
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) significantly impacts respiratory and motor function, balance, and cognition, leading to muscle weakness and impaired exercise capacity. The impairments often result in challenges with daily activities, particularly those requiring dual-tasking.
Objectives:
The study investigated whether patients with severe COPD would exhibit more significant cognitive and motor performance decline during dual tasks compared to healthy controls.
Design:
This study employed a cross-sectional design to compare cognitive and motor performance in dual tasks between patients with severe COPD and healthy controls.
Methods:
We included 44 patients with severe COPD and 43 healthy individuals. Participants underwent various tests, including pulmonary function tests, six-minute walking tests, dual Timed Up and Go tests (TUG), dual single-leg stance tests (SLS), Berg Balance Scale assessments, and Falls Efficacy Scale International evaluations (FES-I).
Results:
The COPD group had significantly lower scores in the Berg Balance Scale (BBS; 44.79 ± 4.70 vs 52.67 ± 2.16, p < 0.0001) and longer times for the TUG test (12.44 s; [11.44, 13.50] vs 9.14 s; [7.91, 10.11], p < 0.0001) and shorter times for the SLS test (14.15 s; [12.31, 15.65] vs 26.20 s; [23.45, 30.88], p < 0.0001), indicating poorer functional mobility and balance. Furthermore, dual-task interference (DTI) outcomes revealed poorer performance in the COPD group (p < 0.0001). The fear of falling (FES-I) was increased in the COPD group. There was a significant positive correlation between DTI TUG and FES-I (r = 0.35, p = 0.01) and a negative correlation between DTI SLS and BBS (r = −0.41, p = 0.005) in the COPD group.
Conclusion:
The study reveals significant impairments in DTI and balance among patients with severe COPD. Patients with severe COPD performed worse in tests involving dual tasks. They had poorer balance overall compared to healthy controls, with longer times for the dual Timed Up and Go test and shorter times for the SLS test, indicating a higher susceptibility to DTI and a greater fear of falling.
Plain language summary
Introduction
The concept of dual-task refers to the simultaneous performance of two tasks, typically a motor task combined with a cognitive task. 1 This paradigm is increasingly relevant in evaluating cognitive and motor functions in elderly individuals due to its ability to mimic real-life scenarios and its sensitivity to age-related decline. 1
Chronic obstructive pulmonary disease (COPD) is a common and debilitating respiratory disease that affects over 250 million people worldwide. 2 It significantly affects respiratory function, motor function, balance, and cognition. 3 Due to systemic inflammation, inactivity, and corticosteroid use, COPD patients often experience muscle weakness and wasting, particularly in the lower limbs, leading to difficulties in walking, climbing stairs, and performing daily activities. 4
Reduced exercise capacity is another hallmark of COPD. Patients experience fatigue and breathlessness during physical exertion, further limiting their activity levels. 5
Balance problems are also common in COPD, as impaired postural control and muscle weakness increase the risk of falls. 6 This risk is further exacerbated by medication side effects and cognitive impairments associated with COPD, which often manifest as difficulties with attention, memory, and executive function. 7
The combination of motor, balance, and cognitive impairments can make dual-tasking, such as walking while doing simple math, particularly challenging for COPD patients. 8 Dual-tasking in the context of COPD typically involves combining a physical task (related to mobility or exercise) with a cognitive task (related to memory, attention, or decision-making).9,10 Dual-task performance and balance are essential for maintaining independence and avoiding falls in older adults. However, people with COPD are at increased risk of falls due to several factors, including dyspnea, which can lead to changes in breathing patterns. 11 These changes may result in altered gait, decreased stride length, reduced walking speed, muscle weakness, and impaired balance.11,12 Dual-task interference (DTI) is the decrease in performance on one or both tasks when performed simultaneously, compared to when performed individually. 13 This phenomenon occurs because our cognitive sources, such as attention and working memory, are limited, and performing two tasks at once can overload these resources, leading to a decline in performance. 14
The existing literature on dual-task performance in patients with COPD is currently limited. A study by Heraud et al. found that patients with COPD are highly susceptible to DTI, as indicated by increased gait variability when simultaneously performing cognitive and walking tasks. 15
Ozsoy et al. found that while there was no significant difference in the time to complete a motor task alone, patients with COPD showed greater impairment in cognitive performance during the dual-task conditions. 8
By understanding DTI, we can gain valuable insights into how patients with COPD allocate resources and coordinate different processes. This knowledge can inform strategies for improving multitasking performance and reducing the negative effects of DTI in various contexts.
We hypothesized that cognitive and motor performance deterioration during dual tasks would be worse in the COPD group than in healthy controls. This is the first study to compare dual-task interference between patients with severe COPD and healthy controls.
Methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 16
Study design
This study employed a cross-sectional design to compare cognitive and motor performance in dual tasks between patients with severe COPD and healthy controls. The study was conducted at the Pulmonary Rehabilitation Center, Clinical Hospital of Infectious Diseases and Pulmonology, “Victor Babeş” in Timisoara, Romania, between May 2023 and February 2024.
Participant recruitment and consent
Patients with severe COPD were recruited from those seeking treatment at the Pulmonary Rehabilitation Center, and healthy controls were recruited from individuals who came for routine health checks during the same period.
All participants were informed about the study objective and procedures. Before enrollment, written informed consent was obtained from each participant. The study protocol was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki. 17
Patients with COPD were included if they met the following criteria: age over 40 years, smoking history of more than 20 pack-years, forced expiratory volume in 1 second 30% ⩽ (FEV1) < 50% predicted for severe COPD and FEV1 < 30% predicted for very severe COPD, FEV1/forced vital capacity (FVC) ratio less than 0.7 predicted (post-bronchodilation), modified Medical Research Council (mMRC) dyspnea scale ⩾ 2, and physician diagnosis of COPD. 18
Healthy controls were included if they were over 40 years old and had no history of respiratory disorders. Exclusion criteria for both groups included medications that could affect how their bodies respond to exercise, postural orthostatic hypotension, conditions that cause dizziness or fainting when standing up, neurological or musculoskeletal conditions that could increase the risk of falls and balance problems, such as Parkinson’s disease, stroke, or recent lower-extremity joint replacements, COPD exacerbations in the past 3 months, or impaired vision.
Data collection
At admission, all participants underwent a pulmonary function test (PFT), a six-minute walking test (6MWT), a Timed Up and go test (TUG), a Single-Leg Stance test (SLS), Berg Balance Scale (BBS), and completed Falls Efficacy Scale—International (FES-I) questionnaire. During the dual-task tests, participants were instructed to perform cognitive and physical tasks simultaneously. The balance tests, including the Berg Balance Scale, were part of the specific research protocol, not routine clinical evaluations.
Outcome measures
Pulmonary function test
We used the Smart PFT UI device Medical Equipment Europe GmbH provided to assess pulmonary volumes. Spirometry is a non-invasive pulmonary function test that measures various lung volumes and flow rates during a forced expiration. 19 We evaluated the following parameters: forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), and FEV1/FVC ratio post-bronchodilator.
Six-minutes walking test
The six-minute walking test is a simple, non-invasive measure of functional exercise capacity commonly used to assess cardiopulmonary fitness and exercise tolerance in patients with various conditions such as COPD. The patients were instructed to walk comfortably along a marked path or corridor as far as possible for 6 min. The total distance walked in 6 min was recorded. 6MWT (%) represents the patient’s achievement (%) in relation to the anticipated distance of a healthy patient. A lower 6MWT distance indicates reduced exercise tolerance and may suggest underlying cardiopulmonary or neuromuscular impairment. 20 The 6MWT was performed on a 30-meter walkway with markers at each end. The patients were given standard instructions and performed the test twice, with the second test completed 2 h after the first test. 20 The second test was recorded.
Timed Up and Go test
The Timed Up and Go test is a simple, non-invasive tool for assessing functional mobility and balance in older adults and individuals with neurological or musculoskeletal conditions. The test measures an individual’s time to stand up from a standard armchair, walk at their average pace to a line 3 m away, turn around, walk back to the chair, and sit down again. The results are interpreted based on the time taken to complete the task. A longer time indicates poorer functional mobility and balance. 21
The TUG test is a single-task assessment, and it is important to consider the ability to perform dual tasks, which are more representative of real-world activities when assessing fall risk.
The dual-task TUG test is a modification of the TUG test that incorporates a cognitive task while the individual is walking. This dual-task challenge is more demanding and can provide a more comprehensive assessment of an individual’s ability to navigate their environment safely. 22
Three repetitions were performed for each test. The best test was recorded. Patients rested between each test as needed. Patients rested for at least 1 h between the two types of tests.
Single-leg stance
The SLS test is a simple and noninvasive static balance assessment commonly used in clinical settings to evaluate postural stability and fall risk. The test involves standing on one leg for as long as possible while keeping the other leg bent at the knee and off the floor. 23
The results of the SLS test are interpreted based on the time the participant can maintain a Single-Leg Stance with each leg. A shorter time indicates poorer static balance and increased fall risk. 24 Each test was performed three times, with the best result recorded, and patients rested as needed between tests.
Cognitive task
After performing the single-task TUG and SLS, participants completed the dual-task TUG and SLS. In both tests, participants were instructed to simultaneously perform the test and count backward 7 from 100. As an indicator of cognitive performance, the rate of correct responses (RCR) was calculated using the formula: number of correct answers/numbers of = responses × 100. The values are presented in %.
Berg Balance Scale
The BBS is a widely used and reliable tool for assessing balance in individuals of all ages. It is a 14-item questionnaire that evaluates a variety of static and dynamic balance tasks, such as standing with feet together, standing on one leg, turning around, and reaching down to pick up an object. The BBS is scored on a 5-point scale, with a maximum score of 56. A higher score indicates better balance, while a lower score indicates poorer balance. 12
Fear of falling
The Falls Efficacy Scale—International (FES-I) is a 16-item questionnaire designed to assess an individual’s concern about falling. It is a valuable tool for identifying individuals at risk of falls and evaluating the effectiveness of fall prevention interventions. The total score is calculated by adding the scores for all 16 items. A score of 28 or higher is considered a heightened concern about falling. 25
Statistical analysis
The data and analysis were conducted using a licensed edition of MedCalc® Statistical Software version 22.016 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2023). The plot distribution was analyzed using the Shapiro–Wilk test.
This study determined the sample size based on the ability to detect significant differences in key outcomes between the control and COPD groups using standard statistical power analysis techniques. Using Cohen’s d for effect size estimation, where a large effect size (d = 1.2–1.5) was anticipated based on the provided data, we calculated the required sample size to achieve a power of 0.8 at a significance level (α) of 0.05. The calculations indicated that each group would need approximately 12 participants to detect the observed differences with sufficient power. However, to ensure robustness and account for variability, we included 43 participants in the control group and 44 participants in the COPD group. These sample sizes are well above the calculated minimum, providing confidence in the statistical validity and reliability of the study’s findings.
The central tendency indicators were defined as the arithmetic mean and standard deviation (SD) for parametric variables and the medians and interquartile range [IQR] for non-parametric data.
The parameters were compared using either an independent samples t-test or a Mann-Whitney test for independent samples. Chi-squared test was used to determine the difference between the observed proportions in categorical data. The Wilcoxon signed-rank test, a non-parametric test, was used for comparing two related samples or repeated measurements on a single sample to assess whether their population mean ranks differ.
Correlation analysis was performed to determine the strength and direction of the relationships between data from two groups: COPD patients and COPD patients with long-term oxygen therapy (LTOT). The Pearson correlation coefficient (r) was used for this purpose. Correlations were interpreted based on the strength of the relationship. Correlations were interpreted according to the magnitude of the association. The manuscript only presented correlations that were moderate or strong (|r| > 0.3).
A p-value of less than 0.05 was deemed statistically significant.
Results
We included 44 patients with severe COPD and 43 healthy individuals. According to our results, the following parameters from the COPD group—height, FVC, and FEV1 showed a parametric distribution. For the rest of the parameters, the Shapiro–Wilk test demonstrated a non-normal distribution; non-parametric tests were performed for these parameters.
Based on these findings, the parameters of the control group, including height, weight, BMI, FVC, FEV1, FEV1/FVC, TUG, TUG-dual, and FES-I, presented a parametric distribution. The Shapiro–Wilk test reveals a notable deviation from normality for the remaining parameters, necessitating non-parametric testing.
Baseline characteristics of the control group
Out of a sample size of 43 individuals, 33 (76.74%) were identified as male. The individuals’ ages ranged from 45 to 68, with a median age of 63.00; [61.25, 65.75]. The individuals’ heights ranged from 156 to 183 cm, with a mean of 175.04 ± 5.96 cm. The individuals’ weights ranged from 54 to 106 kg, with a median of 80.00 [73.50, 86.75]. The anthropometric measurements suggest a group with an average height of about 175 cm and a median BMI in the normal to overweight range. A significant portion has hypertension and cardiovascular disease, while a smaller percentage has diabetes or obesity. Pulmonary function is within normal ranges, with sPO2, FVC, FEV1, and the FEV1/FVC ratio indicating generally good respiratory health. No participants are on LTOT.
Baseline characteristics of the COPD group
Out of a sample size of 44 individuals, 34 (77.27%) were identified as male. The patients’ ages ranged from 54 to 72, with a median age of 64.00; [62.50, 66.00]. The patients’ heights ranged from 162 to 188 cm, with a mean size of 171.86 ± 7.12 (mean ± SD). The patients’ weights ranged from 44 to 134 kg, with a median of 58.50 [53.00, 91.00]. The patients’ BMI varied from 16.40 to 41.20, with a median of 19.40 and a range of [17.60, 30.95]. A significant portion has hypertension and cardiovascular disease, with a smaller percentage having diabetes or obesity. Almost half (45.45%) of the participants are on LTOT. The group has a lower average height and a wide range in weight and BMI, with the median BMI indicating an underweight to normal weight status. Pulmonary function is significantly impaired compared to typical values, as reflected in the reduced FVC, FEV1, and FEV1/FVC ratio. The distinguishing characteristics of the patients are displayed in Table 1.
The comparison of baseline characteristics between the two groups.

The data presented in the control and COPD groups are expressed as value (percentage), arithmetic mean ± SD or median, and [IQR].
BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; GOLD, Global Initiative for Obstructive Lung Disease; LTOT, long-term oxygen therapy; SPO2, peripheral capillary oxygen saturation.
The outcomes of the control group and the COPD group are presented in Table 2. These comparisons demonstrated strong statistical power (p < 0.0001), with lower results in the COPD group in 6MWT and BBS and higher scores in FES-I.
The comparison of outcomes between groups (control vs COPD).

Results are expressed as arithmetic mean ± SD or median and [LQ, UQ].
BBS, Berg Balance Scale; DTI, dual-task interference; FES-I, Fall Efficacy Scale International; RCR, rate of correct responses; 6MWT, six-minutes walking test; SLS, Single-Leg Stance test; TUG, Timed Up and Go test.
The lowest RCR value in the COPD group was 40%, while the control group’s lowest value was 60%. Both groups had the highest value of 100%. The median RCR for the first group was 75%, with a 95% confidence interval ranging from 66.67 to 75 and an interquartile range of 60–75. The control group had a median RCR of 80%, a 95% confidence interval of 75.0–100.0, and an interquartile range of 75.0–100.0.
DTI TUG of the control group was 2.79 ± 0.37 s. The DTI TUG for COPD group was 3.44 ± 0.59 s. The p-value is less than 0.0001, indicating that the difference in the DTI TUG times between the two groups is statistically significant.
Based on DTI SLS, the control group had a mean time of 2.90 s with a standard deviation of 0.87 s. The COPD group had a mean time of 4.25 s with a SD of 0.80 s. The p-value is less than 0.0001, indicating that the difference in the DTI SLS times between the two groups is statistically significant. The comparison of outcomes between groups is presented in Table 2. The graphical representation of TUG and TUG-dual scores within the control group and COPD group is presented in Figure 1. Furthermore, the graphical representation of SLS and SLS-dual scores within the control group and COPD group is presented in Figure 2.
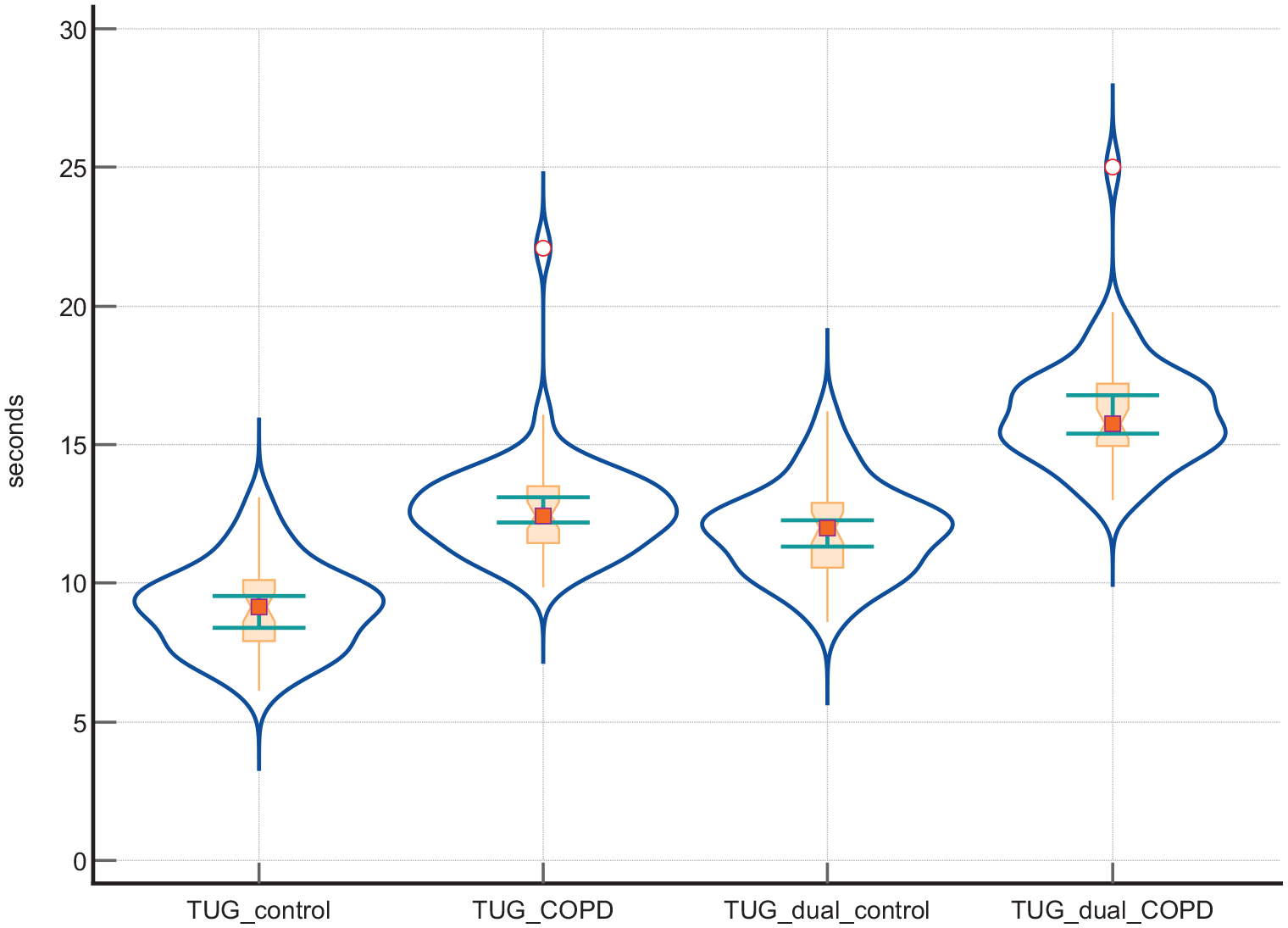
The graphical representation of TUG and TUG-dual scores within the control group and COPD group (dot-and-line diagram with violin plot representation, notched box-and-whisker with markers and connecting lines).

The graphical representation of SLS and SLS-dual scores within the control group and COPD group (dot-and-line diagram with violin plot representation, notched box-and-whisker with markers and connecting lines).
The differences between single and dual-task TUG for COPD showed a statistically significant median difference of 3.45 (95% CI: 3.25–3.65) with all 44 patients performing worse on the dual task, confirmed by a Wilcoxon test (Z = −5.78, p < 0.0001). In control group, a statistically significant median difference of 2.785 (95% CI: 2.65–2.90) with all 43 participants performing worse on the dual task (Z = −5.71, p < 0.0001).
The differences between single and dual-task SLS for COPD patients showed a statistically significant median difference of −4.3 (95% CI: −4.5 to −4.05) with all 44 patients performing worse on the dual task (Z = −5.78, p < 0.0001). In control group, was demonstrated a median difference of 2.9 (95% CI: −3.2 to −2.6) with all 43 participants performing worse (Z = −5.71, p < 0.0001).
The results based on the Pearson correlation coefficient indicate a statistically significant moderate positive correlation between DTI TUG and FES-I (r = 0.35, p = 0.01) in the COPD group, suggesting these two parameters tend to increase together. However, in the COPD group with LTOT, while there is a moderate positive correlation between DTI TUG and FES-I (r = 0.40), the p-value of 0.07 suggests this correlation is not statistically significant at the 0.05 level. Lastly, there is a statistically significant moderate negative correlation between DTI SLS and BBS in the COPD group (r = −0.41, p = 0.005), indicating that as DTI SLS increases, BBS scores tend to decrease. These findings highlight the relationships between these parameters in different groups, though the implications of these relationships would need further investigation. Table 3 presents the relationship between DTI TUG, SLS, and test parameters (FES-I, BBS). Figure 3 presents the relationship between DTI TUG and FES-I in the COPD group.
The relationship between DTI TUG, SLS, and test’s parameters.

BBS, Berg Balance Scale; DTI, dual-task interference; FES-I, Fall Efficacy Scale International; LTOT, long-term oxygen therapy; SLS, Single-Leg Stance test; TUG, Timed Up and Go test.
COPD, Chronic obstructive pulmonary disease.

The relationship between DTI TUG and FES-I in the COPD group. Moderate positive linear correlation between DTI and FES-I for COPD group—scatter diagram and regression line with heat map, 95% confidence interval curve (blue area), 95% prediction interval curve (orange area). The background color of the heat map indicates the density of points, suggesting clusters of observations. Red indicates a high concentration of points, yellow indicates a moderate concentration of points, and blue indicates a low concentration of points. The orange circles represent the correspondence between plot data from the same patient’s FES-I (X-axis) and DTI (Y-axis).
Discussion
We compared dual-task performance and balance in patients with severe COPD to healthy controls. To our knowledge, this is the first study that evaluates dual-task performance in patients with severe COPD.
The results underscore the significant differences in physical function, balance, and respiratory health between the control and COPD groups. The COPD group exhibited poorer performance across all measured parameters, highlighting the impact of COPD on physical and functional abilities. We observed that patients with severe COPD exhibit impaired dual-task performance and balance compared to healthy controls. Patients with COPD were more susceptible to DTI, as indicated by increased gait variability when simultaneously performing cognitive and walking tasks.
The comparison between patients with severe COPD and healthy controls shows significant differences in the 6-minute walking test, Berg Balance Scale, Timed Up and Go test, SLS, and Falls Efficacy Scale - International. These differences highlight the substantial impact of COPD on functional capacity, balance, and the fear of falling (FOF). Patients with severe COPD performed significantly worse on the TUG test compared to healthy controls. The COPD group took longer to complete the TUG test (12.44 s vs 9.14 s in controls, p < 0.0001). When performing the dual-task version of the TUG test, the COPD group again took significantly longer (15.75 s vs 12,00 s in controls, p < 0.0001. Similarly, the COPD group exhibited poorer performance on the SLS test. They could maintain single-leg balance for a shorter duration than healthy controls (14.15 s vs 26.20 s, p < 0.0001. This difference was even more pronounced during the dual-task SLS, where the COPD group could only balance for 9.90 s compared to 23.20 s in the control group (p < 0.0001).
Our results indicate that patients with severe COPD have significantly impaired functional mobility and balance when a cognitive task is added to the tests. The longer times taken by the patients with COPD on the TUG and SLS tests, especially during dual-task conditions, highlight their increased risk of falls and reduced ability to perform daily activities that require simultaneous cognitive and physical abilities.
Ozsoy et al. observed that patients with COPD display a more significant decrease in cognitive and motor performances during dual-tasking compared to healthy individuals. The authors suggest several explanations for the findings, such as frontal lobe dysfunction and disease severity. 8 The authors observed a significant correlation between disease severity and cognitive DTI in the COPD group, indicating that as the severity of COPD increases, cognitive performance may be more negatively affected during dual-tasking. 8 Compared to Ozsoy’s study, we observed a higher baseline value of the TUG test and an increased TUG-dual time. An explanation for our results is that we analyzed only severe patients with COPD. Consistent with his findings, we previously observed that cognitive dysfunction significantly correlates with COPD severity and exacerbation phase. 26 In contrast with our study, Heraud et al. specifically looked at the impact of COPD on cognitive and motor performance during dual-task walking. 15 The authors found that COPD patients exhibited an exaggerated cognitive-motor interference during dual-task walking, characterized by increased gait variability, a parameter closely related to fall risk and disability. Stride time variability, an indicator of gait variability, was significantly higher in COPD patients compared to controls during dual-task walking. 15 This may be due to the motor control abnormalities observed in COPD patients during visual-guided quadriceps contractions. 27
Morlino et al. looked at gait abnormalities in COPD patients and their relationship to respiratory function. 28 The authors found that gait abnormalities in COPD, such as reduced gait speed and stride length, were not directly related to respiratory function parameters like FEV1. Instead, they suggest that gait impairments in COPD are likely multifactorial, involving factors like muscle weakness, deconditioning, and neurological changes. 28
In another study, Van Hove et al. focused on the influence of cognitive load on static balance in COPD patients. 29 The authors found that COPD patients had impaired balance compared to healthy subjects. Cognitive tasks mainly affected speed-related parameters, demonstrating that cognitive tasks during static balance tests altered postural control in both the control and COPD groups. 29 Consistent with his findings, we also observed that cognitive tasks during the static SLS test altered the postural control in both the control and COPD groups.
While our study focused on the behavioral outcomes of dual-task performance, Hassan et al. examined changes in oxyhemoglobin concentration in the prefrontal cortex during cognitive-motor dual-tasks in people with COPD. 30 The authors found that COPD patients exhibited increased oxyhemoglobin concentration in the prefrontal cortex during the dual-task performance compared to healthy controls. COPD may require greater prefrontal cortex activation to maintain dual-task performance, indicating increased cognitive effort. 30 This additional cognitive load may contribute to poorer dual-task outcomes in COPD patients.
Studies have shown a connection between increased FOF and negative consequences in older adults, such as limitations in physical function, reduced physical activity levels, and higher risk of falls.31,32 There is also early evidence suggesting that people with COPD may experience a heightened FOF.33,34 In the COPD group, higher FES-I questionnaire scores indicated increased FOF (27.50 vs 18.00, p < 0.0001) were observed. A statistically significant moderate positive correlation (r = 0.35, p = 0.01) was found between longer DTI TUG times and higher FES-I scores, reflecting a heightened FOF. However, in COPD patients on LTOT, a moderate positive correlation (r = 040.) was noted, but it did not reach statistical significance (p = 0.07). Similarly, Oliveira et al. also reported that patients with COPD had higher FES-I scores compared to healthy controls, suggesting an increased FOF in the COPD group. 35 The correlations between DTI TUG and FES-I, as well as DTI SLS and BBS, illustrate the impact of dual-task interference on mobility and balance in COPD patients. These findings suggest that COPD patients with more significant functional impairments also experience higher fear of falling and poorer balance, which are critical factors in their overall quality of life and risk of falls.
A systemic review and meta-analysis identified specific BMI categories that are associated with a higher risk of falls in community-dwelling older adults. 36 The findings of the study suggest that both underweight and obesity are significant risk factors for falls. The risk of falling increases with decreasing BMI, with the highest risk observed at BMI values below 18.5. 36 The data from our study shows that the median BMI in the COPD group was 19.40; [17.60, 30.95], which is significantly lower than the median BMI in the control group of 25.20; [24.00, 28.90] (p = 0.03). This difference in BMI between the two groups could significantly impact balance, as higher BMI values are generally associated with better postural balance and stability.36–38
Our study contributes to the limited research on dual-task performance and balance, specifically in severe COPD, a population with heightened disease severity and functional limitations. It provides evidence of the detrimental effects of COPD on dual-task abilities. Implementing dual-task assessments, such as the dual-task Timed Up and Go and SLS with a cognitive task, provides a more nuanced understanding of the challenges individuals with severe COPD face. These assessments, which simulate real-world scenarios requiring attention to both motor and cognitive demands, further underscore the importance of evaluating functional performance comprehensively.
The findings of our study have several implications for future research in the field of COPD and dual-task performance. First, the study highlights the need for further research to investigate the underlying mechanisms contributing to the impaired dual-task performance and balance in patients with COPD. This could include exploring the role of muscle weakness, respiratory muscle dysfunction, and other factors contributing to the observed impairments.
Our research has some limitations, including its cross-sectional design, which precludes the establishment of causal relationships. Another limitation is that we did not assess the impact of other factors that may affect dual-task performance and balance, such as cognitive impairment, depression, and anxiety. LTOT is a common treatment for patients with COPD, especially in severe and very severe stages, and it can significantly impact balance and functional mobility. Thus, the use of LTOT among patients with severe COPD may have introduced variability in the results. Future longitudinal studies could provide insights into the trajectory of dual-task performance and balance impairments in severe COPD.
Conclusion
This study highlights the significant impairments in dual-task performance and balance among patients with severe COPD. The results show that patients with severe COPD performed significantly worse in tests that involved dual-task and had poorer balance overall compared to healthy controls. This is evident from the longer times taken to complete the dual TUG test and the shorter times for the dual SLS test. Furthermore, we observed a significant positive correlation between dual-task interference in the TUG test and the fear of falling, indicating that patients with severe COPD who experience greater DTI are more likely to fear falling.