
Abstract
Long-term non-invasive ventilation (NIV) was introduced in the 1980s, initially mainly for patients with poliomyelitis, muscular dystrophy (MD) or scoliosis. The obesity-hypoventilation syndrome has since become the commonest reason for referral to most centres providing home-NIV. Patients with MD are numerically a much smaller part of the workload, but as their disease progresses the need for ventilatory support changes and they require regular comprehensive assessment of their condition. We have examined the trend in MD use of home-NIV in our unit over the last 25 years. The number of new referrals appears to be stabilizing at around 20–25 over a 5-year period, equivalent to approximately 0.5 per 100,000 of population per year. The mean age at commencement of home-NIV is now 37.5 years, with 5-year survival rates of 70–75%. Ten-year survival rates are just over 40%. The distance of usual place of residence from our unit is fairly stable, currently at a mean of 27 km. Excellent survival rates mean that patients with MD, while numerically small, are likely to remain an important part of the workload of centres providing home-NIV. Our data should prove useful in the planning of future services for this group of patients.
Introduction
Non-invasive ventilation, using positive airway pressure via a nose or face mask, was first developed in the 1980s. It rapidly became established as a valuable modality for patients with respiratory muscle weakness, correcting nocturnal hypoventilation and prolonging survival. 1,2 Many of these early patients had neuromuscular problems, such as muscular dystrophy (MD) or the sequelae of poliomyelitis.
We started providing home-NIV for patents with MD about 25 years ago. As with many home-NIV centres, in recent years the obesity-hypoventilation syndrome has become the commonest reason for referral. 3 (We also see large numbers of patients with more rapidly progressive neurological problems, such as motor neurone disease, and the number of referrals of patients with chronic obstructive pulmonary disease is steadily increasing.) Patients with MD are now a small minority of our patients, around 10% of the total number using home-NIV. They remain, nevertheless, an important group with specific requirements in terms of how their NIV is provided.
In order to plan future home-NIV services for MD patients, we have looked at referral patterns and survival rates over the last 25 years.
Methods
We defined adult MD as patients aged 18 years or over with a diagnosis of muscular dystrophy or spinal muscular atrophy. (During the period of the study, five patients were transferred from paediatric home-NIV services. These were not included in the analysis.)
We interrogated our database to see how many patients with MD were on home-NIV on 1st January in the years 1995, 2000, 2005, 2010 and 2015. We looked at how many had started home-NIV in the previous 5 years, their age and distance of usual place of residence from our unit. For each cohort, we calculated the 5- and 10-year survival rates (YSR).
Results
Table 1 shows the diagnoses of the 46 patients with MD using home-NIV on 1st January 2015. These diagnoses were based on a combination of clinical picture, muscle biopsy and genetic analysis: the “unclassified” group refers to those with a clear clinical picture of MD but inconclusive muscle biopsies and negative genetic tests. Twenty of the patients used cough-assist devices at home (an additional seven had lung volume recruitment bags) and five had implanted pacemaker/defibrillator units for cardiac dysrhythmias. On 1st January 2015, we had just under 500 patients in home-NIV, the MD group therefore representing around 10% of our workload. In addition to the home-NIV group, five patients with MD were managed with tracheostomy over the 25-year period of our study; in four of these, the tracheostomy had been performed prior to referral to our unit.
Diagnoses of patients with MD using home-NIV on 1st January 2015.
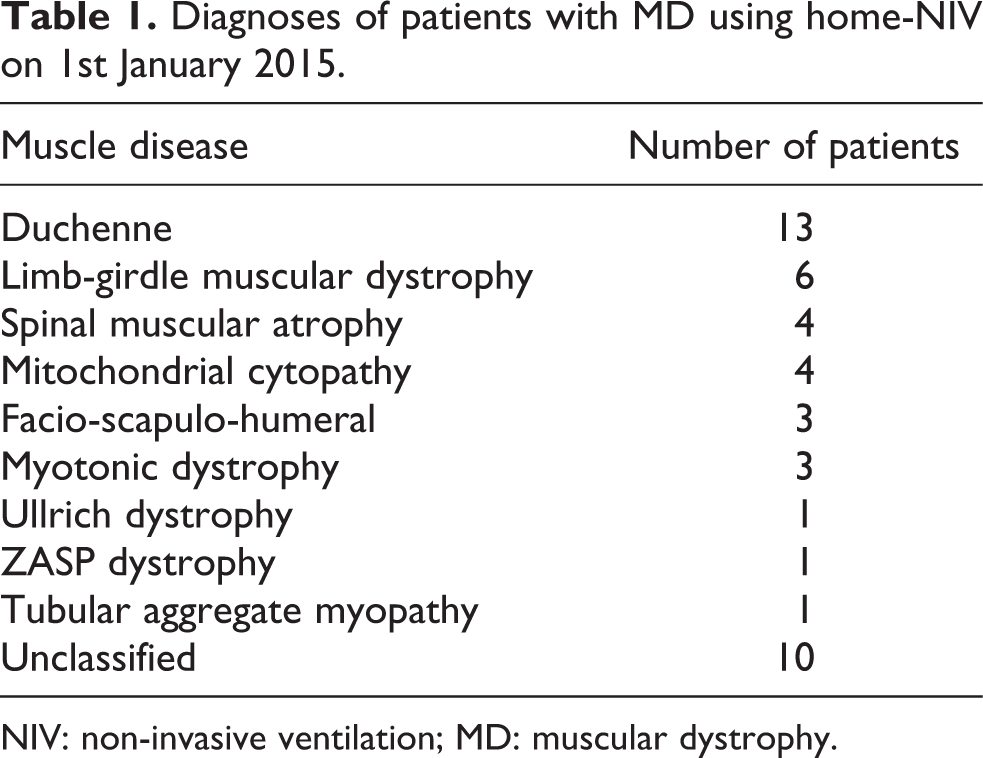
NIV: non-invasive ventilation; MD: muscular dystrophy.
Table 2 shows the number of MD patients started on home-NIV for each 5-year period of the study. The mean age and distance of residence from our unit are shown for each of these 5-year cohorts, together with their 5- and 10-YSR where this is available. The bottom line of Table 2 gives the total number of MD patients on home-NIV on each of the 5-year anniversaries.
Number of patients with MD started on home-NIV in a 5-year period, with age and distance of residence from our unit, together with the total number of MD patients at each 5-year anniversary.
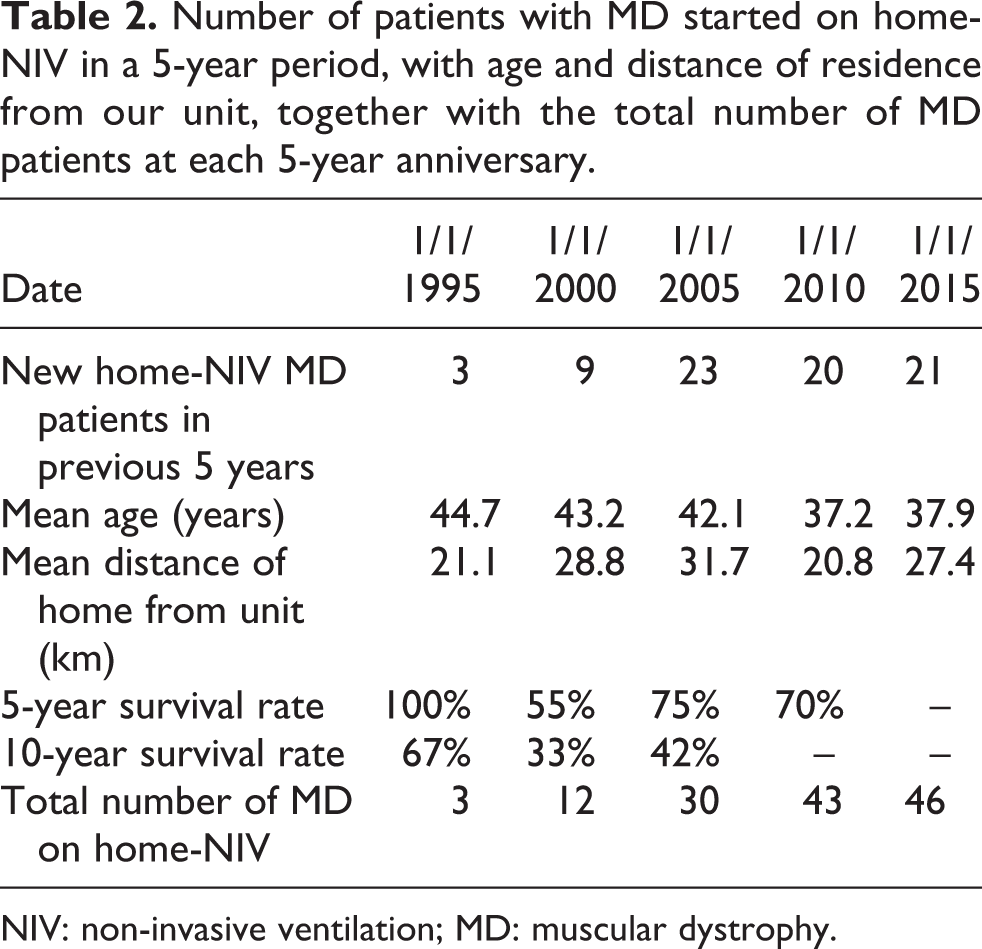
NIV: non-invasive ventilation; MD: muscular dystrophy.
Discussion
The number of new MD patients starting home-NIV each 5 years seems to be stabilizing at 20–25, equivalent to 4–5 patients per year. (A small number of MD patients were started on home-NIV but died or discontinued between one of our 5-year anniversaries.) We estimate our catchment population for this group of patients to be around 1 million, so five patients each year is equivalent to 0.5 per 100,000. This estimate is higher than the incidence figure of 0.2 per 100,000 which we derived previously from national death certification data. 4
Recent scientific advances allow more precise diagnoses of MD, but the background prevalence is unlikely to be changing. Moreover, there are as yet few therapeutic interventions which delay progression to ventilatory failure. We suggest that 0.5 per 100,000 population could be used with reasonable confidence in planning home-NIV services for MD. A prevalence of 100 children and adults with MD per 100,000 population is cited in the Walton report 5 ; while not all of these will require home-NIV, it remains a concern that there may still be patients with MD who would benefit from home-NIV but are not referred.
We excluded motor neurone disease, on the basis that the NIV requirements for this important but more rapidly progressive condition are different. We also excluded other neurological conditions (such as myasthenia gravis, multiple sclerosis, polymyositis and Guillain-Barre syndrome), on the grounds that they follow a less predictable course. We did not include post-poliomyelitis patients, since the number of new patients presenting is dwindling and the main aim of this study was to inform planning for the future provision of home-NIV.
As our service has matured, 5-YSR has settled at 70–75%. (Small numbers mean that the 5YSR for our early cohort is unlikely to be reliable.) This is in line with the figure of 73% published for Duchenne muscular dystrophy 6 and 81% for a mixed group of neuromuscular conditions including some patients with central hypoventilation. 7 Survival rates should improve with wider use of cough-assist devices and implanted defibrillators. With a 5YSR of 80%, four of five patients commencing home-NIV should be alive 5 years later. Ten YSR is more difficult to predict with confidence, given the small numbers in our study, but 40–50% would seem a reasonable estimate. The implication for a home-NIV service is that the number of MD will continue to rise for well over 10 years after new referral rates have stabilized.
We wondered if we might see a progressive reduction in the age of starting home ventilation, reflecting earlier recognition of MD, better liaison with paediatric services or earlier detection of respiratory complications as a result of regular screening. This appears not to be the case, with the mean age of starting home-NIV falling only slightly to just under 40 years, reflecting the diversity of MD. Duchenne muscular dystrophy are an important group, often starting to use home-NIV around the time to transition from paediatric to adult services, 6 but a home-NIV service must also plan for the care of other MD patients who develop respiratory problems much later in life. 8 –10 The low numbers of patients with myotonic dystrophy in our study reflects the challenges of successfully establishing long-term treatment NIV in this group. 11
Without a national register, we cannot be sure of the number of MD patients in our catchment area who are looked after by adjacent home-NIV centres, local services or national centres. Acute NIV services have been set up in all acute hospitals in our region over the period covered by the present study. These peripheral units are now providing home-NIV. We had anticipated that some MD patients would choose these local centres for their care, and that as a result the average distance our patients lived from our centre would fall. This appears not to the case to any great extent, possibly reflecting the location of the regional neurology service in our unit. It was noted in the Eurovent study that university hospitals had a higher proportion of neuromuscular patients. 12 Since MD patients choose to travel to a specialist centre, close liaison with neurology and other regional services is important in order to minimize the number of visits the patients make.
The Eurovent study also noted that neuromuscular patients, presumably mainly MD, were numerically the largest group of patients using home-NIV for more than 10 years. 12 While this may no longer be the case, following the epidemic of obesity-hypoventilation, we feel that MD patients are an important group of long-term users of home-NIV. Their ventilatory needs change as their respiratory muscle weakness progresses, which requires regular careful assessment of the patient, tailoring of home-NIV equipment and adjustment of care packages. A significant proportion will need cough-assist devices, which are likely to push survival rates even higher. We may also see more cardiac problems as a consequence of these patients living longer. Although some patients have progressed to ventilator dependence, our use of tracheostomy ventilation remains low. Many countries have much higher use of tracheostomy, 12 but we feel that our practice is consistent with the experience of others, 13 given the low prevalence of bulbar weakness in our patients.
Conclusions
Centres providing a regional NIV service should plan for 0.5 new MD patients per 100,000 of population. The excellent survival rates for this group mean that their numbers will continue to steadily increase. As their diseases progress, the equipment needs of this group will require funding. Many of these patients present in middle age, indicating the need for regular surveillance of respiratory function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.