
Abstract
Numerous patients with chronic obstructive pulmonary disease (COPD) and asthma do not use inhaler devices properly, which can contribute to poor disease control. The objective of this study is to assess the technical and safety use of dry powder inhalers (DPIs) versus pressurized metered-dose inhalers (MDIs) in adult patients with COPD or asthma in Lebanon. A concurrent, prospective comparative observational study was conducted at one hospital and 15 community pharmacies in Lebanon. Over a period of 18 months, 246 questionnaires were filled. Patients included were adults with COPD or asthma. Answers were entered into the Statistical Package for Social Sciences software and excel sheet. T-test and correlation were used to analyze the results; 67.8% and 38.4% of those using DPIs and MDIs, respectively, performed the exact technical steps adequately (p = 0.003, relative risk: 2.134, 95% confidence interval: 0.910–4.842). When compared to MDI, a higher percentage of DPI users found their devices easy to use. Moreover, 81.4% of the MDI users found difficulty in coordinating between pressing the canister and inhaling. Rates of exacerbations were significantly higher in MDIs vs. DPI users (59.4% vs. 21.7%). Overall, 44.31% of patients did not receive education from their healthcare professionals about the devices. A significant number of COPD/asthma adult patients do not use their devices properly. Even though DPIs were significantly easier to use, proper education on the technical use of all types of inhalers is needed.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are chronic respiratory diseases (CRDs) of the airways and the lungs. 1 According to the American Thoracic Society, CRDs are responsible for around 7% of deaths worldwide; they are a major burden on public health services and are a cause of diminished quality of life and loss of productivity. 2 In Lebanon, and despite limited data, one study was able to determine the prevalence of COPD as 9.7%. 3 In addition, and as estimated by the World Health Organization, by 2030, COPD will be the third leading cause of death around the world. 4 Since respiratory diseases affect a considerable percentage of the population worldwide and because of the increasing risk of morbidity and mortality, more efforts should be made in order to increase prevention and optimize treatment of such diseases. One way is to improve the use of inhaler devices and appropriately train and educate patients. 5,6
Pressurized metered dose inhalers (MDIs) and dry powder inhalers (DPIs) are the most commonly used inhaler devices. MDIs, developed in the mid-1950s, 7 deliver a fixed drug dose from a pressurized canister requiring coordination between inhalation and actuation. Around two decades later, 8 DPIs were introduced to the market as a more convenient alternative to MDIs since they deliver the drug in a powder form and do not require coordination. Although inhalers are highly effective in reducing the burden and risk of asthma and COPD, many patients do not use them properly. Multiple studies have shown that a significant percentage (up to 94%) of patients fail to complete at least one step correctly. 9 –14 This poor adherence contributes to uncontrolled symptoms, 15,16 low drug deposition in the lungs, 14,17 impaired quality of life, flare-ups, urgent doctor visits, and loss of life. 18 There are multiple factors related to incorrect inhalation technique, the most reported include old age, 12,13,16,19 –23 low education level, 11,13,19,22,23 lack of prior instructions, 12,13,16,19,20,22,23 and the use of multiple devices. 12,21
As for device type, data is inconsistent in favoring one type over the other. Multiple trials have shown more errors with the use of MDIs than with DPIs. 9,13,23 –25 A large French observational study of 3811 patients showed that errors were higher in patients using pressurized MDIs (76%) versus DPIs (49–55%). Critical errors compromising treatment efficacy were highest for Turbuhaler (32%) followed by MDIs (28%) and finally by Aerolizer, Autohaler, or Diskus (11–12%). 24 Furthermore, few studies favored specific DPIs over the others such as Diskhaler, 10,21 Handihaler, 11 or Diskus. 23,25 On the other hand, a recent retrospective multicenter study reviewed medical registries of COPD patients on fixed-dose combinations of inhaled corticosteroids and long-acting β 2 agonists. After adjustment for confounding factors, results showed that patients using DPIs (vs. MDIs) were less likely to adhere to treatment. 26 Another large multicenter study found no significant difference in inadequate inhalation technique between DPIs (17% for Aerolizer, 23% for Turbuhaler, and 24% for Diskus) and MDIs without a spacer (24%). 27 The “Device Selection and Outcomes of aerosol therapy: evidence-based guidelines,” published by CHEST (2005), concluded that devices used for the delivery of bronchodilators and inhaled corticosteroids do not differ in efficacy. However, the randomized controlled trials included are of limited quality (design and duration) where patients are carefully selected and well trained thus not reflecting reality and effectiveness. 28
Accordingly, it is necessary for healthcare professionals to understand the administration difficulties faced by patients in order to prescribe the preferred and most appropriate device for each individual and emphasize on the important steps for administration. Healthcare professionals identify poor adherence with inhalers as a major barrier to the delivery of effective asthma and COPD care, yet practical adherence interventions are lacking.
Because of the conflicting data worldwide and the limited data in Lebanon, this study was conducted in order to assess the technical and safety use of DPI (all types such as Diskhaler, Accuhaler, Turbuhaler, and Handihaler) vs. pressurized MDI devices in adult patients with COPD or asthma in Lebanon.
Methods
Setting and design
A concurrent, prospective comparative observational study was conducted at one teaching hospital and 15 community pharmacies in Lebanon in Beirut and Byblos area over a period of 18 months. Patients, with COPD or asthma using MDIs and/or DPI devices, visiting the community pharmacies to purchase such products or being hospitalized due to pulmonary diseases and discharged on such devices were asked if they were willing to participate in the study. Two structured questionnaires (one for MDIs and one for DPIs) were prepared by the investigators in order to conduct the survey. This study was approved by the Lebanese American University (LAU) Institutional Review Board and a waiver of consent was obtained from the patients before filling out the questionnaire.
Inclusion/exclusion criteria
Adult patients (at the age of 18 years or older), from both genders, suffering from COPD or asthma and using medications delivered through MDIs and/or DPIs were included. Patients receiving pulmonary medications through nebulizers or soft mist inhalers only were excluded.
Sources of data
The investigators, with the help of LAU pharmacy students, interviewed pulmonary hospitalized patients and/or patients entering the community pharmacies from 9:00 am till 4:00 pm. The investigators included community and clinical pharmacists (all of which are preceptors to the LAU students and some are professors as well). All of them were trained prior to the initiation of the study. Pharmacy students helping the investigators were completing their fifth and sixth year of pharmacy. They were well trained as well prior to initiation of the study and were supervised by their preceptors. Students were paired in two at each pharmacy/hospital. Both students along with the investigators assessed patients and filled the questionnaires. The tool for assessment consisted of two well-structured questionnaires, where the patients, with the assistance of the investigators, filled the questions with the appropriate answers.
One questionnaire targeted patients using DPIs users, whereas the second targeted those using MDIs. Each questionnaire is divided into three sections. The first section consists of patient’s demographics, the second section includes information about the administration techniques and the different steps required for using DPIs or MDIs, and the last section marks data about ease of use, safety, and patients’ preference (Tables 1 and 2). At the end of data collection, a total of 246 questionnaires were filled; 123 for DPIs and 123 for MDIs. The questions were converted to endpoints in order to meet the objective of the study.
DPI questionnaire.
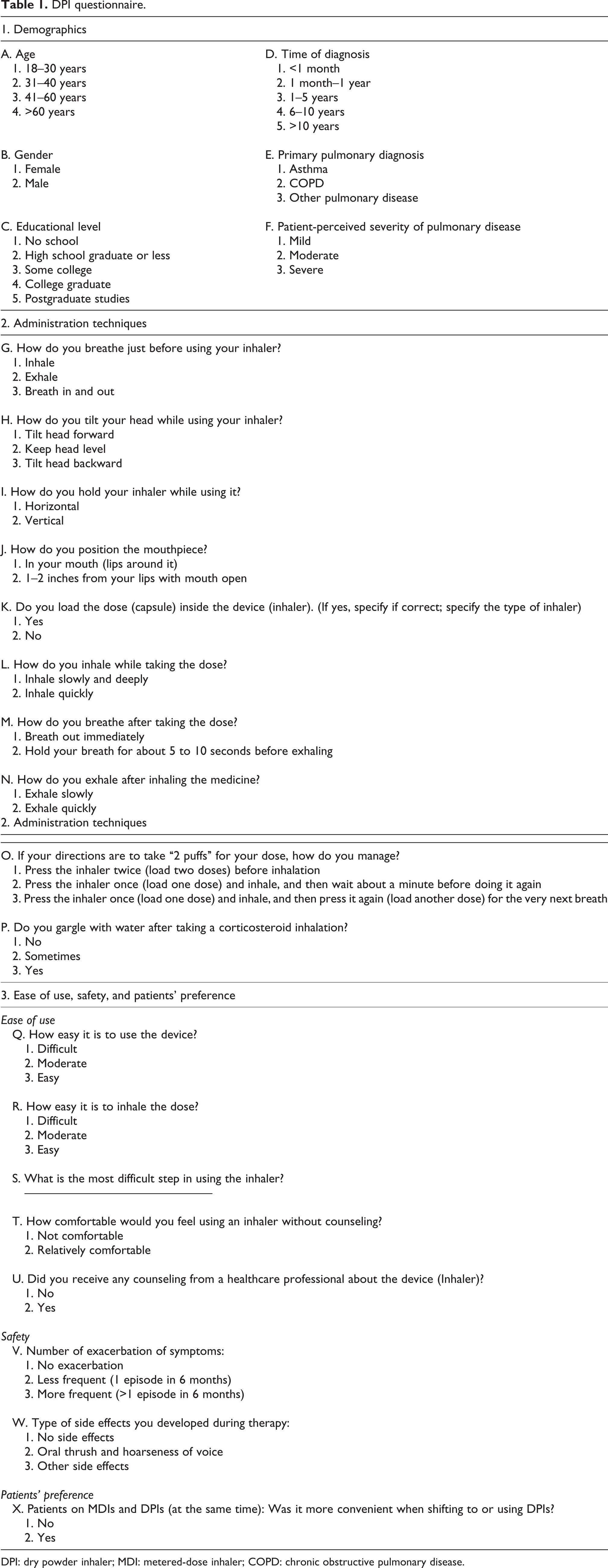
DPI: dry powder inhaler; MDI: metered-dose inhaler; COPD: chronic obstructive pulmonary disease.
MDI questionnaire.

DPIs: dry powder inhalers; MDIs: metered-dose inhalers; COPD: chronic obstructive pulmonary disease.
The primary endpoint was the correct application of the administration techniques. The responses for both devices were converted to either “proper” or “improper.” The secondary endpoints were the ease and safety of use as well as patients’ preference. Each one was analyzed based on the answers to the corresponding questions.
A correlation was conducted to analyze the relationship between ease of use and age; the ease of use and the time of diagnosis; the ease of dose inhalation and exacerbation of symptoms; and gargling after taking a corticosteroid inhalation and side effects. Three categories were developed for the ease of use: difficult, moderate, and easy; two categories for age: all ages (18– 60 years) and age >60 years; two categories for time of diagnosis: <1 year, and >1 year; three categories for the ease of dose inhalation: difficult, moderate, and easy; three categories for exacerbation of symptoms: no exacerbation, less frequent (1 episode in 6 months), more frequent (>1 episode in 6 months); three categories for gargling: no gargling, sometimes, after each dose; and three categories for side effects: no side effects, oral thrush and hoarseness of voice, and other side effects.
Statistical analysis
Data was processed and analyzed through the application of two software: The Statistical Package for Social Sciences (SPSS, version 19, Chicago, IL, USA) and Microsoft Excel. Responses were tabulated and cross-tabulated. Percentages, p-values, relative risk (RR), and 95% confidence interval (CI) were calculated. T-test and binary correlation were applied in order to analyze the results.
Results
A total of 246 patients were surveyed, out of which 123 were using DPIs and 123 were using MDIs; 37 patients (15%) were on both DPIs and MDIs at the same time. Demographic information is shown in Table 3.
Baseline demographic percentages.

DPI: dry powder inhaler; MDI: metered-dose inhaler.
The primary endpoint involved the correct application of the administration techniques of all types of inhalers. Only 19.5 and 26.3% of MDI users, respectively, prime and shake the inhaler before taking the dose. High percentages of both groups position the head and the mouth piece properly while using the inhalers and exhale appropriately after inhaling the dose. However, no significant difference is revealed between the two groups. A higher percentage of DPI users (67.8%) performed the exact technical steps (administration techniques) adequately and properly, as compared to MDI users (38.4%) (p = 0.003, RR: 2.134, 95% CI: 0.910–4.842). The percentages of appropriateness for all administration techniques with p-values are shown in Table 4; a t-test was conducted to test the significance level of difference on administration techniques between DPIs and MDIs: DPI users, as compared to MDI users, had a significant higher percentage of appropriateness on the way of holding the inhaler (100% vs. 73.9%) and the type of inhalation while taking the dose (83.7% vs. 61.2%).
Administration techniques.
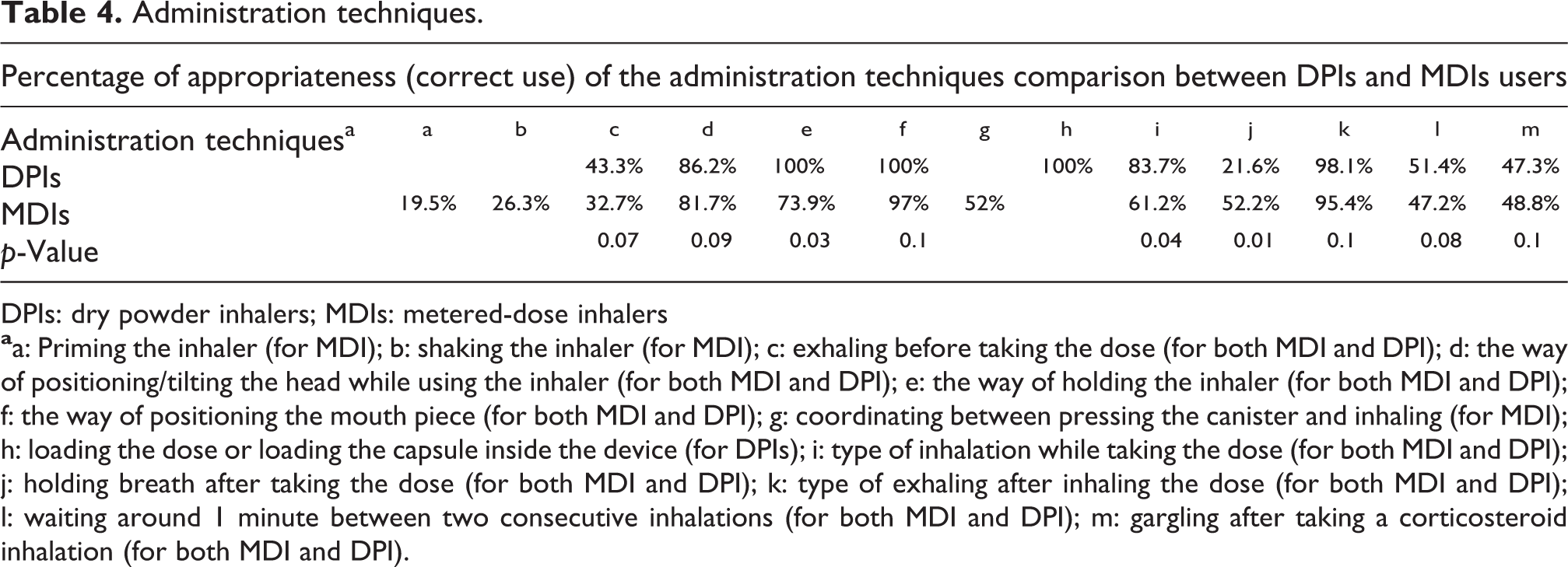
DPIs: dry powder inhalers; MDIs: metered-dose inhalers
The common unapplied (not applied correctly) steps, after being calculated from Table 4, among DPI users vs. MDI users were exhaling before taking the dose (56.7% vs. 67.3% of patients do not apply it correctly; p = 0.07), holding breath for few seconds after taking the dose (78.4% vs. 47.8% of patients do not apply it correctly; p = 0.01), waiting around 1 min between two consecutive doses (48.6% vs. 52.8% of patients do not apply it correctly; p = 0.08), and gargling after taking a corticosteroid inhalation (52.7% vs. 51.2% of patients do not apply it correctly; p = 0.1).
A secondary endpoint was the ease of use of the inhalers. A higher percentage of DPI users (87.3%) found the devices easy to use compared to 56.7% of the MDI users group who said their devices are easy to use (p = 0.001, RR: 2.031, 95% CI: 1.187–3.453). The majority of DPI users (94.8%) found it easy to inhale the dose vs. 53.6% of MDI users (p = 0.001, RR: 2.321, 95% CI: 1.075–3.835). Most of MDI users (81.4%) found difficulty in coordinating between pressing the canister and inhaling, whereas 15.8 and 23.7% of DPI users, respectively, considered loading the dose or loading the capsule inside the device (for DPIs) and holding the breath after taking the dose as the most difficult steps. Out of 246 patients of both groups, 109 patients (44.31%) mentioned that they did not receive the required education or counseling from the healthcare professionals (pharmacists or physicians) about the devices. When asked how comfortable would you feel using an inhaler without counseling, 48.47% of DPI users and 41.51% of MDI users, respectively, answered as relatively comfortable.
Ease of use was allied with the age group, mainly for patients who are above 60 years of age; and with the time of diagnosis. There was a significant negative correlation between ease of use and age for all patients (Table 5; section I). For patients using DPIs and diagnosed with COPD or asthma for more than 1 year, 73.27% found it easy to use vs. 46.34% in the MDI users. For all patients (Table 5; section II), there was a significant positive correlation between ease of use and time of diagnosis.
Correlations.

DPIs: dry powder inhalers; MDIs: metered-dose inhalers.
Safety of use was another secondary endpoint. A statistically significant difference was shown between the two groups in the incidence of exacerbation of symptoms. A much higher percentage (59.4%) of MDI users showed exacerbation of symptoms during therapy compared to only 21.7% of DPI users (p = 0.002, RR: 2.765, 95% CI: 1.184–6.846). As for the side effects developed during therapy, a statistically significant difference was also notified between the two groups (p = 0.01, RR: 2.32, 95% CI: 0.657–1.875) where 49.7 and 16.8% of DPI and MDI users, respectively, developed oral thrush. Ease-of-dose inhalation was stratified by the exacerbation of symptoms. However, there was no significant relationship between them for all patients, DPI users, and MDI users (Table 5; section III). When studying the relationship between gargling after taking a corticosteroid inhalation and side effects, it was noticed that there was a significant negative correlation between them (Table 5; Section IV).
Touching another secondary endpoint that measured patients’ preferences, 78.7% of patients using DPIs and MDIs together found it more convenient shifting to or using DPIs instead of MDIs; and 81.9% of the MDI users would like to shift to a DPI if it has the same cost.
Discussion
The study shows significantly higher adequate and proper administration technique with DPI users (67.8%) vs. MDI users (38.4%). These results are consistent with multiple studies in the literature. 9,13,23 –25 Regarding specific steps, DPI users were significantly better at holding the inhaler appropriately (100% vs. 73.9%) and inhaling correctly while taking the dose (83.7% vs. 61.2%). These findings can also be explained by the less complex administration of DPIs (no coordination needed). Common errors for both DPIs and MDIs were exhaling before the dose, holding breath after the dose (fewer errors with MDIs), waiting between two consecutive doses and finally gargling after a corticosteroid dose. Previous data have shown that common error for both types of inhalers was to exhale before taking the dose. 23,29 Lavorini et al. summarized data from 18 studies performed in patients with asthma and COPD exhibiting specific errors in DPIs technique. Exhaling before taking the dose is by far the most common error observed (12–77%) followed by failure in holding the breath after the dose (0–73%). 14 In this study and for MDIs specifically, patients ranked low in performing the following steps: priming the inhaler (19.5%), shaking the inhaler (26.3%), and coordinating between pressing the canister and inhaling (52%). About 81.4% of MDI users identify coordinating between pressing the canister and inhaling as the most difficult step. On the other hand, 15.8 and 23.7% DPI users, respectively, considered loading the dose and holding the breath after taking the dose as the most difficult steps. A higher percentage of DPIs users found their device easy to use and the inhalation easy to take when compared to MDIs.
Melani et al. investigated the misuse of inhalers in 1644 patients with COPD and asthma. Most common errors seen with MDIs use were failure to exhale before the dose, coordinate between pressing on the canister and inhaling, and hold breath followed by failure to shake the inhaler. 19 This study also found, independent of the inhaler type, a strong association between inhaler misuse and older age and lack of instructions. 19
Our data shows a statistically significant negative correlation between ease of use and age, a positive correlation between ease of use and time of diagnosis, and finally a negative correlation between gargling after taking corticosteroid inhalation and side effects. This confirms once again that the older age is associated with the misuse of inhaler thus special attention to this age group is needed during counseling; moreover, patients will increase their risks of developing some side effects such as oral thrush when they don’t gargle after inhaling a corticosteroid dose. As mentioned previously, lack of prior instructions is one of the major risk factors for inadequate inhalation technique. 12,13,16,19,20,22,23 Our study revealed that a significant percentage (44.31%) of patients did not receive the required education or counseling from their healthcare provider. This provides a major area for improvement and highlights once again the importance of appropriate education. Overall patients preferred DPIs. When asked, most patients on both types of inhalers preferred switching all of their devices to DPIs. After explaining the concept of DPIs (devices containing powdered medications where coordination between pressing on the canister and inhalation is not required) to patients on MDIs, most patients preferred shifting to DPIs if they were at the same cost.
There are multiple ways to improve inhalation technique. Re-education seems to be one of the most important ones. A series of studies were conducted between 1982 and 2000 to assess pressurized MDI use after reading inhaler package inset and/or receiving instructions. 30 –32 The percentage of patients able to use the inhaler appropriately declined throughout the years suggesting the need for re-education in order to maintain and ensure the adequate use of inhalers. In other words, previous ability to correctly use a pressurized MDI is not indicative of correct use during subsequent testing thus continuous re-evaluation is a must. 30 Another way to enhance and reinforce correct inhalation technique is the use of multimedia methods. One study showed that the use of multimedia improved patient’s inhalation technique when compared to the use of the patient information leaflet. 33 According to a recent study, multimedia counseling was as effective and time efficient as conventional counseling in MDIs education. 34 In addition, van der Palen et al. showed that the use of video instructions cause an improvement in inhaler techniques when compared to the control group and to those receiving personal instructions. The combination of multimedia and personal instructions is suggested as well. 35 Finally, the use spacer devices or holding chambers with pressurized MDIs facilitate the coordination between actuation and inhalation and reduce the impaction of large particles in the oropharynx. 36
Healthcare professionals should tailor the device choice to patients’ needs, preferences, and ability. For example, MDIs are preferred in those with spontaneous breathing, appropriate coordination, and poor inspiratory flow. For those with poor coordination but adequate inspiratory flow, a DPI, an MDI with spacer, or a breath-actuated MDI are preferred. As for those with poor coordination and poor inspiratory flow, a pressurized MDI with a spacer is the most efficient option. 36 Future research should be targeted toward finding the optimal device for each specific patient population.
There are some limitations to our study. First, an equal weight was given to each of the essential steps although some are more critical than others. This might overestimate the prevalence of the incorrect use of inhaler devices. On the other hand, one error in a critical step might counteract the entire effect and consequently influence the outcome. Second, results were reported by more than one observer thus interobserver variability cannot be ignored. Finally, our study neither measured compliance nor its relationship with the adequate use of inhaler devices.
Conclusion
In conclusion, the study showed a significant percentage of adult patients with COPD/asthma that do not use MDIs/ DPIs appropriately in the Lebanese community. However, proper administration technique was significantly higher in patients using DPIs. Also, it showed a high percentage of patients not receiving the needed education about their devices. Accordingly, it is very important for healthcare professionals to appropriately train their patients in order to gain the maximal benefits expected from the devices and to prevent exacerbations and worsening of symptoms.
Duration of the study was 18 months. Data collection type is prospective patient interview—questionnaires. Data collection places are community pharmacies and one hospital in Lebanon.
Footnotes
Acknowledgement
The authors gratefully acknowledge the assistance of Hamzeh Ramadan, PhD, in applying the statistical tests and reviewing the statistical analysis; Aline Milane, PharmD, PhD, in participating in the development of the questionnaires; and the LAU pharmacy students in collecting data and filling the questionnaires.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.