
Abstract
The aim of this study is to conduct a systematic review of published studies that evaluate the impact of pulmonary rehabilitation (PR) on survival and fall (including balance) in patients with chronic obstructive pulmonary disease at stability. OVID, Medline, EMBASE, and Cochrane collaboration library were searched for literature dating from January 1980 up to November 2014 as well as an update in October 2015. Two reviewers screened titles, abstracts and full text records, extracted data, and assessed studies for risk of bias; any disagreements were resolved by a third member of the team, and consensus was always sought. Initial searches yielded 3216 records but after review only seven studies were included and there were no studies focused solely on falls. Two cohort studies found some positive benefits of PR on balance, but the results were inconsistent across the studies. Regarding survival, two randomized controlled trials were conducted; one study showed significant survival benefit at 1 year, while the other one showed nonsignificant survival benefit at 3 years. Neither were adequately powered and in both, survival was a secondary outcome. There was only limited inconclusive evidence to show that PR has a significant beneficial effect on balance or survival.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous inflammatory lung disease characterized by progressive airway obstruction. It is the third leading cause of death worldwide. 1 Comorbidities include cardiovascular disease, diabetes mellitus, osteoporosis, increased risk of fall, and depression. 2 In general, impaired mobility, muscle weakness, and impairment of balance due to chronic diseases are strong predictors of fall in adults; 3 recent studies have found that balance is impaired in patients with COPD. 4 A recent Cochrane systematic review showed evidence that falls in elderly can be prevented with exercise. 5 Exercise, with balance training, has been recommended in the guidelines for prevention of falls in older people with grade B evidence. 6
Pulmonary rehabilitation (PR) is an important part in the clinical management of COPD, and it includes education, exercise training, and psychological support. 7 There are demonstrable improvements in exercise tolerance, muscle strength, dyspnea, and quality of life in patients with COPD after PR, cemented in a Cochrane review 8 and the British Thoracic Society (BTS) guidelines. 9 Improving muscle strength and exercise tolerance through PR as well as the opportunity for educational support and improving confidence may well therefore improve the risk of future falls. Given patients with COPD have a high prevalence of osteoporosis, 2 an increased risk of falls is of even more concern. Further quality of life in the older population as a whole is associated with falls.
While a systematic review of six clinical trials has shown survival benefit in those undergoing PR in patients with COPD after an acute exacerbation, 10 the situation in stable patients undergoing standard PR is uncertain. The BTS PR guidelines document research recommendations and include need for research on comorbidities, preserving health, personalization of PR, and extending the outcomes used. 9 The aim of this study is to conduct a systematic review of published studies that evaluate the effect of a PR program on stable patients with COPD to determine if there is benefit with regard to balance, falls, and survival.
Method
Searches were conducted through OVID on Medline, EMBASE, Cochrane collaboration library, and the register of controlled trials from January 1980 until November 2014 and through an update in October 2015. The search yielded adult human studies on patients with COPD who have had standard PR not less than 4 weeks; the outcome measures were balance, fall, survival, and mortality. The search was conducted with the University library services who approved the search terms and methodology structure. The search was limited to articles in “English” and “humans.”
Using the population, intervention, comparison, outcome, and setting model, the criteria were: The population: Stable adult patients with COPD. The intervention: Standard multidisciplinary PR of not less 4 weeks. The comparator/control: Other patients with COPD did not have PR. The outcome: balance, fall, survival, and mortality. The study design: Either cohort or clinical trials from 1980 onward.
The following key words were used: “Pulmonary Rehabilitation”; “COPD” or “chronic obstructive pulmonary disease”; “chronic obstructive lung disease”; “Chronic bronchitis”; “emphysema”; “bronchitis”; “mortality” or “death”; “survival”; “survive”; “fall”; “faller”; “falling”; “accidental fall”; “balance” and “imbalance.” We conducted this review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (Online supplementary Table E1). 11
Two reviewers independently assessed the titles and abstracts; they evaluated the full text studies based on outcome and type of rehabilitation program for at least 4 weeks. These studies were evaluated and selected independently for inclusion in the systematic review. Any disagreements were resolved by a third member of the team, and consensus was always sought. Additional studies were searched for the bibliographies and relevance of the retrieved articles. Studies that did not fulfil the selection criteria were excluded.
Two reviewers independently extracted the full text of the included articles and recorded details on authorship, year of publication, study design, interventions, patient, and outcome measures. Risk of bias was assessed using the Cochrane collaboration’s “Cochrane risk of bias tool (modified) for quality assessment of the randomized control trial (RCT)” for sequence generation, allocation concealment, and blinding. 12 The Newcastle–Ottawa scale (NOS) was used to assess the methodology and quality of the cohort studies; the scale awards four points for selection, two points for comparability, and three points for outcome—a score of 9 is the highest. 13
Results
A total of 3216 citations were identified from the databases in the original search; seven studies that met the eligibility criteria of the review, of which two were RCTs and five were cohort studies, were selected (Figure 1). 14 –20 The quality of the cohort studies, as assessed by the NOS with a mean score of 6 out of 9, with points loss due to sampling method or inadequate time for follow-up. 13 For the two randomized trials, the quality of the included studies reporting was high; allocation concealment and sequence generation were clearly described in both trials. But one trial did not use blinding, while the other was only single-blinded. No quantitative analysis was performed due to the lack of data to comparable outcome data to combine. In general, the studies did not show major problems of bias, for detailed characteristics of the included studies and quality assessment for risk of bias, see Online supplementary Tables E2 to E8.
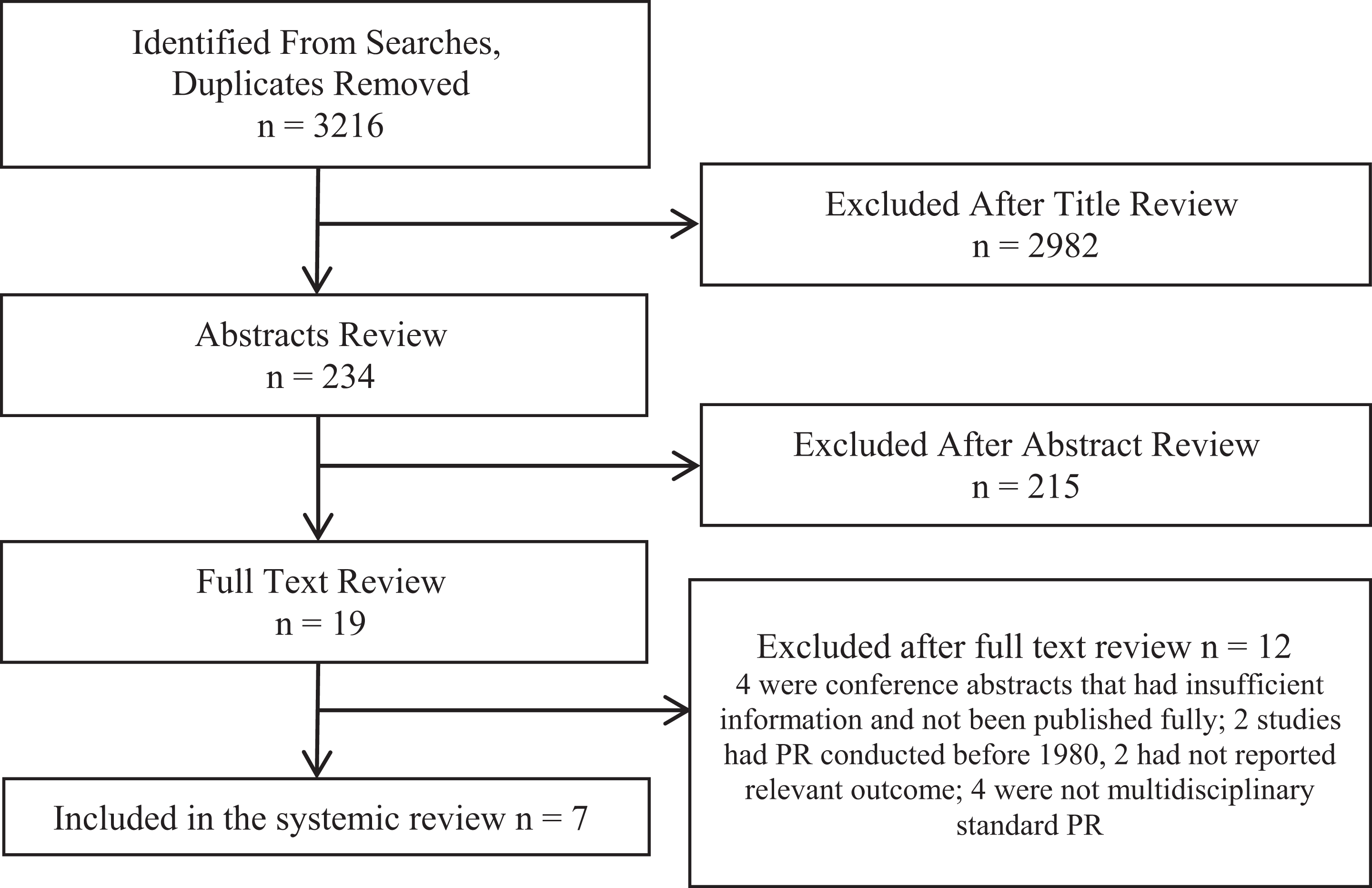
Flow diagram of the selection process of studies included in the systematic review.
Fall/balance
There were no studies that report of the impact of PR on falls directly, while two cohort studies evaluated the effect of standard PR on balance in patients with COPD (Table 1). Both studies assessed the balance tests using minimum detectable change (MDC) as the true change in the balance. The first cohort study by Beauchamp et al. 15 studied 29 patients with COPD (pre- and post-PR) and found significant improvement in measures of balance, the Berg Balance Scale (BBS; BBS mean difference = 2.8 points; 95% confidence interval (CI; 1.7 to 3.8); p < 0.001), and the time up and go test (TUG; (TUG mean difference = −1.5 s; 95% CI (−2.4 to −0.5); p = 0.003] but not for self-assessed balance confidence score as measured by Activities-specific Balance Confidence (ABC) Scale (mean difference = 4.8; 95% CI (−1.0 to 10.7), p = 0.1). In the second study by Beauchamp et al., 14 they conducted a randomized clinical trial by comparing standard PR with PR + balance training. Based on our inclusion criteria, we have taken only the control arm of this trial (PR) and treated as a cohort study. Here, patient inclusion criteria also included a self-reported decline in balance, fall in the last 5 years or a near fall. Within this control arm, 17 patients (pre- and post-PR program) were studied and this time the results showed no significant improvement in the BBS (mean difference = 1.6 points; 95% CI (−0.26 to 3.46), p = 0.07); but there was significant improvement in ABC confidence (mean difference = 13; 95% CI (3.72 to 22.27), p = 0.014). Here, the Balance Evaluation Systems Test (BESTest) showed significant improvement as well (mean difference = 6; 95% CI (3.39 to 8.60), p = 0.0003).
Two cohort studies assessing the impact of PR on fall/balance.

PR: pulmonary rehabilitation; BBS: Berg Balance scale; BESTest: balance evaluation systems test; ABC: activities-specific balance confidence scale; TUG: timed up and go test.
aStudies’ quality assessed by Newcastle–Ottawa scale. Characteristics of the studies (online Appendix).
Survival
Three cohort studies 16 –18 (Table 2) and two randomized controlled trials 19,20 (Table 3) contributed to the mortality data with PR. In 1996, a cohort study by Gerardi et al. 18 investigated survival in 158 patients (of which 87% had COPD) who had completed the PR program, and the survival rate was 80% at 3 years after rehabilitation. In another cohort study by Bowen et al. 16 in 2000 (of which 89% had COPD), the survival rate in 149 patients who completed the PR program was 95% at 1 year, 92% at 2 years, 85% at 3 years, and 73% at 4 years after rehabilitation. In the third cohort study by Connor et al. 17 in 2001 on 170 patients, the 1-year survival rate was slightly lower than Bowen’s study at 91%.
Cohort studies assessing the impact of PR on mortality.

PR: pulmonary rehabilitation: COPD: chronic obstructive pulmonary disease.
aStudies’ quality assessed by Newcastle–Ottawa scale. Characteristics of the studies (online Appendix).
Randomized control trials assessing the impact of PR on mortality.

PR: pulmonary rehabilitation: COPD: chronic obstructive pulmonary disease.
aStudies’ quality assessed by the Cochrane collaboration risk of bias tool. Characteristics of the studies (online Appendix).
Two RCTs 19,20 compared the survival rate between PR and control groups (Table 2), where survival was a secondary outcome in both cases. In 1995, Ries et al. 20 studied two groups of patients; 57 patients (rehabilitation) received the standard PR program and 62 patients (control) received only the PR education component. They found at 3 years that 85% survived in the rehabilitation group compared to 74% among the control group; and at 6 years, 67% in rehabilitation and 56% in the control group survived. Although the PR survival was better, there was no significant difference in survival rate (Hazard ratio = 0.74 (95% CI, 0.41–1.34; p = 0.32)). In the second trial in 2000, Griffiths et al. 19 compared a standard rehabilitation group (92 patients) with a control group (90 patients); survival was reported as a supplementary result of their study. By year 1 of the study, 94.5% survived in the rehabilitation group compared to 90% in the control group (p = 0.032).
Discussion
This systematic review identified a paucity of studies that focus on the effect of PR on falls, balance, or survival. In the two studies that examined any potential benefit of PR on balance, the results were not consistent across the two studies even though each of them demonstrated a significant improvement in at least one of the balance scores. The survival in patients with COPD who had PR at clinical stability appeared to show some benefit; however, this was not always statistically significant.
The identified studies on balance 14,15 have small sample size and they have excluded patients with many comorbidities that could influence their balance. Small statistical differences in some of the balance tests were found, but these were not consistent across the studies. Previous research have shown that patients with COPD have worse balance score on their BBS test compared with healthy individuals. 21,22 The balance tests used in the studies (BBS, TUG, and BESTest) and the ABC balance confidence are important as they have shown reliable and valid results for determining balance and fall risk in adults. 23 –26 In addition, they have been used to evaluate the ability to maintain balance and quantify patients with COPD at risk of falling. 3,27 Both cohorts used MDC instead of the minimum clinically important difference (MCID). “Statistically significant difference” does not necessarily mean “clinically important” in terms of a clinically demonstrable change. Recently, Beauchamp carried out a secondary analysis to determine the MCID of the BBS, BESTest, and ABC. 28
Previous evidence has shown that exercise reduces falls in the elderly. 5 Furthermore, studies have found that standard PR with adding balance training component had a better effect on functional balance and muscle strength in patients with COPD, which should in turn lead to reduced falls. 29,30 In the current evidence, therefore, patients at risk of falls undergoing PR should have a personalized balance training.
PR has been associated with improved survival in patients with COPD after an acute exacerbation. 31 However, the evidence that PR is associated with improved survival in stable patients with COPD is not as clear. The RCTs included in this review were underpowered to show a difference in survival. They both showed improved survival, but they were not statistically significant. 19,20 In addition to the RCT’s, we identified the three cohort studies that showed survival following PR, though it is difficult to then compare with other reports of survival in patients with COPD generally. The 4 year survival in a general cohort of patients with COPD was 81%, 32 in one study and as expected, varied according to severity of COPD in another study. 33 When assessed according to airflow obstruction alone, survival at 52 months was 75% for patients with stages I (FEV1 > 50) and II (FEV1 36–50) and 48% for stage III (FEV1 < 35). 33 Overall, although evidence on PR has shown significant improvement in the quality of life and dyspnea, the outcomes of balance, fall, and survival are less clear.
The main strength of this review was in the rigorous study selection process, and therefore it is unlikely to have missed any research in this area. The main limitation of this review was the lack of studies and evidence for evaluating the desired outcomes. Moreover, Gerardi et al. 18 and Bowen et al. 16 have included patients with diagnoses other than COPD, although the majority did have COPD. It was not possible to look at survival in those with COPD alone.
In conclusion, this systematic review is unable to demonstrate sufficient evidence of the role of PR in improving balance or survival in patients with COPD. Further studies with alternative strategies may need to be employed to determine the benefits of PR particularly on survival as the short-term benefits from pulmonary are well established and therefore unethical to withhold from patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ali Hakamy has carried out this study as part of his PhD program at University of Nottingham. He has received scholarship award from Ministry of Education (Saudi Arabia). No other support from any other organization for the submitted work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.