Dr Zeki Kılıcaslan, Dr Aysen Dokme, Dr Fatma Comce and Dr Nilay Akbay for their help in data collection. Our thanks also to Mr David Chapman for language editing.
Conflict of interest
The authors declared no conflicts of interest.
Funding
Our study has been afforded by Faculty of Medicine, Istanbul University, Turkey.