
Abstract
Chronic obstructive pulmonary disease (COPD) is a complex disorder with extrapulmonary manifestations. Even though there is some knowledge regarding sex differences in the lung disease, little is known about extrapulmonary manifestations. Our aim was to analyze the specific profile of muscle dysfunction, structure, and biology in COPD women. Twenty-one women and 19 men with stable COPD as well as 15 controls were included. Nutritional status, physical activity, lung and muscle function, exercise capacity, and quality of life were assessed. In addition, blood, breath condensate, and quadriceps muscle samples were tested for inflammatory markers. Moreover, fiber phenotype, signs of damage–regeneration, and the expression of key genes linked to myogenesis and inflammation were assessed in the muscle. Inflammatory markers were increased in all body compartments but no correlation was found among them. Muscle dysfunction was present in both COPD groups but was more marked in women. The opposite occurred with the increase in the percentage of type II fibers that was lower in women despite a similar level of airway obstruction as in men. Female COPD also showed higher signs of muscle damage than COPD men who, in contrast, exhibited slightly higher signs of regeneration. We conclude that sex influences muscle phenotype and function in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a rising cause of morbidity and mortality worldwide, 1 and recent studies show a progressively higher prevalence of this condition in women. 2 –5 Interestingly, different reports have suggested that women may be more susceptible to cigarette smoke and more likely to develop early-onset COPD than men, 6 –9 having a greater lung function decline than their male counterparts. 10 In addition, several authors have shown sex differences in the expression of the disease, including symptoms, radiological features, number and severity of exacerbations, and mortality. In this regard, women complain more about dyspnea and seem to have worse health-related quality-of-life scores for the same predicted forced expiratory volume in 1 second (FEV1) than men. 11,12 In addition, women have a higher hyperresponsiveness than men 13 and computed tomographic exams reveal that they have less extensive emphysema, 12,14,15 smaller airway lumens, and disproportionately thicker airway walls. 12 Moreover, COPD women show a higher risk of being admitted to hospital 6 and their mortality rates are higher than those of men. 16,17 However, the effect of gender in systemic manifestations of COPD is still an unexplored area. Skeletal muscle dysfunction, defined as the loss of muscle strength and/or endurance, is probably the most studied systemic manifestation of COPD and is very prevalent. 18 Moreover, muscle dysfunction also has an important impact on exercise tolerance and quality of life of the patients, 19 being an independent mortality predictor. 20 The main factors involved in muscle dysfunction are the decrease in physical activity that leads to deconditioning, nutritional abnormalities, hormonal deficiencies, and a low grade of systemic inflammation. 21 These factors are associated with structural and biological changes within the limb muscles, which include a switch to a higher percentage of type II fibers, apoptosis, muscle damage, oxidative stress, local inflammation, among others. 22 –26 Nevertheless, the preceding studies have been made on male COPD patients or in a mixture of both genders, without paying attention to the presence of potential differences between men and women. Therefore, the specific characteristics of muscle dysfunction in the latter still remain unexplored. Our hypothesis is that most of the factors involved in the differential expression of lung disease in COPD men and women (i.e. hormone profiles, lifestyle patterns, etc.) will also determine a different expression of skeletal muscle involvement. Accordingly, the aim of the present study was to investigate the pattern of muscle dysfunction in women, with special focus on the potential etiological factors as well as on muscle structure and biology.
Methods
Subjects
All stable (at least 3 months from the last exacerbation) COPD women who came to the outpatient clinic at our center were asked to participate but those with relevant comorbidities (heart, neuromuscular, chronic metabolic, or orthopedic disorders) or those receiving oral steroids or other drugs known to modify muscle structure or function were excluded from the study. Finally, 21 Caucasian women with stable COPD 27 were consecutively recruited. Then, 19 Caucasian men with stable COPD, matched for age, body mass index (BMI), and severity were also included. Additionally, eight healthy women and seven healthy men, never smokers, matched for age and BMI with COPD patients, were recruited from the general population. Approval was obtained from the local institutional Ethics Committee on Human Investigation and informed written consent was obtained from all individuals.
Nutritional assessment
Anthropometric variables including BMI and fat-free mass (FFM) index (acquired by bioelectrical impedance; BODYSTAT 1500, Bodystat Ltd, Isle of Man, UK) as well as serum nutritional markers (cholesterol, albumin, total proteins, hemoglobin, and prothrombin time) were obtained in all subjects.
Respiratory function
Forced spirometry was performed (Datospir 92, SIBEL, Barcelona, Spain), and static lung volume and airway resistance (body plethysmography; Masterlab, Jaeger, Würzburg, Germany) as well as carbon monoxide transfer (diffusing capacity of the lungs for carbon monoxide (DLCO); Masterlab) were obtained in all subjects. Variables are expressed through both absolute and percentage of predicted values. Equations for a Mediterranean population were always used. 28 –30 Arterial blood gases were only obtained in COPD patients (gas analyzer; GEM Premier 3000 Instrumentation Laboratory, Bedford, Massachusetts, USA).
Muscle Function
Handgrip and quadriceps muscle strength were evaluated in all the subjects through dynamometry as described elsewhere. 28 –33
Physical endurance
Physical endurance was evaluated through the 6-minute walking test following the American Thoracic Society (ATS)/European Respiratory Society (ERS) recommendations. 34 Walking distance was expressed as both absolute and related to predicted values. 31
Physical activity
Physical activity was measured using accelerometers (SenseWear® Pro2 Armband SWA; BodyMedia, Pittsburgh, Pennsylvania, USA) for seven consecutive days as described elsewhere. 35 Data are expressed as steps per day and metabolic equivalents.
Quality of life
Quality of life was assessed by the COPD-specific version of the St George’s Respiratory Questionnaire (SGRQ-C) 36 using those published for the Spanish population as reference values. 37
Blood samples
Blood samples were obtained after fasting overnight and, following 30 minutes of blood withdrawal, centrifuged at 2000–3000 r/min for 10 minutes. Serum was separated and stored in cryotubes at −80°C. Routine blood tests (complete blood count, biochemistry including liver and kidney functions) as well as high-sensitivity C-reactive protein, calcidiol (25(OH)D), calcitriol, and parathyroid hormone (PTH) were analyzed in all subjects, and estrogen, progesterone, and follicle-stimulating hormone levels were analyzed only in women. In addition, A Bio-Plex human cytokine assay was run according to the recommended procedure (Bio-Plex Precision Pro Assays Human Cytokine 10-Plex ref. 171-A1001P; Bio-Rad Laboratories, Hercules, California, USA). Then, serum levels of tumor necrosis factor (TNF)–α; interferon (IFN)-γ; interleukin (IL)-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, and IL-13; follistatin; leptin; granulocyte colony-stimulating factor (G-CSF); hepatocyte growth factor; vascular endothelial growth factor (VEGF); platelet-derived growth factor; and platelet endothelial cell adhesion molecule were determined. All analyses were performed in duplicate.
Breath condensate
Patients were asked to breath for 10 minutes in a condensator under ventilatory control (EcoScreen/ECoVent, Jaeger, Germany) according to the recommendations from ATS/ERS task force. 38 The samples were immediately frozen and later analyzed. The proteins expression of the following cytokines, TNF-α, TNF-β, IFN-γ, IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, and VEGF, were quantified using specific ELISA kits (RayBiotech, Norcross, Georgia, USA) following previously published methodologies. 7 For all the sample specimens, equal amounts of total protein were always loaded in duplicate. Protocol was also followed according to the corresponding manufacturer’s instructions for each cytokine.
Muscle samples
Open muscle biopsies of the vastus lateralis were obtained from COPD patients and controls following the procedures previously published by our group. 39 All structural and biological muscle analyses were conducted blind in the same laboratory and by the same investigators.
Structural analyses
Briefly, on 3-μm muscle paraffin-embedded sections from both patients and controls, myosin heavy chain (MyHC)-I and -II isoforms were identified using specific antibodies as published elsewhere. 40 The percentages of fiber types and their cross-sectional areas were then calculated. In addition, to assessing the presence of histological signs of muscle damage and regeneration, the area fraction of normal and abnormal muscle was also evaluated following previously published methodologies. 41
Gene expression
The expression of key genes for inflammation (TNF-α and its receptors RI and RII; IL-1β; IL-6 and its receptor; IL-10; and insulin-like growth factor (IGF)-1 and its receptor), cell damage or stress (embryonic and perinatal MyHC isoforms were MyHC-emb and MyHC-peri, respectively) and myogenesis (paired box protein 7 (Pax7), myogenic factor 5 (MyF5), M-cadherin, and differentiation factor 1 (Myo-D) were evaluated by determining their transcriptomes (mRNA) in the muscle. Succinctly, total RNA was extracted from muscle samples using TRIzol reagent (Invitrogen, Life Technologies SA, Grand Island, New York, USA) according to the manufacturer’s protocol. First-strand cDNAs were produced from total RNA using oligo(dT)12–18 primers and SuperScript III reverse transcriptase (Life Technologies SA). Then, quantitative PCR reactions were performed using TaqMan low-density arrays (TLDAs; Applied Biosystems, Foster City, California, USA). The cDNA was mixed with 2× TaqMan Universal PCR master mix (assays-on-demand gene expression products; Applied Biosystems, Foster City, California, USA), loaded into a port of the TLDA card, and run on an ABI Prism 7900HT sequence detection system (SDS; Life Technologies SA). The TLDAs contained 24 different TaqMan gene expression assays (Applied Biosystems) including three housekeeping genes. From them, glyceraldehyde-3-phosphate dehydrogenase was the most stably expressed among all samples and, therefore, it was chosen as our endogenous control (final housekeeping gene). One sample was used as calibrator for data normalization. Data calculation was performed using the relative quantitation (RQ) manager package from the SDS software, version 2.2.2 (Applied Biosystems) and was based on the ΔΔCt method. 42 Finally, data for the expression of each gene were calculated as normalized to those shown by healthy women.
Protein levels
Due to limitations of the muscle sample size, only protein levels of selected cytokines (TNF-α and its receptors RI and RII; IFN-γ; transforming growth factor beta 1; IL-1β, IL-6, IL-10, and IL-12; and VEGF) were quantified using specific ELISA kits (RayBiotech) and following previously published methodologies. 41,43
Statistical analysis
Normal distribution of each variable was determined by the Kolmogorov–Smirnov test. Data are presented as mean ± SD or n (%). Comparisons of physiological and biological variables between both groups of COPD patients and between each of these groups with their corresponding gender controls were analyzed using analysis of the variance. Bivariate relations between physiological and biological variables were explored using the Pearson’s correlation coefficient and a multivariate analysis was also conducted. Data analysis was done using the SPSS Statistics® package (version 20.0) and GraphPadPrism® (version 6.0). In all cases, statistical significance was defined by a p ≤ 0.05.
Results
General characteristics of the study population
Table 1 shows the main general, nutritional, and functional characteristics of all different study groups. Briefly, the cumulated exposure to tobacco smoking was higher in male COPD patients than in women with the disease, and a relatively large percentage of all patients were still active smokers (33% women vs. 26% men, not significant). However, COPD patients of both sexes showed similar nutritional parameters to their respective healthy controls. Moreover, the percentage of patients with low body weight (BMI < 18.5 kg/m2) was similar for both COPD women and men (19% vs. 21%, respectively). Finally, the use of drugs was similar in both groups, including both bronchodilators and inhaled steroids.
Demographic, lung and muscle function, physical activity, and exercise data.a

BMI: body mass index; FFMI: fat-free mass index; FEV1: forced expiratory volume in 1 second; RV: residual volume; TLC: total lung capacity; DLCO: diffusing capacity of the lung for carbon monoxide; PaO2: partial pressure of oxygen in arterial blood; PaCO2: partial pressure of carbon dioxide in arterial blood; MET: metabolic equivalent; HG: handgrip; QMVC: quadriceps isometric maximum voluntary contraction; 6MWT: 6-minute walking test; SpO2: oxygen saturation (oxymeter) at baseline; end-SpO2: oxygen saturation at the end of the 6MWT; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD or as n (%).
bp ≤ 0.01: between COPD men and women.
cp ≤ 0.01: between healthy and COPD women or healthy and COPD men.
dp ≤ 0.001: between healthy and COPD women or healthy and COPD men.
ep ≤ 0.05 between healthy and COPD women or healthy and COPD men.
fThe difference between COPD men and women for HG (absolute values) is p < 0.001.
gp ≤ 0.05 between COPD men and women.
Regarding respiratory function, the group of women showed a mean FEV1 of 39 ± 15% of reference values (ref.) with marked air trapping, reduced carbon monoxide transfer, and slight hypoxemia without hypercapnia. The level of impairment was similar for COPD women and men, with a similar distribution of the severity levels. Muscle of the lower limbs in both COPD groups was weaker compared with their respective controls, although this reduction was greater in female patients, even after normalization by FFM. In contrast, the upper limb function was similar in the four study groups. The exercise capacity, in turn, was slightly reduced in COPD women, and again this reduction was slightly more marked than that observed in COPD men. Obviously, respiratory and limb symptoms at the maximum effort level were more pronounced in both COPD groups than in their respective healthy controls, but there was no difference between COPD women and men (data not shown). The amount of physical activity was similarly reduced in both groups of COPD patients, but women showed a direct relationship of this dimension with quadriceps strength normalized by FFM (r2 = 0.40, p = 0.01). A similar tendency was observed in COPD men. Finally, the SGRQ-C showed a moderate and similar deterioration in the quality of life in both groups of patients (total score 46 ± 24 vs. 47 ± 18 in women and men, respectively). However, women showed a tendency to have a higher perception of dyspnea than men (48 ± 29 vs. 34 ± 23, p = 0.06, respectively).
Systemic inflammation
Both COPD groups showed elevated levels of different inflammatory markers in their peripheral blood, with no differences between men and women (Table 2). Moreover, women with COPD showed a direct correlation between the levels of IL-6 and the severity of the airway obstruction (r2 = 0.17, p < 0.05), which was absent in COPD men.
Serum levels of different cytokines.a

CRP: C-reactive protein; HsCRP: height sensitivity C-reactive protein; TNF: tumor necrosis factor; IFN: interferon; VEGF: vascular endothelial growth factor; PDGF: platelet-derived growth factor; G-CSF: granulocyte colony-stimulating factor; IL: interleukin; HGF: hepatocyte growth factor; PECAM: platelet endothelial cell adhesion molecule; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD.
bp ≤ 0.01: between healthy and COPD women or healthy and COPD men.
cp ≤ 0.05: between healthy and COPD women or healthy and COPD men.
dp ≤ 0.001: between healthy and COPD women or healthy and COPD men.
Lung inflammation
COPD women showed higher levels of diverse inflammatory markers than their healthy controls in the exhaled condensate. Moreover, their IL-8 levels were even higher than those shown by COPD men, with a similar trend for IL-10 (Table 3).
Levels of different cytokines in breath condensate.a

TNF: tumor necrosis factor; IFN: interferon; IL: interleukin; VEGF: vascular endothelial growth factor; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD.
bp ≤ 0.05: between healthy and COPD women or healthy and COPD men.
cp ≤ 0.05: between COPD men and women.
Vitamin D, calcium metabolism, and estrogens
The level of 25-hydroxivitamin D (25(OH) vit D) was significantly lower in women with COPD than in their healthy controls. COPD males showed a similar trend, although less marked than women (Table 4). Furthermore, a decreased level of 25(OH) vit D was evident in the latter, even in the subgroup of patients with only moderate lung disease. By contrast, levels of calcium, phosphate, and PTH were similar among the four study groups. Interestingly, the levels of 25(OH) vit D were directly associated with muscle strength (r2 = 0.14, p = 0.05, for handgrip; and r2 = 0.27, p = 0.01, for quadriceps strength) and inversely with IL-6 levels (r2 = 0.16, p < 0.05) in women. Finally, estrogen levels were very low in both female COPD patients and control women (data not shown).
Serum levels of calcium metabolism parameters.a

25(OH) vit D: 25-hydroxivitamin D; PTH: parathyroid hormone; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD.
bp ≤ 0.05: between COPD men and women.
cp ≤ 0.05: between healthy and COPD women.
dp ≤ 0.01: between COPD men and women.
Structure and molecular events in the quadriceps muscle
Fiber phenotype: COPD patients of both genders showed a higher proportion of type II fibers than their respective healthy controls (Table 5). However, this increase was significantly lower in COPD women compared with COPD men, and the former also showed a direct relationship between the proportion of type II fibers and both the degree of airway obstruction and the BMI-airway Obstruction-Dyspnea-Exercise capacity (BODE) index as well as an inverse correlation with oxygen saturation at the end of the 6-minute walking test (Figure 1(a) and (b)). In addition, both COPD groups showed a tendency to have smaller fibers than their respective healthy controls, although this did not reach statistical significance. However, type II fibers were smaller than type I fibers in COPD women, while in male patients both fiber types exhibited a similar size.
Damage and muscle regeneration: The proportion of abnormal muscle (a mixed surrogate for the presence of damage and repair phenomena) was higher in both COPD groups than in their controls, with no significant differences between sexes. However, when this general index was divided into its different components, the percentage of muscle with abnormal or necrotic fibers (a surrogate of muscle injury) was increased in COPD women not only when compared with their female controls but also with COPD men. This difference was present even in women with a moderate lung disease. Conversely, COPD women showed a lower proportion of muscle with internalized nuclei (a surrogate of the initial stages of regeneration) than COPD men. In addition, the proportion of abnormal muscle directly correlated with the degree of airway obstruction, the BODE index, and the proportion of type II fibers and inversely with the oxygen saturation at the end of the walking test and the level of physical activity in COPD women (Figure 1(c) to (f)).
Gene expression: COPD women showed no significant differences with their healthy controls in the expression of key genes involved in myogenesis (Table 6). However, their Pax7, MyF5, and M-cadherin expression levels were higher than those observed in COPD men. No differences were observed between each one of the COPD groups and their specific healthy controls for those genes linked to cell stress or encoding adhesion molecules or proinflammatory cytokines. However, COPD women showed a higher expression of integrin β, RI of TNF-α, and the receptor of IGF-1 than COPD men. Moreover, the expression of TNF-α and its two receptors was directly correlated with that of the different genes involved in stress and myogenesis, such as Pax7, MyF5, MyHC-emb, and MyHC-peri in COPD women (data not shown).
Molecular levels of key proteins: In addition to transcriptome levels, the protein levels of a few selected proteins related to inflammation were also determined (Table 7). Overall, they show similar results to the former, with no differences between COPD patients and controls, with the exception of the receptors of TNF-α, whose levels were higher in COPD women when compared with their female controls and, in the particular case of RII, with COPD men.

Correlations between the proportion of type II fibers and (a) the BODE index, (b) oxygen saturation at the end of the 6MWT (SpO2), and (c) the percentage of abnormal muscle; as well as between the latter and (d) the BODE index, (e) end-SpO2, and (f) the level of physical activity. 6MWT: 6-minute walking test; SpO2: oxygen saturation (oxymeter) at baseline; BODE: BMI, obstruction, dyspnea, exercise; BMI: body mass index.
Structural characteristics of the vastus lateralis muscle.a
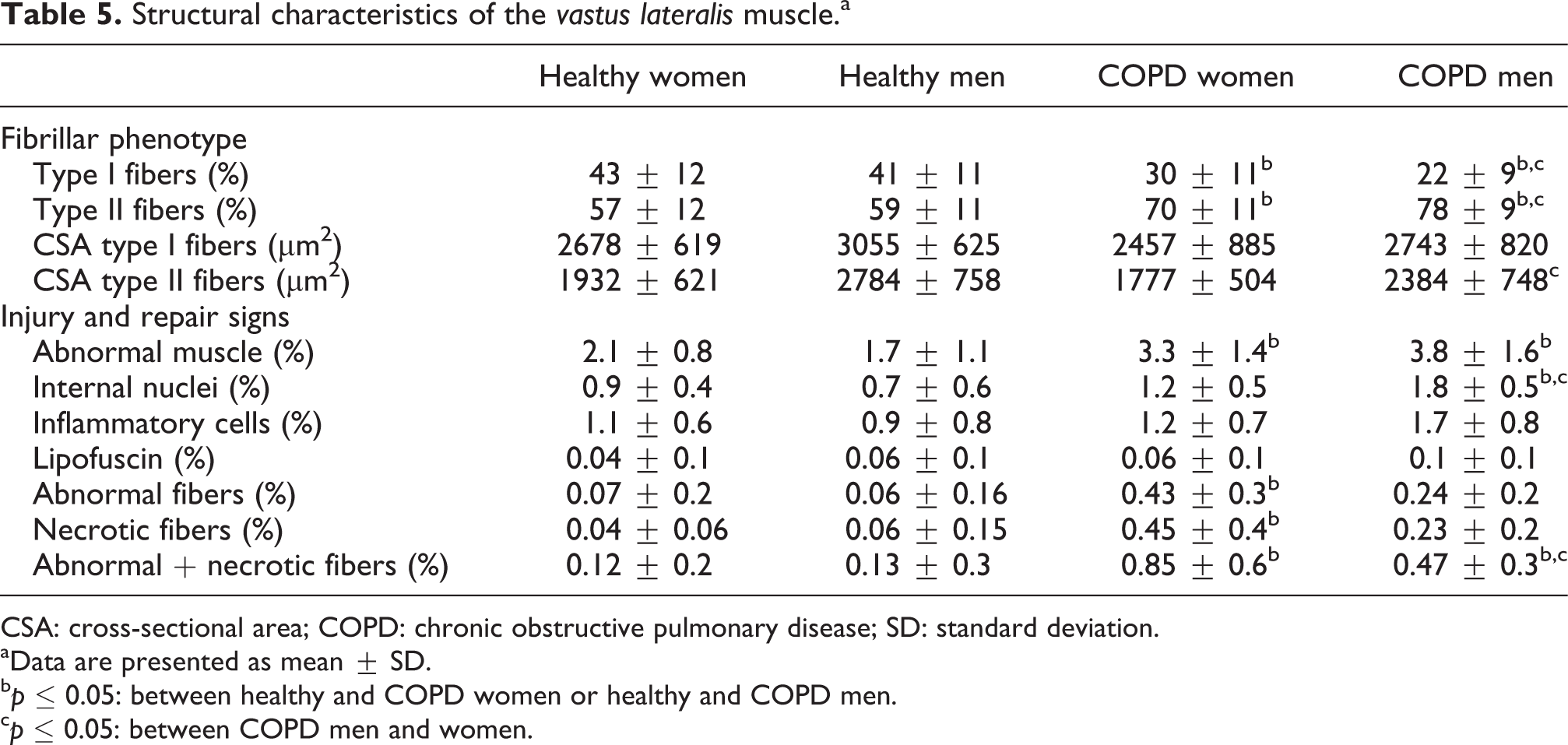
CSA: cross-sectional area; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD.
bp ≤ 0.05: between healthy and COPD women or healthy and COPD men.
cp ≤ 0.05: between COPD men and women.
Transcriptome expression

Pax7: paired box protein; MyF5: myogenic factor 5; Myo-D: myogenic differentiation 1; MyHC-emb: embryonic myosin heavy chain; MyHC-peri: perinatal myosin heavy chain; NCAM: neural cell adhesion molecule; CAV3: caveolin 3; ITG-β: integrin β; TNF: tumor necrosis factor; R: receptor; IL: interleukin; IGF-1: insulin-like growth factor 1; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
aData are presented as mean ± SD and normalized for the expression of each gene in healthy women.
bp ≤ 0.05: differences between COPD men and women.
Protein levels of different cytokines in the vastus lateralis muscle.a

TNF: tumor necrosis factor; IFN: interferon; IL: interleukin; VEGF: vascular endothelial growth factor; R: receptor; SD: standard deviation; COPD: chronic obstructive pulmonary disease.
aData are presented as mean ± SD.
bp ≤ 0.05: between healthy and COPD women or healthy and COPD men.
cp ≤ 0.01: between healthy and COPD women or healthy and COPD men.
dp ≤ 0.05: between COPD men and women.
Inflammation in systemic, pulmonary, and muscle compartments
Regarding inflammatory markers, no correlations of interest were obtained between the different body compartments analyzed in the study.
Tobacco and muscle findings
No differences were observed in different muscle variables between active smokers and ex-smokers. Moreover, no significant relationships were observed between the different muscle findings and the cumulative smoking index (pack-year).
Discussion
The present study describes some of the characteristics of muscle dysfunction profile in women with COPD. Probably, the most novel finding refers to the higher histological signs of injury observed in the quadriceps muscle of female COPD compared to those shown by men, although their levels of lung function impairment, nutritional status, systemic inflammation, and physical activity were similar. Moreover, this phenomenon was evident even in moderate stages of the disease. The opposite occurred with early signs of muscle regeneration, which were slightly lower in COPD women than in men. Moreover, the shift toward an increase in the proportion of type II fibers was lower in COPD women when compared with that observed in men. This study also confirms some findings of previous authors regarding the greater decrease in muscle strength and exercise capacity shown by COPD women and their higher perception of dyspnea. It also confirms the absence of relationships between the levels of systemic, lung, and muscle inflammation.
The patients of the present study showed muscle dysfunction, expressed by a decrease in quadriceps strength. As mentioned, this decrease was more pronounced in women, even after normalization for FFM (absent in previous studies), indicating that the intrinsic properties of the muscle were more altered in females. Moreover, the loss of strength in COPD women was related to their amount of physical activity, reinforcing the idea of a key role for this factor as an inductor of muscle deconditioning in the genesis of muscle dysfunction. Unfortunately, we have no data on the modalities of physical activity, which although quantitatively similar between COPD women and men, could have been qualitatively different among them. Conversely, the absence of detectable relationships between smoking and muscle findings suggests that this factor has not been determinant in the findings of the present study. Moreover, COPD women with a cumulative smoking index lower than that of men showed higher levels of muscle damage. Therefore, we should recognize that an increased susceptibility of female muscle to tobacco cannot be completely ruled out.
In contrast with the lower limbs, the function of the upper limb muscles showed no differences between patients and healthy subjects. This confirms earlier findings of our and other groups, which demonstrated that muscle phenotype is more preserved in the upper limb muscles, probably due to less severe muscle deconditioning and phenotypic changes. 44 –46
As for structural muscle findings, COPD patients showed the increase in the percentage of type II fibers classically observed in this condition 21,23 but this switch was markedly lower in COPD women than in men. This is especially relevant since, as mentioned, this occurs even though both populations showed similar nutritional status and levels of bronchial obstruction, systemic inflammation, and physical activity. Interestingly, the percentage of type II fibers in women was associated with the degree of hypoxemia during exercise. Although, given the nature of the present study, it is not possible to infer a cause–effect relationship several authors have shown that the level of oxygenation may modulate fiber phenotype in skeletal muscles. 47,48 Also estrogens, with very low levels in our patients but with potential residual effects from preceding years, may have influenced their muscle phenotype. 49,50 Interestingly, our group in collaboration with other international teams has recently shown the importance of the switch in fiber types occurring in the quadriceps muscle of COPD patients to predict mortality. 51 Moreover, our COPD women showed higher histological evidences of muscle damage than healthy controls and even than COPD men. The latter, in contrast, showed greater signs of early steps of muscle regeneration than COPD women. As a whole, these findings suggest different susceptibility of patients of both genders to injury that may have been caused by different stimuli, including tobacco (many of the patients were active smokers) and/or exercise. 26,52 The fact that COPD men showed greater signs of early regeneration does not necessarily means that this reparative process will continue correctly until its end, since several groups have recently shown that it can fail in its final steps. 53 Moreover, all the differences observed should be taken with caution, as levels of muscle damage and repair were always relatively low in all groups included in the present study.
Although our results on muscle structure need further confirmation, they suggest that the rehabilitation management of women with COPD should have some specificities. Their lower shift toward a higher percentage of easily fatigable fibers, higher level of muscle damage, and lower level of signs of repair than those seen in men suggest that limb muscle training should be less intense in COPD women.
Another point of interest is the presence of a vit D deficiency in patients with COPD, which was more pronounced in women than in men and was present even in those with only moderate lung disease. In addition, vit D levels were associated with muscle strength in women, both in the upper and lower limbs. The trophic effect that vit D has on bone is very well known but its effects on muscle are less familiar to the medical community. However, it has been shown that vit D positively influences the maintenance of muscle mass. 54 It is possible to speculate that the deficit in this vit, perhaps derived from the lack of outdoor activity of the patients and easily preventable with oral supplements, had played a role in the structural and functional changes exhibited by our female patients.
The present results also confirm the absence of any relationship in the levels of inflammation (as indicated by the expression of specific markers) between systemic, pulmonary, and muscle compartments. This reinforces the idea that the initial trigger (i.e. tobacco) probably targets various organs separately and works against the theory of the inflammation spill over from the lungs.
Another interesting issue is the proportion of patients with low body weight and low muscle mass observed in this study, which was approximately one-fifth, with no differences between men and women. This proportion is close to those reported in previous studies conducted in North America and Northern Europe and much higher than previous studies performed in the Mediterranean area. 55 This geographical difference has been attributed to lifestyle divergences. Our higher proportion of patients with low body weight can probably be explained by the origin of the patients (clinics from a reference hospital), which has determined their major severity and phenotypic traits. In fact, previous studies conducted in Spain analyzed mild COPD, while the mean FEV1 of the present study was 39% ref. and the patients showed a predominance of the emphysema phenotype.
Study limitations
One limitation of the present study is the relatively small number of healthy subjects, which may have prevented the achievement of statistical significance in some variables. However, the ethical constraints of taking a biopsy from the quadriceps muscle in healthy subjects is obvious. Moreover, the control groups are similar to those used in previous studies and significant differences have been obtained in the main variables of the present one. We recognize that this circumstance requires caution with our conclusions, since further studies including the analysis of muscle samples from COPD women should confirm and extend our findings.
The muscle sample size was minimized for the same ethical reasons. This did not affect the structural and transcriptome analyses but has limited the number of proteins included in the study, and thus, only those considered as more relevant for the objectives were chosen. An interesting alternative to the study of damage and other muscle phenomena could be the use of blood biomarkers, such as those currently used for myocardial muscle injury. Unfortunately, to date, there is no validated marker that has proved to be sensitive enough for baseline conditions or mild-to-moderate efforts.
In conclusion, the present study has revealed functional and structural differences in peripheral muscles of women and men with COPD, also confirming other discrepancies in physiological outcomes and symptoms between genders.
Footnotes
Acknowledgements
The authors thank Esther Barreiro for her support, Esther Puig and Francesc Sanchez for their technical assistance in the laboratory, and Jonathan McFarland for his help in editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Plan Nacional SAF2011-26908 and SAF2014-54371, FIS 11/02029 and 12/02534, 2014SGR424, MTV3-07-1010, FUCAP 09 and 11, SEPAR 761, and CIBERES.